

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic diseases, including cardiometabolic disease (cardiovascular disease and diabetes mellitus) and cancer, are major causes of morbidity and mortality worldwide [1]. It is estimated that 25.4 million deaths, equivalent to 46% of all-cause mortality, in the world population occur annually due to cardiometabolic disease and cancer [2]. Over the past several decades, the prevalence of cardiometabolic disease and cancer has increased in all parts of the world, including countries with traditionally low prevalence, partially due to economic development and westernized lifestyles. Some countries, including Korea, have experienced extremely rapid economic development and dramatic shift in lifestyles. In these countries, the distribution and associated burden of diseases have also shifted from communicable to noncommunicable diseases. For example, in Korea, cardiometabolic disease and cancer contributed to 149,924 deaths (53% of all deaths) in 2016 [3], an increase of 25% since 1998.
Among the risk factors for cardiometabolic diseases and cancer, dietary factors, such as suboptimal intakes of fruits, vegetables, nuts and seeds, and whole grains, have been reported to substantially contribute to the burden of cardiometabolic disease and cancer [45]. A previous global burden of diseases (GBD) Study reported that eight of the top 20 risk factors for lost global disability-adjusted life-years (DALYs) were dietary factors [6]. Other studies [78910], using the comparative risk assessment (CRA) method, have also highlighted the impact of dietary risk factors on mortality from chronic disease by quantifying the country- and regional-specific disease burdens attributable to individual dietary factors. CRA is a useful tool for estimating the disease burden attributable to specific factors and synthesizing evidence that informs policy priorities [11]. However, most CRA studies to date have been conducted in European populations [12], and there is limited information from Asian populations, which have undergone substantial changes in dietary patterns over the past decades. A recent study from China [13] reported moderate improvements in consumption of refined grains, fruits, and nuts and seeds and unfavorable changes in consumption of processed meat and sugar-sweetened beverages from 1982 to 2012, suggesting a shift in nutrition intervention and policy priorities for chronic disease prevention over time in China. We previously reported the associations between six dietary factors (fruits, vegetables, whole grains, processed meat, red meat, and sodium) and the burden of cardiometabolic disease mortality from 1998 to 2011 in Korea [14]. In that study, high intake of sodium and low intakes of fruits and whole grains were found to be responsible for the highest number of deaths from cardiometabolic diseases during the study period [14]. Extending earlier studies [1415], the present study examined the impact of nine dietary risk factors (fruits, vegetables, whole grains, processed meat, red meat, nuts and seeds, milk, sugar-sweetened beverages, and calcium), individually and collectively, on the burden of cardiometabolic disease and cancer mortality among Korean adults using nationally representative, repeated cross-sectional survey data from 1998 to 2016. This study differs from the previous reports [1415] by extending the CRA analysis to more comprehensively examine the secular trends of nine dietary factors over a longer period. We also quantified the mortality from cancer, as well as cardiometabolic diseases, attributable to nine selected dietary factors to provide evidence to inform nutritional policy priorities and identify the principal drivers of the burden.
SUBJECTS AND METHODS
We performed a population-level CRA analysis to evaluate the contribution of nine dietary risk factors to the burden of cardiometabolic disease and cancer mortality among Korean adults aged 25 years and older. Detailed descriptions of the CRA methodology have been presented previously [11]. For each of the individual dietary risk factors, we estimated the number and proportion of cardiometabolic and cancer deaths that would have been avoided during the period of analysis if the observed distribution of intake levels had been changed to a hypothetical alternative distribution, called the theoretical minimum-risk exposure distribution (TMRED).
Data sources
For this analysis, we obtained the following information: the intake levels of nine dietary risk factors from the Korea National Health and Nutrition Examination Survey (KNHANES) 1998, 2001, 2007–2016; the TMREDs of dietary factors from previous GBD studies [16]; estimates of the relative risk (RR) for the dietary risk factors and disease relationships from previous meta-analyses [1718]; and the number of disease-specific deaths from the Korean Statistical Information Service (KOSIS), as detailed below.
Intake levels of dietary risk factors
We selected the following nine dietary factors (eight food groups and one nutrient) with probable or convincing evidence for their relationships with cardiovascular disease, diabetes mellitus, and cancer: low intakes of fruits, vegetables, whole grains, nuts and seeds, milk, and calcium and high intakes of unprocessed meat, red meat, processed meat, and sugar-sweetened beverages. We obtained information on the intake levels of the nine dietary factors from KNHANES. The details of KNHANES are described elsewhere [19]. Briefly, KNHANES is a nationally representative cross-sectional survey conducted by the Korea Centers for Disease Control and Prevention and the Ministry of Health and Welfare in 1998, 2001, 2005, and annually since 2007. All subjects included in the survey were selected using a stratified multistage clustered probability sampling design based on geographic area. All surveys collected comparable data using similar designs and sampling methods. Dietary information was assessed by single-day 24-hour recall and semiquantitative food frequency questionnaire (FFQ) (using a 63-item questionnaire before 2012 and a 112-item questionnaire since 2012), which were quantified using the Korea Food Composition Table. To examine temporal trends in dietary intakes across years, we used all KNHANES data collected to date (1998–2016) except the third KNHANES data (2005) which included extreme outliers. Because the same FFQ was not consistently used across the study period and the assessment was limited to population aged < 65 years, we used data from 24-hour recall in our primary analysis. Further, 24-hour recall may be better than the FFQ at estimating absolute intake levels of a large population. We used FFQ data only in the sensitivity analysis. We limited our analysis to participants who completed the nutrition survey. We excluded data from participants with implausible intake values of total energy (< 500 kcal or > 5,000 kcal per day) and of individual dietary factors (intake levels ± 3 standard deviation from the mean). We also excluded data from participants who reported consuming rice less than once per day, as this was considered implausible for Korean adults. The Institutional Review Board of the Korea Center for Disease Control and Prevention reviewed and approved the data of KNHANES (2007-02CON-04-P, 2008-04EXP-01-C, 2009-01COM-03-2C, 2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2C, 2013-07CON-03-4C, and 2013-12EXP-03-5C).
Counterfactual distribution of dietary risk factors
The TMRED values for each dietary factor were defined as the recommended intake levels at which they would yield the greatest beneficial effects or be associated with the lowest level of harm based on previous CRA studies (Table 1) [16].
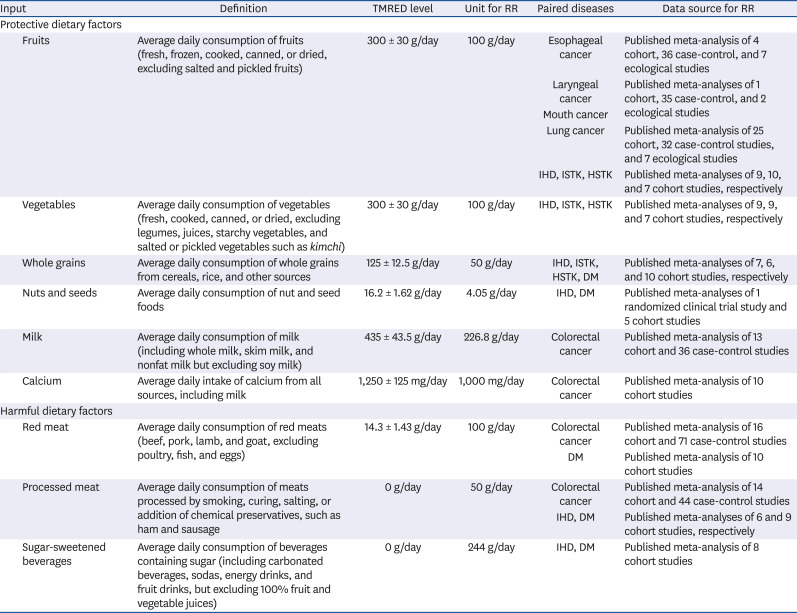
Table 1
Data sources and descriptions of dietary factors, optimal intake levels, and associations with paired diseases
TMRED, theoretical minimum-risk exposure distribution; RR, relative risk; IHD, ischemic heart disease; ISTK, ischemic stroke; HSTK, hemorrhagic stroke; DM, diabetes mellitus.
![]()
Relationships between risk factors and disease
The disease outcomes included in this study were ischemic heart disease (IHD), ischemic stroke (ISTK), hemorrhagic stroke (HSTK), diabetes mellitus, and cancers (including gastrointestinal and respiratory tract cancer, mouth cancer, esophageal cancer, stomach cancer, colorectal cancer, laryngeal cancer, and lung cancer) that are known to be related to diet. The RR estimates were obtained from published systematic reviews, meta-analyses of randomized controlled trials, and observational studies [182021]. Details of the data sources are provided in Table 1.
Disease-specific deaths
Cause-specific mortality counts were extracted from the KOSIS, which provides official statistics on mortality from 236 causes for both sex in 5-year age groups for each year. The causes of mortality were coded according to the International Classification of Disease (ICD), 10th revision. In the present study, we limited the analysis to data on deaths from diabetes mellitus (E10–E14), IHD (I20–I25), ISTK (I63 and I67), HSTK (I60–I62), mouth cancer (C00–C14), esophageal cancer (C15), stomach cancer (C16), colorectal cancer (C18), laryngeal cancer (C32), and lung cancer (C34).
Statistical analyses
To evaluate secular trends in consumption levels of dietary factors, we calculated the mean and standard deviation of the consumption of each dietary factor according to sex, age, and year after applying sampling weights and adjusting for total energy intake using the residual method. Assuming that the effect size estimates (RRs) for each risk factor reflect causal relationships with cardiometabolic and cancer mortality in the study population, we also estimated the expected proportional reductions in mortality in the population by calculating the population attributable fraction (PAF) for each dietary risk factor using the following equation:

where x is the level of exposure, m is the maximum exposure level, P(x) represents the observed age- and sex-specific population distribution of the exposure, P′(x) is the counterfactual or optimal distribution of the exposure, and RR(x) is the age- and sex-specific RR of the mortality or incidence at exposure level x. The PAF for the combined dietary factors was derived from each PAF using the following equation [13]: combined PAF = 1 − ∏Rr=1(1 − PAFr), where r is each individual dietary factor and R is the number of dietary factors. To estimate the number of disease-specific deaths attributable to risk factors, PAFs computed as above were multiplied by the number of disease-specific deaths. All analyses were conducted separately by sex and age groups (25–34, 35–44, 45–54, 55–64, 65–74, and ≥ 75 years) from 1998 to 2016. We then aggregated the age- and sex-specific values to estimate the total number of deaths attributable to dietary risk factors. To assess the uncertainty for the attributable deaths, we applied a Monte Carlo simulation to each risk factor. We iterated this simulation procedure 1000 times for each risk factor and finally generated 1,000 mortality estimates for each sex and age group. We then derived the mean and 95% uncertainty intervals (UIs) bounded by the 2.5th and 97.5th percentiles of the 1000 iteration values. To assess the trend of temporal changes across the years, Cuzick's nonparametric trend test was used [22]. All statistical analyses were performed with STATA, version 13.0 (StataCorp, College Station, TX, USA) and R software, version 3.5.1 (http://www.R-project.org).
Sensitivity analysis
Recognizing the differences in the intake levels of dietary factors assessed by two dietary assessment methods (FFQ and 24-hour recall), we performed sensitivity analyses that repeated the CRA analysis using the data from semiquantitative FFQs from 2012 to 2016, which included 112 items in which the subjects were asked to report how often they consumed each food item during the past 12 months on a nine-point scale (3 times per day, twice per day, once per day, 5 or 6 times per week, 2 to 4 times per week, once per week, 2 or 3 times per month, once per month, less than once per year, or almost never). The responses were converted into daily consumption amounts by multiplying by the serving sizes provided by the Korea Rural Development Administration (KRDA) guideline [23]. Because FFQs were conducted only in participants aged < 65 years, we compared the two survey methods among participants aged 25 to 64 years. To increase the comparability, we restricted the comparisons to food items that were assessed by both methods.
RESULTS
Secular trends in intake levels of dietary risk factors across years
As shown in Table 2, the intake levels of all dietary factors evaluated increased from 1998 to 2016, except for calcium. In particular, among protective dietary factors, the level of dietary intake increased by 165% for nuts and seeds (4.5 vs. 1.7 g/d) and 91% for whole grains (10.9 vs. 5.7 g/d). However, the intakes of these items remained far below the TMREDs (16.2 g/d for nuts and seeds and 125 g/d for whole grains). The intake level of fruits slightly decreased from 1998 to 2008 (140.0 vs. 164.2 g/d) but increased after 2008 (192.1 vs. 140.0 g/d). Among harmful dietary factors, the intake levels of processed meat and sugar-sweetened beverages increased the most during the same time period. Overall, there were no sex-specific differences in the distribution of dietary intakes. When we compared intakes by age group, more unfavorable changes were generally observed in the youngest age group (25–44 years) than in the older age groups (45–64 and ≥ 65 years). The intakes of protective factors such as fruits, vegetables, and calcium decreased in the youngest age group and increased in other age groups. Processed meat intake increased more dramatically in the youngest age group than in older age groups.
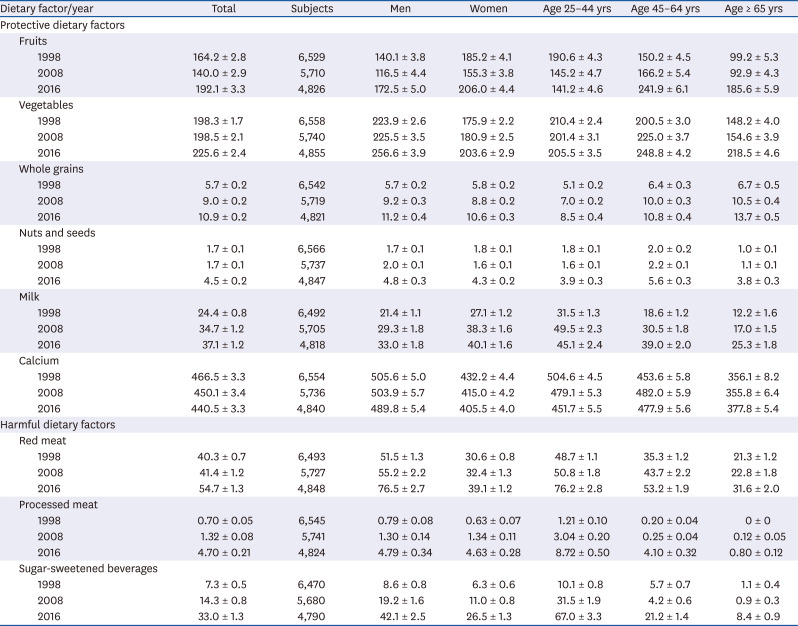
Table 2
Mean and standard error of intake levels of nine individual dietary factors according to sex and age in 1998, 2008, and 2016
Values for mean intake levels and corresponding standard errors were combined across sex and/or age groups.
![]()
Secular trends in cardiometabolic and cancer mortality by age, sex, and year (data not shown)
The number of deaths related to chronic disease (for a total of 738,209 deaths from 1998 to 2016: 435,219 in men and 302,990 in women), including IHD (156,457 deaths: 83,660 in men and 72,797 in women), stroke (186,521 deaths: 96,511 in men and 90,010 in women), diabetes mellitus (126,920 deaths: 63,927 in men and 62,993 in women), and cancer (268,311 deaths: 191,121 in men and 77,190 in women), increased by 34% (16,309 deaths) from 1998 to 2016. A substantial increase in IHD mortality (14,646 vs. 7,601 deaths) was the major cause of an exceptionally high rate of nonaccidental deaths during the study period. Women had a much greater proportional increase in IHD mortality than men (115% vs. 77%). The total number of nonaccidental deaths declined among adults aged < 65 years (14,583 vs. 19,114 deaths) and increased among those aged ≥ 65 years (49,728 vs. 28,888 deaths).
Population attributable fractions and absolute attributable deaths according to dietary factors by year
During the period of analysis, low intakes of fruits and whole grains consistently ranked as the top dietary contributors to the cardiometabolic and cancer mortality burden in Korea (Fig. 1). Although the contribution of fruit intake was reduced after 2008 (P for trend = 0.003), suboptimal intake of fruits remained the largest contributor in 2016, accounting for 7,067 attributable cardiometabolic disease and cancer deaths (95% UI = 6,180.2–7,940.4) in total. Fruit intake was followed by intakes of whole grains and vegetables, which accounted for 4,372 (95% UI = 3,456.2–5,284.9) and 2,338 deaths attributable to cardiometabolic disease and cancer (95% UI = 1,875.6–2,821.5), respectively. Whereas deaths attributable to suboptimal intakes of fruits, whole grains, and vegetables showed overall decreasing trends, deaths attributable to other factors (nuts and seeds, calcium, milk, red meat, processed meat, and sugar-sweetened beverages) increased during the study period. The PAFs generally showed similar patterns for the number of deaths related to dietary risks, except for calcium and milk intakes. During the period of analysis, calcium and milk intakes showed little change in PAFs, but the number of deaths attributable to low calcium and milk intakes increased. The total numbers of deaths attributable to an overall suboptimal diet were 17,849, 20,904, and 17,557 in 1998, 2008, and 2016, representing PAFs of 37%, 34%, and 27%, respectively.
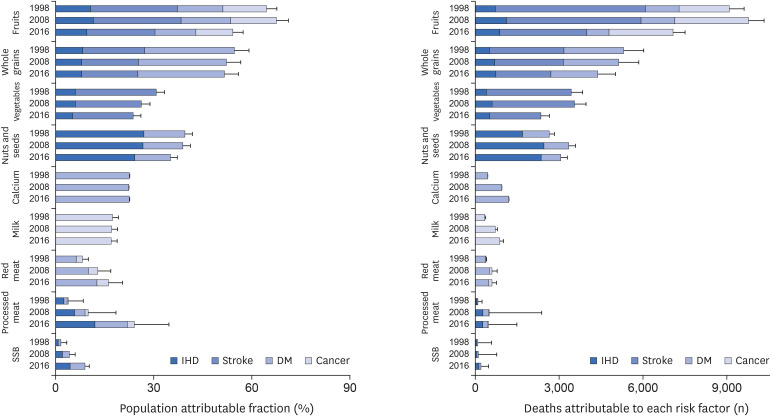
Fig. 1
Population attributable fractions and attributable cardiometabolic and cancer deaths by individual dietary risk factors in 1998, 2008, and 2016.
The error bars represent the standard deviations of the number of deaths from each risk factor. The error bar for the standard deviation of the estimate derived from the low intake of calcium is not visible.
IHD, ischemic heart disease; DM, diabetes mellitus; SSB, sugar-sweetened beverages.
![]()
Stratification by sex, age, and disease
Although the absolute and proportional cardiometabolic and cancer mortality associated with individual dietary factors did not differ between men and women, the patterns varied by age group (Fig. 2, Supplementary Table 1). For all individual dietary factors and for all diseases, younger populations tended to have greater PAFs associated with suboptimal consumption (Fig. 2). For processed meat and sugar-sweetened beverages, the PAF gaps among the age groups gradually widened over the years. In particular, the PAFs for processed meat intake associated with IHD, diabetes mellitus, and colorectal cancer in the youngest age group (25–34 years) rapidly increased from 13.0% in 1998 to 43.8% in 2016 (P for trend = 0.002) and were much higher than those for older age groups.
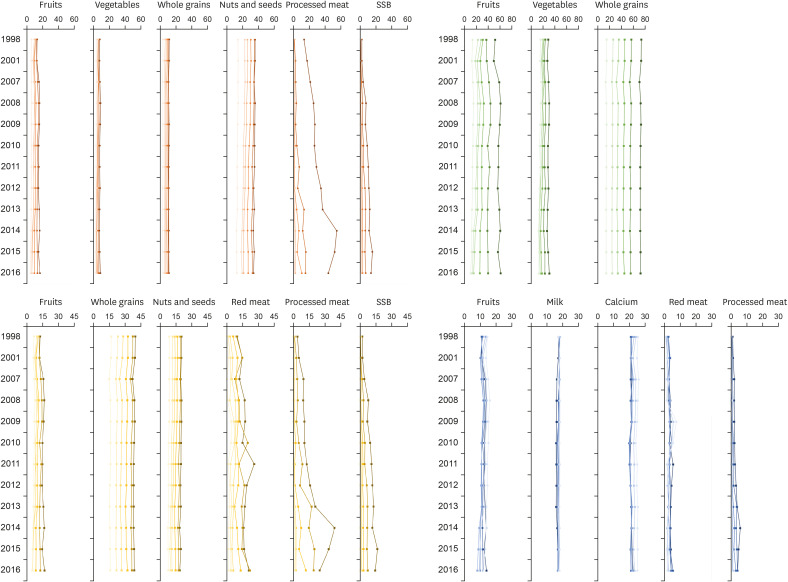
Fig. 2
Population attributable fractions of the individual risk factors across years stratified by age group.
The estimated population attributable fractions of each risk factor to its related diseases were divided into six groups by age: 25–34 years, 35–44 years, 45–54 years, 55–64 years, 65–74 years, and 75 years and older. Darker colors indicate younger age groups. Orange lines indicate ischemic heart disease, green lines stroke, yellow lines diabetes mellitus, and blue lines cancer.
SSB, sugar-sweetened beverages.
![]()
However, because the baseline number of deaths is higher in the older age groups, the absolute number of attributable deaths was greater in the older age groups (Supplementary Table 1). Among the population aged 25 to 44 years, the number of attributable deaths increased for fruit intake and decreased for intakes of milk and red meat over the years. However, in the older age groups, changes in the opposite direction were observed. Further, the number of deaths from low intakes of whole grains and nuts and seeds increased only in the population aged ≥ 65 years.
Comparison of two dietary assessment methods
For whole grains and milk, we observed similar results from the two dietary assessment methods (24-hour recall and FFQ) (Fig. 3). For vegetables, nuts and seeds, processed meat, and sugar-sweetened beverages, we observed similar results when comparisons were made with restriction to food items presented in both methods. However, for red meat intake in all years and fruit intake in recent years, the results from 24-hour recall data were markedly different from those from the FFQ. Compared with the results from the FFQ, PAFs and attributable deaths estimated from 24-hour recall data tended to be lower for protective dietary factors but higher for harmful dietary factors.
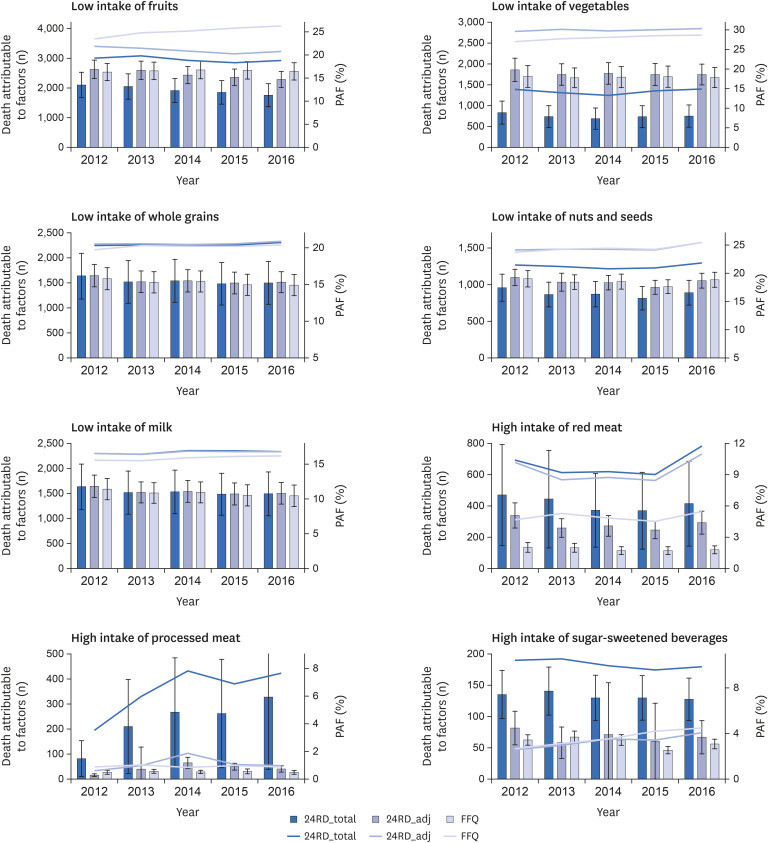
Fig. 3
Comparison of population attributable fraction and total disease burden due to each risk factor by year.
24RD_total indicates that the 24-hour recall data included all food items used for the analyses. 24RD_adj indicates that the 24-hour recall data included only food items that were also included in the FFQ for the analyses. Error bars represent standard deviations. Bar graphs represent the number of deaths attributable to each factor. Line graphs represent the PAF for each factor.
FFQ, food frequency questionnaire; PAF, population attributable fraction.
![]()
DISCUSSION
This study examined the nutrition transition and the associated burdens of cardiometabolic diseases (cardiovascular diseases and diabetes mellitus) and cancer mortality in Korea from 1998 to 2016 using the CRA framework. The study reported important findings. First, among the nine dietary risk factors evaluated, the leading contributors to high cardiometabolic and cancer mortality were low intakes of fruits and whole grains. Despite recent improvements in intake levels of fruits and whole grains, deaths attributable to these factors remained high, as the intake levels remained far below the optimal levels. Second, deaths attributable to low intakes of nuts and seeds, calcium, and milk and high intakes of red meat, processed meat, and sugar-sweetened beverages continuously increased since 1998. Finally, the total number of deaths from chronic diseases attributable to all dietary factors combined was 231,148 (49,430 IHD deaths, 87,060 stroke deaths, 46,291 diabetes mellitus deaths, and 48,367 cancer deaths), accounting for nearly 31% of chronic disease mortality during the study period. Our data suggest that these dietary risk factors may be important targets for chronic disease prevention in Korea.
Consistent with previous findings [121415], our data showed that low consumption of fruits and whole grains made the greatest contribution to cardiometabolic and cancer mortality in Korea from 1998 to 2016. A prior GBD study identified a diet low in fruits and whole grains as the world’s leading contributor to all-cause mortality in 2015 [21]. This finding is also consistent with earlier CRA studies conducted in Koreans using diet information obtained from the FFQ in the KNHANES in 1998 to 2011 and from 2012 to 2013 [1415]. These studies have shown that, among the dietary factors evaluated, suboptimal intakes of fruits and whole grains consistently ranked as the top contributors to cardiometabolic deaths during the study period [1415]. In the present study, we used the same national survey data (KNHANES) but examined the longer-term nutritional transition using 24-hour recall data from the first KNHANES (1998) to the latest KNHANES (2016). Further, our analysis included people aged ≥ 65 years to evaluate the nutritional transition in a broader age spectrum, whereas previous studies were limited to people aged 25 to 65 years. Consequently, the intake patterns for several dietary factors were somewhat different from those in earlier studies. For example, in previous studies [1415], the intakes of fruits, vegetables, and whole grains were in continuous decline from 2005 to 2013, whereas the current study showed an upward trend starting in 2008, indicating recent improvements in the consumption levels of these food groups in the population. Despite these differences, the ranking of dietary factors remains the same across the studies. The overall moderate improvements in the intakes of fruits, vegetables, and whole grains observed in the present study may possibly be explained by increased knowledge and awareness of nutrition in the population through nationwide nutritional education (e.g., Green Food Education Program), policies (e.g., nutrition fact labeling), and campaigns (e.g., Dietary Life Practice Campaign) focusing on fruit and vegetable intakes over the past few decades [914]. However, as the current levels of dietary intake still remain far below the optimal levels, it is important to develop and promote more effective nutritional strategies to achieve further reduction in disease burdens. Moreover, the contributions of relatively lower-ranked dietary factors, including calcium, milk, meat (unprocessed and processed), and sugar-sweetened beverages, to the disease burden were on a continuous upward trend, indicating emerging nutrition problems that need to be highlighted in future prevention efforts.
In the current study, the PAFs for each diet–disease pair varied extensively according to age group, with generally higher PAFs in the younger age groups. Specifically, younger populations had much higher and more rapidly increasing PAFs from intakes of processed meat and sugar-sweetened beverages, which could be largely explained by the much higher intakes of these food groups in younger populations than in older populations. Further, improvements in dietary patterns (increased intakes of fruits and vegetables) were mainly observed in the older age groups (≥ 44 years), and more unfavorable changes (a sharp increase in processed meat intake) were observed in the younger age group (25–44 years). Our findings suggest possible birth cohort effects, as well as a period effect, that may have influenced dietary intakes over time. Younger populations are more likely to have been exposed to processed meat and sugar-sweetened beverages at a younger age, the critical period for formation of taste and food preferences, and thereby could have more easily adopted a Western diet throughout their lives [11]. Along with changing family structure (an increase in one-member or small-sized families), eating out has become more frequent in Korea [24], especially among younger populations, resulting in greater exposure to diets high in processed meat and sugar-sweetened beverages. Countries like Korea that have undergone dramatic economic development and social change are likely to experience large generational differences (e.g., the birth cohort effect) in lifestyle and disease patterns. Our results indicate that the nutritional transition and dietary patterns vary by age and thus highlight the need for different nutritional strategies for different age groups.
In sensitivity analyses, we observed that the CRA results were slightly different according to dietary assessment methods, whereas other information (e.g., RRs, TMRED, and mortality) stayed the same. This discrepancy in results can be explained by different numbers of food items included in the two methods (FFQ vs. one-day 24-hour recall). The KNHANES FFQ is designed to capture an individual’s habitual intake during the past 12 months using 112 food items and a nine-level frequency scale, whereas the 24-hour recall is designed as an open-ended survey assessing the actual amount of food intake during the past 24 hours. Hence, the estimated intakes of each dietary factor assessed by 24-hour recall were consistently higher than those assessed by the FFQ. The discrepancy between the two methods was particularly high for red meat, indicating the possibility of underestimation of red meat consumption when using the FFQ. In other words, the FFQ may be missing important food items that could largely contribute to the disease burden.
Several limitations of this study should be considered in interpretation of the findings. First, we used a single-day 24-hour recall to assess intake levels of individual dietary factors. This method may not to be able to capture day-to-day variations and long-term average diets, and thus the results may not represent the usual intake of individuals. Second, measurement errors in our dietary data are also possible due to inaccurate reporting of portion size, since the method relies on memory. However, the 24-hour recall may provide adequate estimates of absolute intake levels and group means in a large population. Third, our analysis assumed that the RR for each dietary factor reflects the causal relationships with cardiometabolic and cancer mortality in our study population. Because these RRs were derived from meta-analyses that primarily included people of European descent, it is not certain that the same RRs would describe the relationships in Koreans. As Asians are believed to have different body composition and cardiometabolic profiles than their Western counterparts, further investigations are needed to confirm the diet–disease relationships in Asians and whether the TMREDs used in this study are appropriate optimal levels for this population. Despite the limitations, this study has important strengths. Using nationally representative data, we comprehensively investigated nutritional transitions and associated disease burdens in Korea over the past 19 years. We separately examined the trends in different sex and age groups to identify effective target groups for nutritional interventions and policies. Further, as there are very few data from Asian countries on this subject, this study provides important evidence to inform dietary intervention and policy priorities in Asia.
In conclusion, 231,148 cardiometabolic and cancer deaths were attributable to dietary risk factors in Korea from 1998 to 2016. Among the nine dietary factors evaluated, suboptimal intakes of fruits and whole grains were the leading causes of chronic disease burden. Our data suggest that to reduce the chronic disease burden in Korea, more effective nutritional policies and interventions are needed to target these dietary risk factors.
 XML Download
XML Download