

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Impairment of vascular function, such as increased arterial stiffness and endothelial dysfunction, has been demonstrated as an essential determinant for future cardiovascular events [12]. Vascular endothelial dysfunction and stiffness of large elastic arteries appear to develop from changes in vascular smooth muscle tone and structural components of the arterial wall driven by a reduction in nitric oxide (NO) bioavailability and an increase in oxidative stress and inflammation [3]. Three tests are commonly used in routine clinical practice as methods for measuring cardiovascular function with excellent reproducibility and repeatability: brachial-ankle pulse wave velocity (baPWV; an index of arterial stiffness), flow‐mediated vasodilation (FMD; an index of endothelial function), and carotid intima-media thickness (cIMT; a marker of early atherosclerosis) [4]. These noninvasive tests can serve not only as markers for the assessment of vascular dysfunction but also as predictors of cardiovascular events [56].
A growing body of evidence indicates that natural products such as foods (including herbs and spices) and dietary supplements have physiological benefits and reduce the risk of cardiovascular disease (CVD) [789]. Acanthopanax senticosus Harms (ASH), otherwise known as Siberian ginseng or Gasiogapi in Korea, is widely distributed in the far eastern region of Russia and Northeast Asian countries such as Korea, Japan, and China [10]. The root, fruit, and stem of ASH has been traditionally and commonly used as an adaptogenic medicine [11]. Its potential beneficial effects have been reported both in vitro and in vivo: fruit on immunity [12], insulin resistance, and hepatic lipid accumulation [13]; stem bark on gastric ulcers [14], oxidation [15], allergic reaction [16], and inflammation and nociception [17]; leaves on bacterial infection [18]; and crude extract on radiation-induced brain injury [1619]. However, evidence of the clinical effects of ASH is very limited, having only been reported in a few papers: the root for an alcohol-induced hangover [20] and the leaves on oxidative stress [21] and bone remodeling [22] in postmenopausal women. Therefore, the present study aimed to evaluate the efficacy of ASH fruit on vascular function using a randomized, double-blinded, placebo-controlled trial.
SUBJECTS AND METHODS
Study product
The aqueous extract of ASH fruit and a matched placebo were provided by Lifetree Biotech Co., Ltd. (Suwon, Korea). The dried fruit of ASH was extracted with water at 105°C for 4 h, filtered, vacuum evaporated, and spray-dried to yield a powder after mixing with dextrin (50% in volume). The ASH fruit extract contained 0.17 mg eleutheroside E per gram, as analyzed by the Korean Health Supplement Institute (Seongnam, Korea). The study product was packed in a gelatin capsule to be given a dose of 0, 500, or 1,000 mg ASH fruit extract per day.
Participants
Participants were recruited at Dongguk University Ilsan Hospital (Goyang, Korea). Adults aged 20–64 years were eligible for the study if they had at least 2 of the following criteria: cigarette smoking ≥ 10 per day; 120 mmHg ≤ systolic blood pressure (BP) ≤ 160 mmHg or 80 mmHg ≤ diastolic BP ≤ 100 mmHg; and 220 mg/dL ≤ total cholesterol < 240 mg/dL, 130 mg/dL ≤ low density lipoprotein (LDL) cholesterol < 165 mg/dL, or 150 mg/dL ≤ triglycerides (TGs) < 220 mg/dL. Exclusion criteria were: vigorous physical activity of ≥ 10 h per week; postmenopausal women or receiving hormone replacement therapy; a history of body weight change ≥ 10% in the previous 8 weeks; body mass index ≥ 35 kg/m2; pregnancy or breastfeeding; and a history of vascular disease, diabetes, or any other chronic diseases likely to interfere with study participation.
Study design
This was a 12-week randomized, double-blind, parallel-arm, placebo-controlled, single-center study. The sample size was estimated at 28 subjects per group to detect a difference in endothelial function by a functional ingredient [23] among groups with a statistical power of 80% and a 2-sided alpha of 0.05, allowing for an attrition rate of 10%. The study was reviewed and approved by the Institutional Review Board (IRB) of Dongguk University Ilsan Hospital (IRB No. 2013-117) according to the guidelines laid down in the Declaration of Helsinki and was registered on the World Health Organization International Clinical Trials Registry Platform (No. KCT0001072). All participants provided written informed consent before enrollment.
After the run-in period of 1 week, the eligible subjects were randomly assigned into either the placebo (n = 31), the low-dose (n = 33), or the high-dose group (n = 34) with a dosage of 2 capsules 2 times a day. The randomization code was set using computer-generated random numbers by a researcher who was not engaged in running the trial. The group allocation was blinded for both investigators and participants. The subjects were instructed to maintain their usual dietary and lifestyle habits but to avoid certain foods containing ASH or caffeine and functional foods for vascular health. The subjects were also asked to record dietary intakes and physical activities for 3 days each week (2 weekdays and 1 weekend day) using a smartphone application to monitor the differences in dietary and lifestyle habits among groups. Compliance was monitored every month by counting the remaining tablets. At the beginning and end of the intervention period, BP and vascular function were assessed; adverse events were recorded for the entire study duration; safety hematology, blood chemistry, and urinalysis assessments were carried out; and blood samples were taken after an overnight fast of 12 h for western blotting and oxidized LDL (oxLDL) measurements.
Assessment of vascular function
Subjects rested for at least 10 min in a seated position, and 3 consecutive BP and pulse rate measurements were performed using an oscillometric BP monitor (WatchBP Office; Microlife AG, Widnau, Switzerland) with 1-min intervals between each. baPWV was measured twice using a volume-plethysmographic apparatus (VP-1000; Colin Co., Ltd, Komaki, Japan) between the right brachial artery pressure and both ankles and expressed as the average of the right-side and left-side baPWV values. FMD and cIMT were measured in the brachial artery and the carotid artery, respectively, using a 7.0–14.0Hz multifrequency linear array probe, attached to high-resolution ultrasound sonography (VIVID 7 or 9; GE Healthcare, Milwaukee, WI, USA). cIMT was defined as the distance between the echogenic line and the outer echogenic line, representing the intima-blood interface and the adventitia junction, respectively. cIMT values were calculated as the average of the mean left and right measurements. The brachial artery FMD was measured in the supine position, and baseline artery diameters and peak systolic blood flow velocities were recorded for 1 min before the forearm cuff was inflated to 250 mmHg for 5 min by inducing reactive hyperemia. Following cuff deflation, the diastolic diameter of the brachial artery was recorded for 3 min. The maximum FMD diameter was calculated by averaging 3 consecutive measurements, expressed as the percentage change in the vessel diameter between the baseline and maximal dilation during the 3 min that followed cuff deflation. All measurements were conducted by an experienced operator who was blinded to the study design and groups.
Plasma oxLDL concentration
Plasma oxLDL concentration was measured using an enzyme-linked immunosorbent assay according to the manufacturer's instructions (Mercodia AB, Uppsala, Sweden). Absorbance was measured at 450 nm using a microplate reader (Epoch Microplate Spectrophotometer; BioTek Instruments, Winooski, VT, USA). All trials were done following the manufacturer's instruction.
Western blot analysis
The western blotting analysis was performed to determine endothelial NO synthase (eNOS) and eNOS phosphorylation at Ser1177 in erythrocytes. After lysing the erythrocytes in lysis buffer (iNtRON Biotechnology, Seongnam, Korea), the supernatant was analyzed for protein concentration by the Bradford method (Bio-Rad, Hercules, CA, USA). A total of 120 μg of protein was separated via 8% sodium dodecyl sulfate-polyacrylamide gel electrophoresis and transferred to a polyvinylidene fluoride membrane (Bio-Rad). After blocking with 5% bovine serum albumin, the membranes were incubated with primary antibodies against eNOS, phosphorylated-eNOS (Ser1177; Cell Signaling Technology, Danvers, MA, USA), or β-actin (Santa Cruz Biotechnology, Santa Cruz, CA, USA) followed by incubation with horseradish peroxidase-conjugated secondary antibodies (Santa Cruz Biotechnology). The chemiluminescent signal was visualized and quantified using a ChemiDoc XRS imager equipped with Quantity One software (Bio-Rad).
Statistical analysis
The analysis was based on a per-protocol population to enable efficacy comparisons for randomized subjects who received a placebo or 1 of the 2 interventions without major protocol violations. Extreme outliers were identified for all parameters and removed if they were greater than 3 times the interquartile range for each group within each time point. The data were normally distributed, as assessed from a QQ plot. Differences in the baseline characteristics were examined by 1-way analysis of variance for continuous variables or χ2 tests for categorical variables. The efficacy of ASH fruit over the 12-week intervention period between and within the groups was estimated by applying a linear mixed-effects model considering the random effect (subject), random error (within-subject), and fixed effects (group, week, and group-by-week interaction). All P-values were 2-sided, and those < 0.05 were considered as statistically significant. All statistical analyses were carried out using SAS 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Participant characteristics
The Consolidated Standards of Reporting Trials flow diagram of the study is shown in Fig. 1. Of the 98 eligible subjects initially selected for the study, 76 subjects completed the 12-week intervention without experiencing any serious or severe adverse events. Twenty-two subjects were excluded due to the withdrawal of consent (n = 3) or loss at follow-up (n = 19). The average age of the subjects was 45.1 years old, and they were more likely to be smoked 14.8 cigarettes/day and had elevated systolic and diastolic BP (140.6 and 90.2 mmHg, respectively), elevated TGs (1.9 mmol/L), elevated total cholesterol (5.3 mmol/L), and elevated LDL cholesterol (3.6 mmol/L). There was no significant difference in baseline characteristics between the 3 groups (Table 1), indicating that the subjects in the 3 groups were equally matched. The mean compliance for all subjects was 86.5%. The subjects maintained their habitual diets and lifestyle throughout the study period.
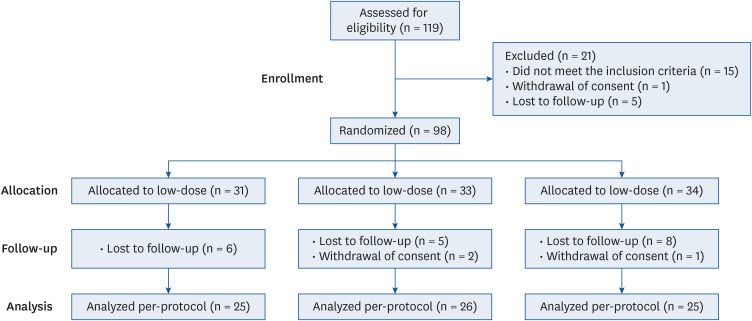
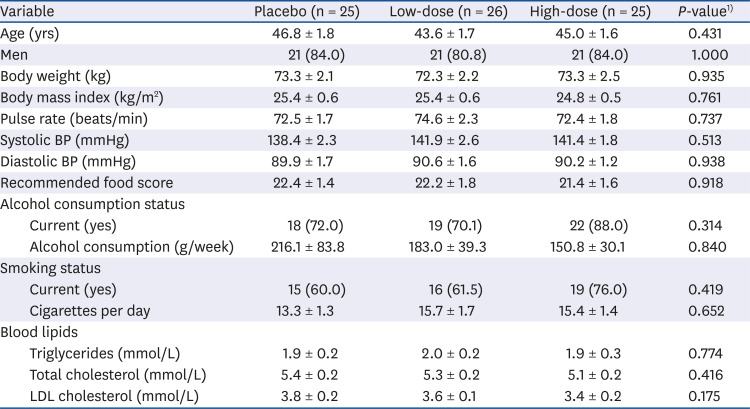
Fig. 1
Consolidated Standards of Reporting Trials diagram showing the flow of participants through the intervention.
![]()
Table 1
Baseline characteristics of the subjects
Data are presented as mean ± SEM or number (%).
BP, blood pressure; LDL, low density lipoprotein.
1)Analysis of variance for continuous variables and χ2 tests for categorical variables were used to compare differences between the groups.
![]()
Vascular function
At the baseline, subjects had similar systolic and diastolic BP, baPWV, FMD, and cIMT (Table 2). There was a significant intervention effect on arterial wall stiffness assessed by baPWV (P for interaction = 0.012). The low-dose group showed more significant changes in baPWV after the 12-week intervention period relative to the placebo group (31.1 vs. −98.7 cm/s; P = 0.007). However, there were no significant changes in FMD and cIMT. Consistent results were found with the low-dose group for the changes in systolic BP after the 12-week intervention period (0.1 vs. −7.7 mmHg; P = 0.044), although the difference in diastolic BP was not significant among the groups.
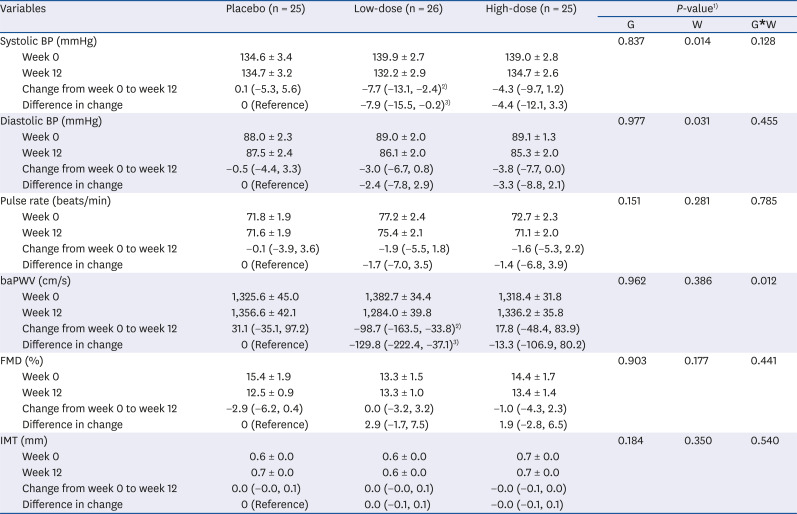
Table 2
Effect of Acanthopanax senticosus Harms fruits on vascular function after 12-week intervention period
Data are presented as mean ± SEM and least square means (95% confidence intervals).
G, group; W, week; BP, blood pressure; FMD, flow-mediated dilation; IMT, intima-media thickness; baPWV, brachial-ankle pulse wave velocity.
1)A linear mixed-effect model was applied to test the intervention effect over the 12-week period between and within the groups taking into account the repeated measurements. P-values for each fixed-effects term (group, week, and group-by-week interaction) in the linear mixed model.
2)P < 0.01 vs. Week 0.
3)P < 0.05 vs. the placebo group.
![]()
Biomarkers for vascular endothelial function
There was a borderline intervention effect on vascular endothelial function assessed by the ratio of phospho-eNOS/eNOS (P for interaction = 0.097; Fig. 2A). Consistent with the aforementioned findings, the low-dose group showed a significantly higher level of eNOS phosphorylation than the placebo group after the 12-week intervention period (0.8 vs. 1.22; P = 0.037) when the ratio of phosphorylated-eNOS/eNOS was normalized to 1 for the placebo group at the baseline. However, plasma oxLDL levels were unchanged in the intervention groups (Fig. 2B).
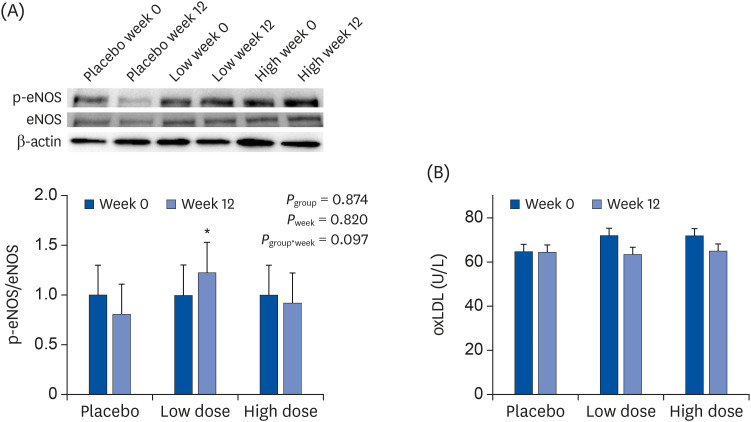
Fig. 2
Effect of ASH fruit supplementation over 12 weeks on biomarkers for vascular endothelial function: (A) eNOS phosphorylation in the erythrocytes and (B) oxLDL level in the plasma of apparently healthy subjects. The protein expression of eNOS and phosphorylation of eNOS were measured by western blotting and their levels normalized to β-actin as the loading control. Values are expressed as least-squares means ± 95% confidence intervals. Significant differences for the groups (placebo, low-dose, and high-dose), week (week 0 and week 12) and group-by-week interaction were evaluated using a linear mixed-effects model.
ASH, Acanthopanax senticosus Harms; p-eNOS, phosphorylated endothelial nitric oxide synthase; eNOS, endothelial nitric oxide synthase; oxLDL, oxidized low density lipoprotein.
*P < 0.05 vs. the placebo group.
![]()
DISCUSSION
In this study, we hypothesized that ASH fruit exerts beneficial effects on improving arterial stiffness and endothelial dysfunction by restoring endothelium-dependent vasodilation in the human body. It is known that cardiovascular risk factors and even borderline levels of these are associated with CVD [2425], and these risk factors can affect the mechanical properties of the blood vessel walls [2]. It is evident that natural products embody a fundamentally different kind of healthfulness by maintaining the normal physiological response [26], and the use of these products, as well as lifestyle modification, for reducing the risks of developing ailments are becoming preferred [25]. Therefore, we recruited healthy subjects with borderline-risk vascular dysfunction and without the need for antihypertensive and lipid-lowering medications to estimate the effect of ASH fruit supplementation better.
In support of the hypothesis, we demonstrated a decrease in baPWV and SBP, and an increase in eNOS phosphorylation in the subjects consumed the low dose of ASH fruit for 12 weeks relative to placebo consumption. The significant reduction in systolic BP is in agreement with the findings from other studies in that systolic BP was statistically lower in the groups supplemented with plant-based functional foods [27282930]. Given the importance of systolic BP [31], ASH fruit supplementation may be able to disable a potentially positive feedback mechanism concerning the relevance of arterial stiffness to cardiovascular risk.
Arterial stiffness measured by pulse wave velocity (PWV) is the most accurate indicator of structural and functional changes in vessel walls [32] and an independent predictor of all-cause and cardiovascular mortality in hypertensive patients [33]. However, measuring carotid-femoral PWV is not an ideal method for routine use because it requires a skilled technique and exposure to the inguinal area during measurement [34]. Therefore, in this study, we decided to use the baPWV, which is a simple method using a separate oscillometric cuff on the 4 extremities. Besides, it has been proven and validated that baPWV can serve as a qualitative index of arterial stiffness and shows similar characteristics to those of carotid-femoral PWV [3435]. An increasing number of studies have reported that baPWV is useful to predict early atherosclerotic changes in the vascular system [36] as well as to identify the potential bioactive in plant-based functional foods for vascular endothelial health [2728293037]. Measurement of FDM of the brachial artery has also been used as an index of endothelial function [1]. In this study, we did not observe statistical significance in FMD values among groups. It might be attributed to the fact that FMD measurements are technically challenging, resulting in a low reproducibility [38].
While the underlying molecular mechanisms remain unclear, there are reviews and human studies that demonstrate a plausible relationship between oxidative stress, cardiovascular risk factors, arterial stiffness, and endothelial dysfunction that importantly focus on hypertension and CVD [394041]. In the present study, 2 possible mechanisms, eNOS activation, and reduced oxidative stress were investigated. A significant increase was found in eNOS activation but not in plasma oxLDL level by low-dose ASH fruit consumption relative to placebo. We could thus conclude that ASH fruit supplementation may reduce BP and arterial stiffness, which may be due, in part, to increased NO signaling via a marked increase in eNOS phosphorylation. Erythrocyte eNOS-derived NO via eNOS phosphorylation plays a prominent role in the regulation of endothelium-dependent vasodilation, blood flow, and the further pathogenesis of vascular disease by contributing to the intravascular NO pool [42]. This result is consistent with Fukada et al. [43], who showed a significant increase in eNOS phosphorylation in lymphatic endothelial cells of fifty 20–39-year-old healthy Japanese females who consumed ASH fruit water extract for 1 month. This result is also in agreement with Johnson et al. [30] who reported that blueberry consumption over 8 weeks in a randomized controlled trial improved endothelium-dependent vasodilation through NO production rather than decreased free radical production. Based on previous studies and the results described herein, an improvement in arterial stiffness and systolic BP in response to ASH fruit can be ascribed to eleutheroside E, the main component of ASH fruit, based on its role in promoting vascular relaxation by activating the eNOS/NO/cyclic guanosine monophosphate signaling pathway [44].
We designed this study to explore whether the effects occur in a dose-dependent fashion. However, the results turned out not to be dose-dependent, leading us to speculate why this happens. One possible reason for this result could be explained by the presence of multiple components in the ASH fruit. It has been suggested that an array of active bioactive co-existing in plant extracts might play additive or antagonistic roles, providing unexpected outcomes when compared with a single isolated component [45]. For example, Ginkgo biloba containing numerous bioactive ingredients substances is known for its health benefits with various pharmacological activities. However, many studies have reported that Ginkgo biloba induced biphasic (hormetic) dose responses in a variety of biological systems and endpoints, including hearing loss, ethanol metabolism, and function of neuronal and glial cells [46]. This position can be further supported by other studies demonstrating the hormetic mechanisms of several plant-derived functional foods [47].
Some limitations of the present study should be acknowledged. First, the reason for the subtle and small depth of response to ASH fruit supplementation could have been due to inter-individual variability the duration and extent of having risk factors. It has been reported that as the disease duration and extent is increased, the risk of atherosclerosis development can increase [48]. However, in the present study, the subjects were included if they had at least 2 risk factors for vascular dysfunction regardless of the category or the degree of severity. Despite the fact that the beneficial effect of ASH fruit was not significantly affected by certain combinations of risk factors (Supplementary Table 1), this heterogeneity could have affected the outcomes of the present study. Second, the generalizability of the findings should be investigated further with caution via the single-center design of our study (implying potential bias in the selection of subjects) and the dosage and parts of the ASH fruit across similar interventions. Third, this study should be replicated in a large cohort or other clinical studies for external validation on an independent sample set to further support that the statistically significant findings were actually due to the intervention and not confounding variables. Besides, sex and gender differences for developing CVD in humans have been reported [49]. Even so, the small unequal sample size between men and women did not allow us to investigate putative sex and gender differences in the response. Furthermore, our study was limited to selected clinical markers, and so further studies would be valuable to elucidate the mechanisms of action by multi-omics profiling related to the up- and downstream signaling pathway of eNOS activation.
Our present study demonstrated that 12-week ASH fruit supplementation reduced baPWV and systolic BP (indicating an improvement in arterial stiffness) at 500 mg/day in healthy adults with smoking and the tendency of having elevated BP or blood lipid parameters. Our results also suggest that this novel beneficial role of ASH fruit could result from the activation of eNOS phosphorylation. Nevertheless, the NO-mediated process may not be one of the ultimate targets of reducing the risk of vascular dysfunction, and so further studies are warranted to elaborate mechanistic and molecular insights into the clinical importance of ASH fruit on the vasodilation effect by utilizing the integration of ASH fruit and its secondary metabolomics with systems biology. Furthermore, the finding from this study opens a new avenue to investigate further the role of ASH fruit in an extended number of subjects to assess for which of the risk factors this supplementation is most beneficial.
 XML Download
XML Download