

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With aging populations, diabetes mellitus has become a chronic metabolic disease affecting adults worldwide [12]. It is the most common noninfectious disease with a rapidly increasing incidence and is one of the leading causes of increased mortality [3]. As reported by the International Diabetes Mellitus Federation (IDF), diabetes mellitus was reported in approximately 425 million adults worldwide in 2017 and the number is expected to continue to increase to 600 million adults by 2045 [4], with type 2 diabetes mellitus (T2DM) accounting for nearly 90% of cases [3]. In Taiwan, there are about 2 million diabetic patients; the number continues to increase by 20,000 per year, with nearly 10,000 people dying from diabetes mellitus annually [5], indicating the potentially heavy social burden of diabetes mellitus care.
T2DM is partly a hereditary disease and is also strongly dependent on environmental factors, lifestyle, and dietary habits [6]. With disease progression, patients gradually develop disordered metabolism; that is, β cells fail to produce enough insulin due to insulin resistance, resulting in complications such as dyslipidemia, hypertension, inflammatory mediator increase, coronary heart disease (CAD), serum adiponectin reduction, hypercoagulable state, and vascular endothelial dysfunction [78]. Bhowmik et al. [9] reported that dyslipidemia is common in T2DM and pre-diabetes mellitus and its prevalence is especially high in patients with high triglyceride (TG) and low high-density lipoprotein-cholesterol (HDL-C) levels; excessively high TG levels may be a result of diseases such as diabetes mellitus, hypothyroidism, kidney disease, or liver disease.
There are numerous studies in terms of glycated hemoglobin A1c (HbAlc). HbA1c can be effectively managed by improving health literacy and promoting self-management and good lifestyles among patients [101112]. Health literacy is conceptualized as health-improving skills, namely, the necessary knowledge, motivation, and capability for acquiring, understanding, assessing, and using health information [13]. Health literacy is especially pertinent for the self-management of diabetic patients [14] as good self-management contributes to disease control and delayed occurrence of chronic complications. Good self-management includes not only problem solving, active planning, and goal setting but also refers to the establishment of personal problem-solving skills and effective treatment of chronic disease symptoms [151617]. However, only 23% of T2DM patients have treatment compliance and maintain HbA1c levels below 7% [18]. Therefore, good daily living habits are a key lifestyle factor for HbA1c management in T2DM patients [14].
Lifestyle factors that lead to T2DM include smoking, heavy alcohol consumption and poor diet, exercise habit, and mental health, which can result in or exacerbate the complications of T2DM [19]. Recent epidemiological studies on alcohol consumption and the risk of T2DM have shown that moderate drinkers have the lowest risk of diabetes mellitus [192021] but that smoking is a risk factor for drug resistance in diabetes mellitus treatment [22]. Biswas et al. [23] also demonstrated the importance of long-term sedentary lifestyle as a risk factor for T2DM and that regular exercise helps manage blood sugar, lower cardiovascular risk factors, and improve overall health, thereby providing preliminary protection. In addition, exercise lasting more than 8 weeks can reduce HbA1c management performance by 0.66% [22]. Combined, these findings underscore the need for T2DM self-management in daily life, including healthy diets, regular exercise, blood glucose self-monitoring, and medication. In addition to affecting HbA1c management, these lifestyle choices also affect blood lipid levels [24]. In short, more attention should be paid to the impact of lifestyle on the health literacy of patients with T2DM.
A growing number of studies have identified the potential predictors influencing effective self-management; however, they mainly focus on the impact of single lifestyle habits on T2DM management [10192526]. This study, therefore, focused on providing empirical outcomes of the effects of lipid profile tests and multiple good lifestyle habits on the management of HbA1c level in diabetic patients, aiming to improve the knowledge, motivation, and ability of diabetic patients in using health information to improve their health literacy.
Go to : 
SUBJECTS AND METHODS
Design
This study enrolled a total of 349 T2DM patients with more than 5 care visits, between November 30, 2016, and June 30, 2017, within the diabetic care network under the Health Management Plan led by the Taiwan Department of Health (DOH). Based on relevant literature, an Outpatient Record Form of Diabetes Mellitus Care was designed and lipid profile tests were performed for data collection and analysis. The study program was reviewed and approved by Institutional Review Board of the Kaohsiung Veterans General Hospital (VGBKS16-CT12-22).
Instruments
Referring to relevant reports [2728], this study designed an Outpatient Record Form of Diabetes Mellitus Care for data collection. The patients underwent HbA1c testing after enrollment. According to results retrieved from their medical records, the patients were divided into 2 groups based on HbA1c level (≤7.5% or > 7.5%.) Statistical analysis was performed on the 2 groups.
According to the recommended diabetes-care indicators in the Diabetes Mellitus Prevention Handbook [2930] published by the Taiwanese Association of Diabetes Educators and the Health Promotion Administration, Ministry of the Health and Welfare, the Outpatient Record Form of Diabetes Mellitus Care was designed as outlined below and tabulated in Table 1 [283031].
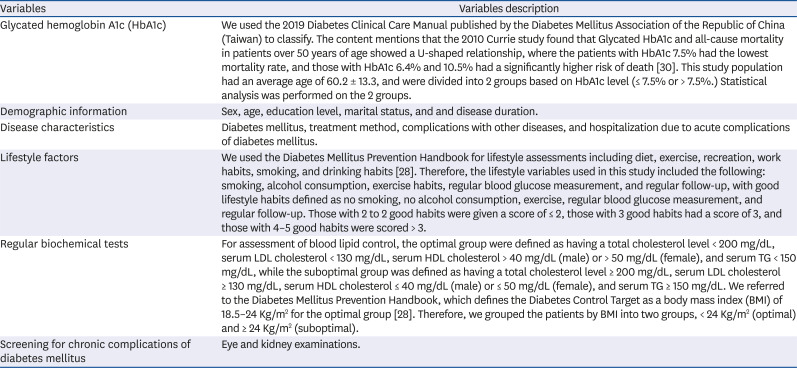
Table 1
Outpatient record form of diabetes mellitus care
| Variables | Variables description |
|---|---|
| Glycated hemoglobin A1c (HbA1c) | We used the 2019 Diabetes Clinical Care Manual published by the Diabetes Mellitus Association of the Republic of China (Taiwan) to classify. The content mentions that the 2010 Currie study found that Glycated HbA1c and all-cause mortality in patients over 50 years of age showed a U-shaped relationship, where the patients with HbA1c 7.5% had the lowest mortality rate, and those with HbA1c 6.4% and 10.5% had a significantly higher risk of death [30]. This study population had an average age of 60.2 ± 13.3, and were divided into 2 groups based on HbA1c level (≤ 7.5% or > 7.5%.) Statistical analysis was performed on the 2 groups. |
| Demographic information | Sex, age, education level, marital status, and and disease duration. |
| Disease characteristics | Diabetes mellitus, treatment method, complications with other diseases, and hospitalization due to acute complications of diabetes mellitus. |
| Lifestyle factors | We used the Diabetes Mellitus Prevention Handbook for lifestyle assessments including diet, exercise, recreation, work habits, smoking, and drinking habits [28]. Therefore, the lifestyle variables used in this study included the following: smoking, alcohol consumption, exercise habits, regular blood glucose measurement, and regular follow-up, with good lifestyle habits defined as no smoking, no alcohol consumption, exercise, regular blood glucose measurement, and regular follow-up. Those with 2 to 2 good habits were given a score of ≤ 2, those with 3 good habits had a score of 3, and those with 4–5 good habits were scored > 3. |
| Regular biochemical tests | For assessment of blood lipid control, the optimal group were defined as having a total cholesterol level < 200 mg/dL, serum LDL cholesterol < 130 mg/dL, serum HDL cholesterol > 40 mg/dL (male) or > 50 mg/dL (female), and serum TG < 150 mg/dL, while the suboptimal group was defined as having a total cholesterol level ≥ 200 mg/dL, serum LDL cholesterol ≥ 130 mg/dL, serum HDL cholesterol ≤ 40 mg/dL (male) or ≤ 50 mg/dL (female), and serum TG ≥ 150 mg/dL. We referred to the Diabetes Mellitus Prevention Handbook, which defines the Diabetes Control Target as a body mass index (BMI) of 18.5–24 Kg/m2 for the optimal group [28]. Therefore, we grouped the patients by BMI into two groups, < 24 Kg/m2 (optimal) and ≥ 24 Kg/m2 (suboptimal). |
| Screening for chronic complications of diabetes mellitus | Eye and kidney examinations. |
Note. We used BECKMAN DxH1601 Fully Automatic Blood Cell Analyzer to instruments blood HbA1c and lipids [31].
![]()
Statistical analysis
The variables analyzed in the present study included age (≤ 65 or > 65 years), sex (male or female), education level (< primary school, high school or less, or junior college), disease duration (< 3 years, 3-10 years inclusive, or > 10 years), BMI (< 24 or ≥ 24 kg/m2), other chronic illness (Yes or No), family history (Yes or No), smoking (Yes or No), alcohol consumption (Yes or No), exercise (Yes or No), regular blood glucose measurement (Yes or No), and regular follow-up (Yes or No). One-way Pearson Chi-square tests were performed to explore the correlation between categories. Finally, multivariate regression analysis was performed to explore the effects of all factors on HbA1c. Modeling was conducted to explore lifestyle factors associated with suboptimal HbA1c levels (i.e., HbA1c > 7.5%). After data collection, statistical descriptions and analyses were conducted using IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, New York) in which the appropriate statistical methods were selected according to the research variables. Statistical results are presented in Tables with supplementary explanations. P-values < 0.05 were considered to indicate statistical significance.
Go to :
RESULTS
Baseline characteristics of diabetic patients
As shown in Table 2, this study enrolled a total of 349 patients. The average age was 60.2 years, with approximately 36% participants more than 65 years of age. In particular, the highest proportion of patients with HbA1c > 7.5% (62.2%) were ≤ 65 years of age; among them, 55.5% were male. A high proportion of patients with HbA1c > 7.5% (63.3%) had BMI ≥24 kg/m2 and a high proportion of participants in this group had a family history of chronic diseases. The disease duration averaged 8.55 years, with 28.7% and 35.8% of the total patients having durations less than 3 and more than 10 years, respectively, a statistically significant difference by Pearson Chi-square test (P = 0.002). Among patients with disease duration of fewer than 3 years, 3-10 years (inclusive), and more than 10 years, 25.1%, 35.3%, and 39.6% had HbA1c levels > 7.5%, respectively, with the largest proportion having more than 10 years of disease duration. Of the 349 T2DM patients, approximately 59% (P = 0.002) were also diagnosed with other chronic illness. Among those with other chronic illnesses, 63.3% had HbA1c > 7.5%, a higher proportion than that in the group without other chronic illnesses (36.7%). Regarding the education level, 18.4% of the patients were illiterate, while 39.7% had a high school education or above (P = 0.032). Among patients with no education (illiterate), junior high school education or less, and senior high school education or above, 20.9%, 41.5%, and 37.6% had HbA1c levels > 7.5%, respectively, with the highest proportion occurring in the group with a junior high school education or less. Among lifestyles, patients with ≤ 2 and 3 good habits accounted for 37.5% and 41.3% of the study population, respectively (P = 0.008). Among patients with ≤ 2, 3, and > 3 good habits, 38.2%, 43.8%, and 18.0% had HbA1c levels > 7.5%, respectively, with the group with 3 good habits having the highest proportion. As shown in Table 1, disease duration, other chronic illness, education level, and lifestyles had significant effects on the distribution of patients with HbA1c > 7.5%.
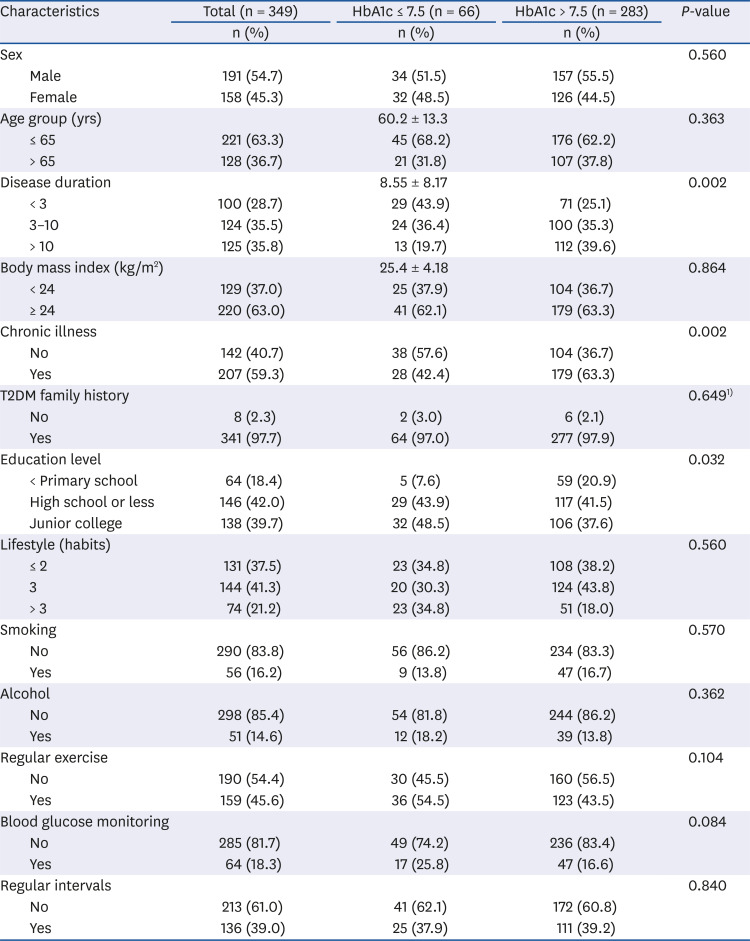
Table 2
Effect of demographic characteristics on HbA1c level
![]()
Lifestyle on lipid profile in diabetic patients
Table 3 presents a cross-tabulation between 5 good lifestyle habits, HbA1c management performance, and lipid profile to assess the correlation with lipid profile to lifestyle habits and HbA1c > 7.5%. For different HbA1c management levels, there was a statistically significant difference (P = 0.044) in the distribution of cholesterol levels, indicating a significant correlation between optimal cholesterol and HbA1c levels. Among patients with optimal and suboptimal cholesterol levels, 77.3% and 85.8% had HbA1c levels > 7.5%, respectively, indicating that a high proportion of patients with suboptimal cholesterol levels also had suboptimal HbA1c levels. Moreover, there was a statistically significant difference (P = 0.013) in the distribution of LDL-C among different HbA1c groups, indicating a significant correlation between LDC-C and HbA1c levels. Among patients with optimal and suboptimal LDC-C levels, 77.4% and 88.5% had HbA1c levels > 7.5%, respectively, indicating that a high proportion of patients with suboptimal LDL-C levels also had HbA1c > 7.5%. A statistically significant difference (P = 0.018) was also observed in the distribution of LDL-C among different alcohol consumption groups, indicating a correlation between LDL-C and alcohol consumption. Among patients with optimal and suboptimal LDL-C levels, 82.5% and 92.0% did not consume alcohol, respectively, indicating that a high proportion of patients with suboptimal LDC-C levels did not consume alcohol. Finally, we also observed a statistically significant difference (P = 0.013) in the distribution of HDL-C among different exercise groups. Among patients with optimal and suboptimal HDL-C levels, 53.3% and 39.9% exercised, respectively, indicating that a high proportion of patients with optimal HDL-C levels also exercised.
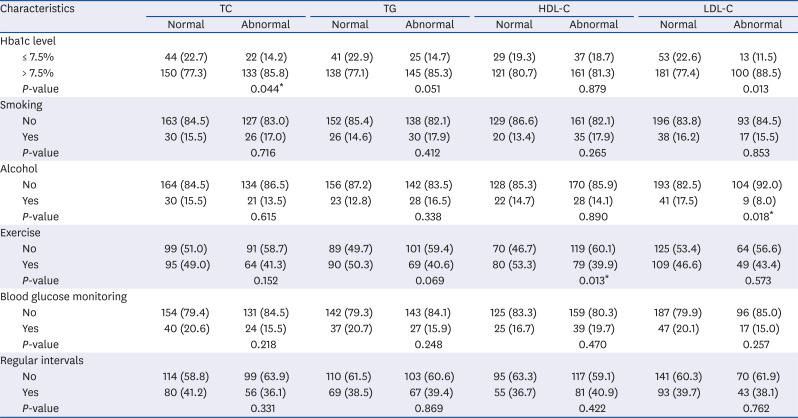
Table 3
Effect of lifestyle on lipid profile in diabetic subjects (n = 349)
Values are presented as number of patients (%).
TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; HbAlc, glycated hemoglobin A1c.
*P < 0.05.
![]()
HbA1c management predictors of basic demographic characteristics, chronic illness, and lifestyle factors
As shown in Table 4, after correction for the compounding effects of basic demographic characteristics (sex, age, disease duration, BMI, family history, and educational level), the regression analysis results of Model 1 showed that the odds of HbA1c > 7.5% in patients with a disease duration over 10 years was 3.849 (P = 0.001) times that in patients with a disease duration of fewer than 3 years. In other words, patients with a long disease duration (> 10 years) had less optimal HbA1c management than those with a short disease duration (< 3 years). For education levels, the odds of HbA1c > 7.5% in illiterate patients was 4.427 (P = 0.006) times that in patients with senior high school education or above, indicating that illiterate patients had less optimal HbA1c management than those with senior high school education or above. In addition to the basic demographic characteristics, Model 2 also considered other chronic illnesses. After correction for the compounding effects of the basic demographic characteristics, Model 2 showed that disease duration and education level had significant effects on HbA1c management. The odds of HbA1c > 7.5% in patients with a disease duration of more than 10 years was 3.189 (P = 0.005) times that in patients with a disease duration of fewer than 3 years. The odds of HbA1c > 7.5% in illiterate patients was 4.063 (P = 0.005) times that in patients with senior high school education or above; however, other chronic illness had no significant effect on HbA1c management.
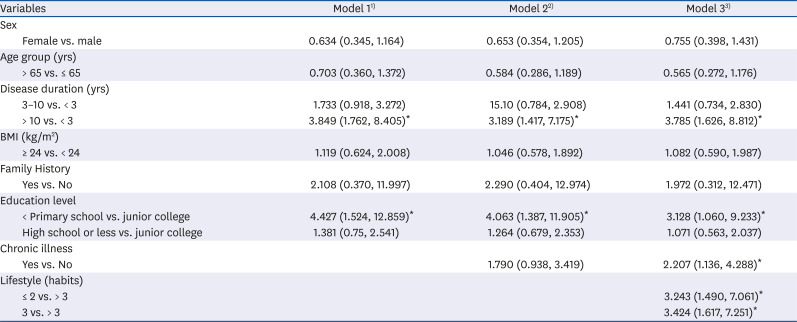
Table 4
Multivariate logistic regression analysis of optimal HbA1c level (n = 349)
HbAlc, glycated hemoglobin A1c.
*P < 0.05.
1)Adjusted for demographic characteristics.
2)Adjusted for demographic characteristics and chronic illness.
3)Adjusted for demographic characteristics, chronic illness, and lifestyle habits.
![]()
Model 3 included lifestyle factors (≤ 2, 3, and > 3 good lifestyle habits). After correction for the compounding effects of basic demographic characteristics (sex, age, disease duration, BMI, family history, and education level) and other chronic illnesses, Model 3 showed that the odds of HbA1c > 7.5% in patients with a disease duration of more than 10 years was 3.785 (P = 0.002) times that in patients with a disease duration of fewer than 3 years. In addition, the odds of HbA1c > 7.5% in illiterate patients was 3.128 (P = 0.039) times that in patients with senior high school education or above. The odds of HbA1c > 7.5% in patients with other chronic illness was 2.207 (P = 0.019) times that in patients without other chronic illness. Among the 5 good lifestyle habits, the odds of HbA1c > 7.5% in patients with ≤ 2 and 3 good habits were 3.243 (P = 0.003) and 3.424 (P = 0.001) times that in patients with > 3 good habits, a statistically significant positive correlation, indicating that patients with ≤ 2 and 3 good habits had less optimal HbA1c management than that in patients with > 3 good habits.
Go to :
DISCUSSION
This study included basic demographic characteristics (sex, age, disease duration, BMI, family history, and educational level) in 3 models. Model 2 considered additional chronic illnesses and Model 3 included lifestyle factors (smoking, alcohol consumption, exercise, regular blood sugar measurement, and regular follow-up). These 3 models were used to explore the associations between suboptimal HbA1c levels and the above factors, revealing that lifestyle factors were significantly correlated with HbA1c management in each model. In particular, patients with a long disease duration, illiteracy, and other chronic illness had less optimal HbA1c management, while those with more than 3 good lifestyle habits had optimal HbA1c management.
The results of the present study revealed a significant correlation between HbA1c management and disease duration and education level, regardless of whether only basic demographic characteristics were included and their compounding effects were collected (Model 1), or with additional consideration of other chronic illnesses (Model 2). HbA1c management in patients with disease duration of more than 10 years was less optimal than that in patients with a disease duration of fewer than 3 years. A similar finding was observed in a Japan-based study by Hayashino et al. [32], who reported less optimal glycemic management with increasing disease duration, with a linear relationship between disease duration and HbA1c levels; Daher et al. [16] also observed that patients with more than 10 years of disease duration had difficulty in managing blood sugar due to gradual decline of β-cell function and gradual increase in insulin resistance. Smith et al. [16] also reported that assistance from nearby hospitals and clinics was conducive to the selfmanagement of chronically ill patients. As shown above, disease duration was related to HbA1c management. Therefore, diabetic patients should receive regular follow-up in nearby clinics and hospitals. Moreover, hospitals or health units should provide educational outreach in communities and parks to promote the public understanding of the disease, help the public improve on unhealty lifestyle behaviors, and promote health literacy and skills for effective self-management and prevention of T2DM.
Regarding education levels, the results of this study revealed that less optimal HbA1c management in illiterate patients than that in patients with education. This observation was consistent with that of Maneze et al. [14], who reported that patients with a low education level had insufficient knowledge about diabetes mellitus, resulting in suboptimal HbA1c management. Similarly, Liu et al. [33] recommended that educational intervention in the form of lively and interactive animations be used to improve the effectiveness of health education. Due to population aging and high illiteracy among older people, standardized health education may be difficult for them to understand [1434]. Therefore, combining storytelling and performance with public health specialties in a relaxed manner may allow patients and their family members to jointly learn about diabetes mellitus self-management and increase their knowledge to alleviate the long-term negative effects of low education level on HbA1c management.
The results of the present study showed less optimal HbA1c management in diabetic patients with other chronic illness than that in patients without chronic illnesses. Kautzky-Willer et al. [35] reported that chronic illness such as hypertension, kidney diseases, and mental disorders are key factors affecting HbA1c management, as these diseases may gradually increase the risk of developing T2DM due to their negative effects on HbA1c levels. A Mexico-based study by Herrington et al. [36] observed that the causes of death most closely related to diabetes mellitus were vascular diseases, renal diseases, or infection, recommending that patients receive medication treatment regardless of socioeconomic status as well as in regular screening for complications for timely treatment to improve the quality of patient care. The effects of different chronic diseases on T2DM have been extensively investigated, with the occurrence of chronic diseases related to factors such as genetics, diet, exercise, and lifestyle. Given this context, the World Health Organization (WHO) suggested that the provision of primary preventive health services can lead to optimal HbA1c management and reduce complications [37]. Studies have also reported the associations between chronic diseases and major lifestyle factors [3839]. Therefore, the establishment of patient-specific health literacy in daily life is required to promote chronic disease prevention and management.
The results of the present study revealed optimal HbA1c management in patients with more than 3 good lifestyle habits. Similar to the results reported by Jia et al. [22] and the American Diabetes mellitus Association, our study indicated that lifestyle habits were the underlying factors affecting the treatment of patients with T2DM. Diabetic patients should increase dietary fiber intake, avoid smoking, have moderate alcohol consumption, and exercise regularly to reduce the risk of T2DM [40]. In addition, a longitudinal study by Houle et al. [25] indicated that diabetic patients require not only good diets and regular exercise but also regular medication and self-testing of blood sugar levels, as these practices are related to HbA1c management. Akter et al. [4142] found that people who smoked 10 cigarettes per day had a 16% higher risk of T2DM than that in those who did not; however, the risk steadily decreased with increased smoking cessation duration, with the risk of T2DM in those who had stopped smoking for 10 years falling to the same level as that in those who did not smoke. Previous studies have reported that moderate alcohol consumption is associated with a reduced incidence of T2DM and improved cardiovascular health in diabetic patients; however, the risk of T2DM is increased in heavy and binge drinkers, leading to decreased metabolism in patients with cardiovascular diseases [1920214344]. In addition, exercise also plays an important role in the management of T2DM, as regular exercise increases insulin sensitivity, which is beneficial for managing blood sugar, reducing cardiovascular risk factors, and improving overall health [22]. In addition, self-testing of blood sugar levels can reveal patterns in blood glucose levels throughout the day to remind patients of the need for self-management and has been proven particularly important for the treatment of patients with T2DM [45]. As shown above, T2DM patients should change their lifestyle habits to healthy ones in the long-term.
The results of the present study demonstrate that the risk of T2DM may be significantly alleviated by lipid profile tests or lifestyle correction. Patients should be provided with effective empirical outcomes and develop healthy behaviors, as these measures can reduce the risk of complications and premature death. Only by helping T2DM patients with their lifestyle habits is it possible for them to effectively manage their HbA1c levels and enhance their health literacy.
This study reported empirical outcomes showing that maintaining good lifestyle habits can effectively improve T2DM management and promote patient knowledge, motivation, and ability to use health information. Furthermore, patients with more years of disease duration, with education, or with good lifestyle habits had optimal HbA1c management. Thus, T2DM patients should conduct effective self-management, take precautions in their daily lives and improve their health literacy for quality diabetes mellitus care.
Go to :
 XML Download
XML Download