

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute myocarditis is a rare inflammatory condition of the myocardium. The spectrum of presentation can range between mild myocardial dysfunction and fulminant congestive heart failure, which causes significant morbidity and mortality. However, because of its rarity, few large-scale epidemiological studies have reported acute myocarditis in children.1)2) Furthermore, no population-based epidemiological studies have been performed in Korea.
The Korean National Health Insurance (NHI) scheme is a public medical insurance system covering the entire Korean population. Under the NHI scheme, the Korean Health Insurance Review and Assessment Service (HIRA) evaluates the medical fees charged, the quality of care, and the adequacy of medical services rendered to each patient by recording data including diagnoses, treatments, procedures, and prescription drugs. In this study, we evaluated the 10-year (January 2007 through December 2016) epidemiological trends of acute myocarditis in Korean children by utilizing the HIRA database with the following objectives: 1) to describe the demographics of acute myocarditis in Korean children and, 2) to investigate temporal trends in the management of myocarditis in children.
Go to : 
METHODS
Sources of data and data selection
We analyzed the HIRA claims data of children and adolescents aged ≤19 years who were diagnosed with acute myocarditis between January 2007 and December 2016 (inclusive of December 2016 claims). We analyzed data with codes I40, I41, or I51.4, which indicate acute myocarditis based on the National Center for Health Statistics International Classification of Diseases, 10th edition (ICD-10).
Operational definition
In this study, children with “acute myocarditis” were defined as those who were hospitalized with primary diagnostic codes of I40, I41, or I51.4, based on the ICD-10 classification. We sub-classified this patient population into the “acute fulminant myocarditis (AFM)” and the “non-AFM” groups. According to the clinical criteria adapted from previous studies, that distinguish fulminant form of myocarditis by their history of rapid hemodynamic deterioration,3) we operationally defined “AFM” for those who required extracorporeal membrane oxygenation (ECMO) and/or mechanical ventilator support.
Statistical analysis
All database management and statistical analyses were performed using the SAS statistical software version 9.3 (SAS Institute, Cary, NC, USA). Categorical data were compared using the chi-square test or the Fisher exact test. Continuous data were analyzed using the independent t-test or the Wilcoxon rank-sum test. The annual trends in incidence were performed using the Cochran-Armitage's trend test. Estimated year-specific, age-specific, and sex-specific patient populations were standardized to the “Population in Korea 2010” obtained from the Statistics Korea website (http://www.kosis.kr). A p value <0.05 was considered statistically significant.
Go to :
RESULTS
Incidence rate
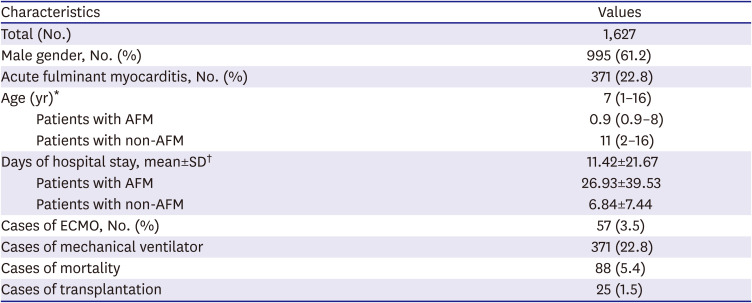
Using the Korean HIRA database, the records of 1,627 children were analyzed between January 2007 and December 2017. The overall incidence was 1.4 per 100,000 children in 2007 and 2.1 per 100,000 children in 2016. The annual incidence of acute myocarditis showed a significant increase in trends over time (Figure 1). There were 995 boys (61.2%) and 632 girls (38.8%); the incidence in 2016 was 2.5 per 100,000 boys and 1.7 per 100,000 girls, which indicated a significant sex difference (Figure 1). Overall, 6.9% (113/1,627) of the study population died (n=88) or heart transplanted (n=25). Of the 1,627 children with acute myocarditis, 371 children (22.8%) were diagnosed with AFM and needed ECMO (n=57) and/or mechanical ventilator support (n=371) (Table 1). The incidence rate of AFM showed an increasing trend over time; however, it showed marginal significance (p=0.0592).
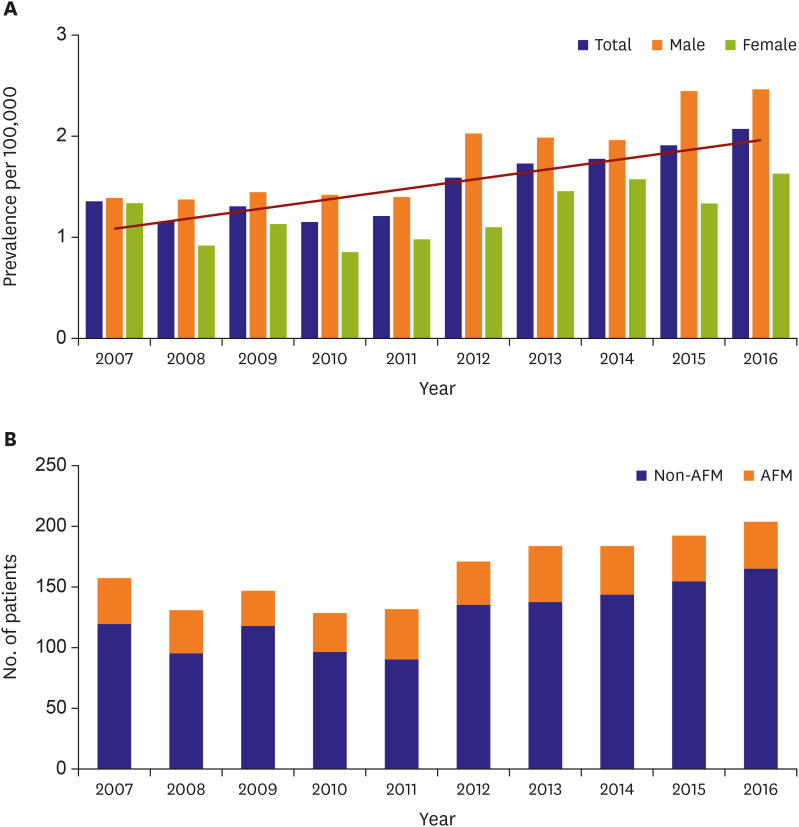 | Figure 1Incidence of acute myocarditis according to (A) sex, and (B) clinical manifestation in 2007–2016.
|
Table 1
Demographic characteristics of pediatric patients with myocarditis in National Health Insurance Service
Values are presented as number (%) or median (interquartile range) or mean±standard deviation.
AFM = acute fulminant myocarditis; ECMO = extracorporeal membrane oxygenator.
*p<0.0001; †p=0.001.
![]()
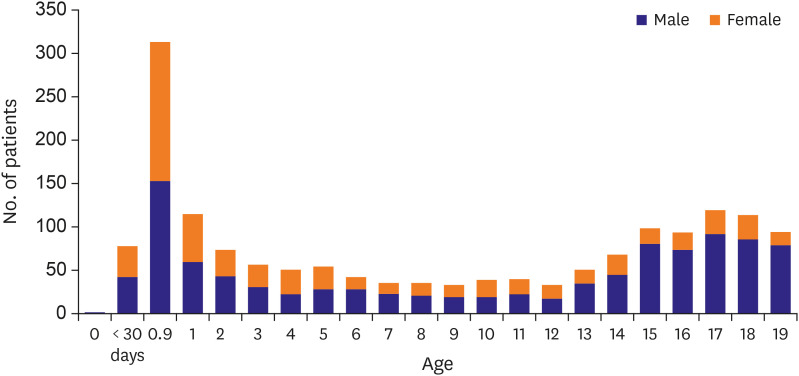
Age, sex, and seasonal distribution
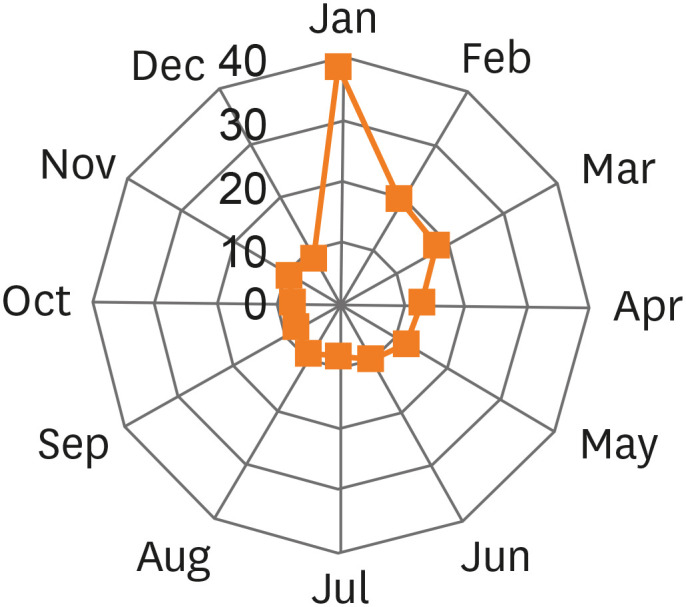
The mean age of children diagnosed with acute myocarditis was 8.52±6.97 years. A bimodal age distribution was observed with a peak in infancy and a smaller peak in the mid-teenage years. The sex distribution of children with acute myocarditis was significantly age-dependent (Table 1, Figure 2). Girls were younger than boys (mean age 6.49±6.33 years vs. 9.81±7.06 years, p=0.000), and a significant proportion of girls were diagnosed with acute myocarditis in <5 years of age. No sex difference was observed in the incidence rate of acute myocarditis in children aged ≤5 years (373 boys vs. 366 girls); however, the incidence rate in adolescents aged ≥13 years showed a significant male preponderance (482 boys vs. 152 girls). Figure 3 shows the seasonal variations in the occurrence of acute myocarditis—nearly 50% of all cases occurred between January and March (754 of the 1,627 cases investigated, 46.3%).
Acute fulminant myocarditis vs. non-acute fulminant myocarditis
To differentiate between AFM and non-AFM, we operationally defined “AFM” as “a state of acute myocarditis necessitating the use of a mechanical ventilator and/or ECMO support.” Of the 1,627 children investigated, the percentage of children with AFM was 371 of 1,627 children (22.8%). Table 2 shows the comparison between AFM and non-AFM. Children with AFM were younger than those with non-AFM (mean age 4.69±5.81 years vs. 9.65±6.89 years, p<0.0001). The percentage of children with AFM showed a peak at ≤28 days of age (52 of 79 neonates, 65.8%). However, this trend showed a decrease with increasing age (140 of 313 infants [44.7%], and 179 of 1,253 children aged ≥1 year [14.5%], p=0.000). Seven patients (3 AFM and 4 non-AFM) underwent endomyocardial biopsy (EMB). The rates of pacemaker implantation (9.1% vs. 2.1%, p<0.0001), pericardiocentesis (1.8% vs. 0.5%, p=0.023), and heart transplantation (3.2% vs. 0.9% p=0.006) in the AFM group were significantly higher than those in the non-AFM group. Additionally, the use of amiodarone (32% vs. 2.3%), intravenous immunoglobulin (IVIG) (94% vs. 27.2%), and steroid (33.9% vs. 7.5%) was significantly higher in children with AFM than in children with non-AFM (p for all <0.0001).
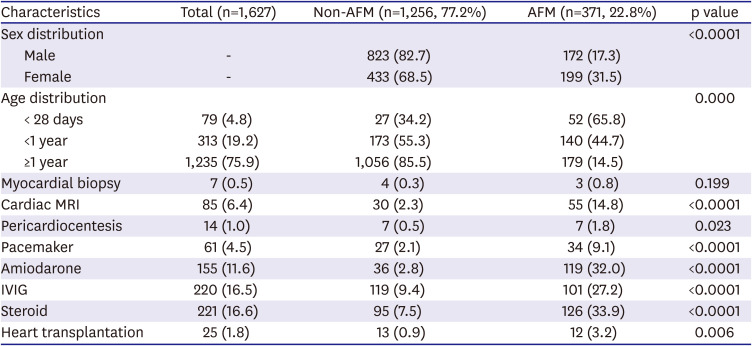
Table 2
Comparison of patients based on clinical manifestation
Values are presented as number (%).
AFM = acute fulminant myocarditis; IVIG = intravenous immunoglobulin; MRI = magnetic resonance imaging.
![]()
Management and outcomes of acute fulminant myocarditis
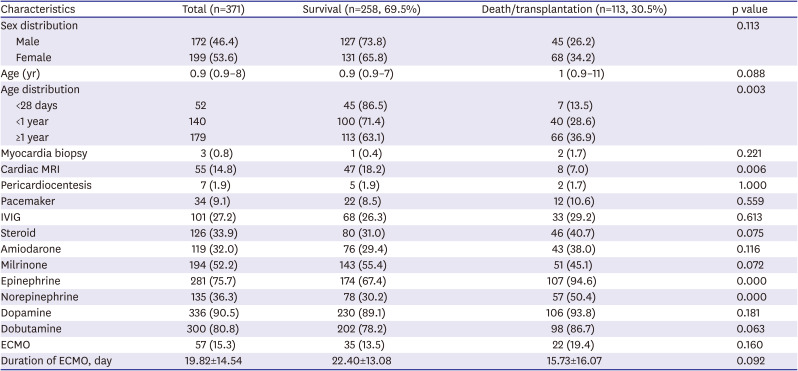
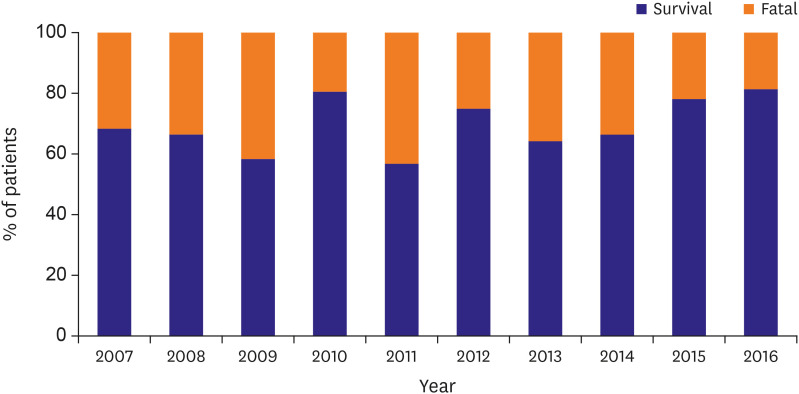
Children with AFM (n=371) were further stratified into 2 groups based on outcomes (death or heart transplantation vs. survival) as shown in Table 3. Of the 371 children with AFM, 258 (69.5%) survived. The outcome was significantly age-dependent—the survival rate of neonates was 86.5% in contrast to 63.1% in those aged ≥1 year (p=0.003). ECMO was required in 57 of 371 children (15.3%). The survival rate in those treated with ECMO was 35 of 57 children (61.4%). The initiation of ECMO did not significantly affect the outcome. The administration of IVIG and steroids did not significantly affect the outcome. Additionally, the administration of dopamine, dobutamine, or milrinone did not significantly affect the outcome. Notably, only MRI was significantly associated with lower mortality/transplantation. (18.2% in the survivor vs. 7.0% in the fatality group, p=0.006). The survival rate of children with AFM remained nearly identical over the 10-year study period (Figure 4). We observed an increase in the use of ECMO (p<0.0001), in the rate of EMB (p=0.0045), and in the administration of IVIG (p=0.0003) and steroid (p=0.0011) and a decrease in the use of dopamine (p=0.0014) and dobutamine (p=0.0098) over the study period (Figure 5).
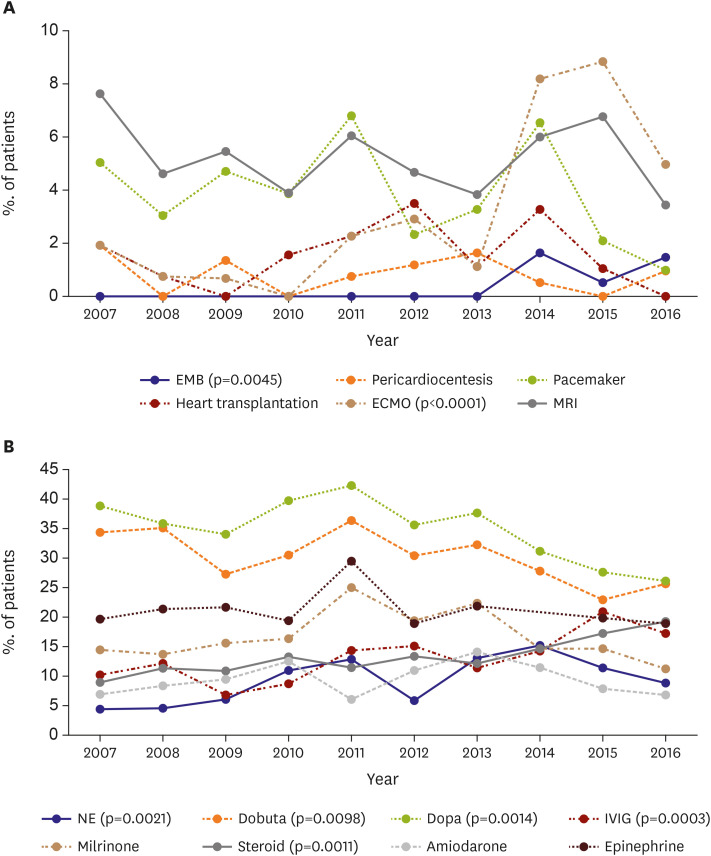 | Figure 5Temporal trends in (A) care requirements, and (B) medications in acute myocarditis. ECMO indicates extracorporeal membrane oxygenation.ECMO = extracorporeal membrane oxygenation; EMB = endomyocardial biopsy; IVIG = intravenous immunoglobulin; MRI = magnetic resonance imaging; NE = norepinephrine.
|
Table 3
Comparison of patients with acute fulminant myocarditis (n=371) based on outcome
Values are presented as number (%) or median (interquartile range) or mean±standard deviation.
ECMO = extracorporeal membrane oxygenator; IVIG = intravenous immunoglobulin; MRI = magnetic resonance imaging.
![]()
Go to :
DISCUSSION
Previous research investigating epidemiology of pediatric myocarditis was based on Western population.1) Our study is the first nationwide epidemiological study to investigate acute myocarditis in Korean children. Furthermore, our study provides comprehensive data regarding the demographic features and management of acute myocarditis in children over a 10-year period.
Several studies have reported the incidence of acute myocarditis in children. A nationwide study in Finland reported an incidence rate of 1.95 cases/100,000 person-years in children aged 0–15 years.1) A Japanese study (based on questionnaires mailed to teaching hospitals) reported an incidence rate of 0.26 cases per 100,000 populations among children and adolescents aged 1 month–17 years.2) Notably, the reported incidence rate varies significantly across studies,4)5) and the true incidence rate of acute myocarditis in children remains unknown. In this nationwide study, we observed that the predicted annual incidence rate of acute myocarditis in children and adolescents aged ≤19 years was approximately 2 cases/100,000 populations in Korea, which was nearly similar to the recent nationwide study performed in Finland.1) We also observed that the incidence rate of acute myocarditis in children showed an increase over the 10-year study period. This increase in the incidence rate might be attributed (at least partially) to increased awareness of acute myocarditis among Korean physicians.
In this study, we observed a “bimodal age distribution” of acute myocarditis in children. Several previous studies have shown a bimodal age distribution with peaks during infancy and the mid-teenage years.1)6) Interestingly, the age distribution in our study showed a remarkable peak during infancy in addition to a smaller peak during adolescence, which differed slightly from the patterns observed in the studies performed in the United States (US) or in Finland.1)6) Notably, the age distribution observed in our study is nearly similar to that reported by Japanese studies.2) The difference in the age distribution between Westerners and Asians has not been adequately discussed by previous studies. Therefore, no definitive conclusions can be drawn in this context. Nevertheless, it would be reasonable to consider the role of regional or racial variations.
Interestingly, the children included in this study showed a significant age-dependent sex distribution. No sex difference was observed in the incidence rate of acute myocarditis in children aged ≤5 years; however, the incidence rate in adolescents aged ≥13 years showed significant male preponderance. Although a few contradictory results have been observed with regard to the age- and sex distribution trends,7)8) several previous studies have also reported similar male preponderance in adolescents.1)6)9) The exact cause for the sex difference is unclear. Several experimental studies support the role of sex hormones in the occurrence of myocarditis in that estrogens have been shown to protect against myocarditis.10) Thus, the increase in the incidence rate among adolescent males in the present study may be attributed to the increasing levels of testosterone in this patient population. However, in addition to the influence of sex hormones, complex genetic and sex chromosome–related factors and as yet unknown genetic variations might play key roles in the occurrence of myocarditis.10)11)
We also investigated the seasonal pattern of acute myocarditis. A previous study performed in Finland reported that the incidence of acute myocarditis was the highest between September and December.1) We also observed a prominent seasonal variation in that nearly 50% of the cases presented between January and March in our Korean population. Acute myocarditis is primarily a viral infection; thus, this prominent seasonal variation may be explained by this etiology.
Notably, in this study, the survival rate in neonates with AFM was significantly better than that of older children; there is a possibility that transient myocardial dysfunction in neonates with ventilator support may have included and influenced the result. Clinical features of acute myocarditis vary, and AFM differs from non-AFM in terms of the aggressive and fulminant presentation of the former. Previous studies reported that the incidence of AFM may constitute approximately 10%–38% of all cases of acute myocarditis.12)13) In our Korean population-based study, we observed that 22.8% of children with AFM received ECMO and/or mechanical ventilator support. Compared with the excellent overall survival rate of acute myocarditis (1,514 of 1,627 children, 93%), the survival rate of children with AFM was poor (69.1%), and this finding concurred with earlier reports.2) However, the recent study in Finland reported a much higher survival rate of 84.6% in children with AFM.1)
In this study, 32% of children with AFM needed amiodarone, and 9.1% of children with AFM required temporary pacemaker support. We admit that these data cannot represent the prevalence of whole kind of arrhythmias in children with myocarditis, yet it showed that clinically significant tachyarrhythmias which need medication or bradyarrhythmias which need pacemaker treatment are common complications of AFM in children. Similar with previous reports, death or heart transplantation seems not directly attributed to the arrhythmias (p=0.116 for amiodarone; p=0.559 for pacemaker).14)15)
Those with AFM frequently tend to progress to refractory heart failure and require rescue intervention with mechanical circulatory support, like ECMO, which is the most common form of mechanical support used in children with myocarditis.16) Despite serious risks associated with ECMO therapy, such as bleeding, brain injury, and limb ischemia, it is considered as the most important life-saving option in patients with severe, life-threatening AFM. In our study, 15.4% of children with AFM received ECMO support. A previous study reported that ECMO was initiated in approximately 17% of the children who were hospitalized with myocarditis.17) Another study in US that used the Pediatric Health Information System database reported that ECMO was initiated in 18.9% of children hospitalized with myocarditis.6) The rate of ECMO use in our study was slightly lower than that in previous studies. Furthermore, the utilization of ECMO did not provide significant survival benefit in our study: 57 of the 371 children with AFM (15.3%) received ECMO support, and 22 of these 57 children (38.5%) died during hospitalization. In many centers, ECMO was considered as last-resort rescue therapy after unsuccessful trials of other modalities, therefore, timely ECMO initiation seems not always take place; therefore, the lack of timely initiation of ECMO might contribute (at least partially) to this unsatisfactory result. The importance of early ECMO treatment in the survival of children with AFM was recently demonstrated by Jung et al.18); they reported an outstanding survival rate (92.3%) in children with AFM who managed by early ECMO treatment strategy.
Based on the belief, that an autoreactive cellular and humoral immune response triggered by viral infection may be responsible for the myocardial inflammation, immunosuppressive therapies including corticosteroids or immunoglobulin continue to be widely used to treat acute myocarditis in children.6)19)20)21) Similar with previous studies, immunosuppressive agents were commonly used to treat acute myocarditis in our study population (IVIG 27.2%, and corticosteroids 33.9% in children with AFM). An increasing trend was observed in immunosuppressive agents use during the study period (IVIG, p=0.0003; corticosteroids, p=0.0011). However, no significant survival benefit was observed, which was consistent with many previous studies.22)23) Nonetheless, it is worthy of attention, that significant improvement in LVEF or LVEDD was noticed in the IVIG group in their studies. A focused trial enrolling children with severe viral myocarditis is crucial to determine the true benefit of IVIG in this group of patients.
The limitations of our study are as follows: 1) The retrospective study design is a drawback of this study. 2) Errors related to possible coding inaccuracy cannot be excluded. Besides, it is unclear what diagnostic criteria were used to label children as having myocarditis with such databases designed for cost claim issues. Further studies using either hospital-based medical records or prospective studies are required. 3) The incidence of acute myocarditis may have been under- or over-estimated in children presenting with acute myocarditis and concomitant clinical conditions such as sudden cardiac death in outpatient clinics or emergency departments. 4) Data related to etiological factors, and long-term follow-up outcomes were unavailable. Despite these limitations, the present study is clinically important because this was a large-scale study in a real-world setting that utilized data from the national database. Additionally, no selection bias was observed.
This is the first nationwide study to investigate the epidemiology and management of acute myocarditis in children in the entire Korean population. In this study, we observed an increase in the incidence of acute myocarditis in children over the last decade. To date, there is a lack of consensus regarding the management of acute myocarditis in children.24) However, in our view, this study could serve as the backbone for future clinical trials and nationwide strategy planning for the management of acute myocarditis in children.
Go to :
 XML Download
XML Download