

 PDF
PDF Citation
Citation Print
Print



A 58-year-old male with a past medical history of diabetes mellitus type II, hyperlipidemia, diskitis, and Streptococcus gordonii endocarditis presented to the emergency department with fever and chills. Due to known history of endocarditis, an urgent transthoracic echocardiogram (TTE) was performed which revealed a 2.2 × 1.3 cm tricuspid valve vegetation, 1.7 × 0.3 cm pulmonary valve vegetation, and a quadricuspid aortic valve with mild regurgitation (Figure 1A, B, and D). Transesophageal echocardiogram (TEE) was performed and confirmed a quadricuspid aortic valve and revealed a large aortic root abscess with fistula formation from the right coronary cusp into the right ventricle (Figure 1C, E-G, Figure 2A and B). Surgical intervention confirmed abscess vegetation extending from the right coronary cusp into the interventricular and interatrial septums, creating a large necrotic fistula to the right atria and ventricle (Figure 2C). Extensive cardiac surgery was performed and included composite aortic root replacement, reimplantation of left main coronary artery, right coronary artery bypass grafting, tricuspid valve replacement, and aortic sinus to right ventricle fistula repair with bovine pericardial patch.
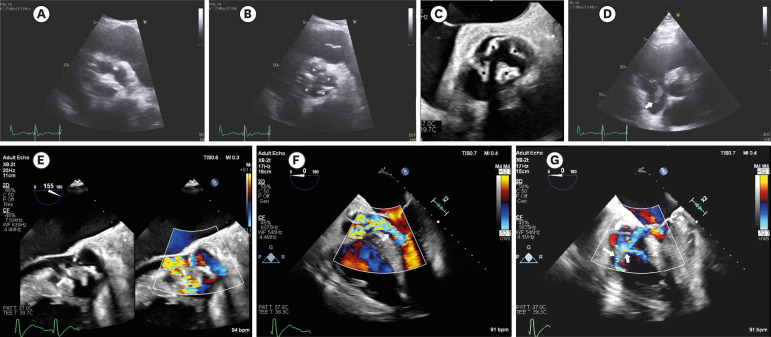 | Figure 1TTE in parasternal short axis illustrating aortic valve during diastole (A) and systole (B, asterix). TEE demonstrating aortic quadricusp valve (C, asterix). TTE in parasternal short axis demonstrating a mobile echo-density on the tricuspid valve suggestive of a vegetation (D, arrow). TEE image showing severe aortic regurgitation and valvular defect consistent with right ventricular fistula formation (E and F, arrows). TEE demonstrating right ventricular fistula with multiple jets from aortic root (G, arrows).TEE = transesophageal echocardiogram; TTE = transthoracic echocardiogram.
|
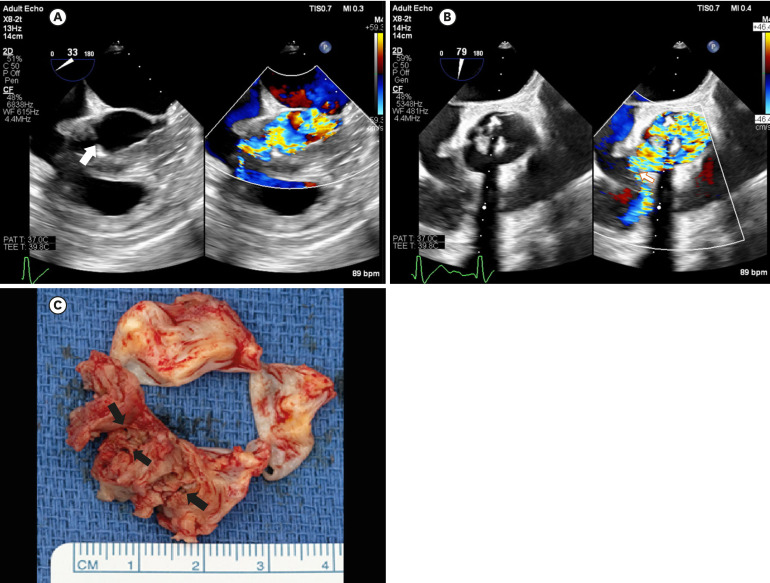 | Figure 2TEE short axis view of aortic valve demonstrating large abscess with fistula formation (A, arrow). TEE short axis view illustrating fistula formation into right ventricle (B, arrow). The gross anatomy specimen of the aortic root with evidence of multiple fistulas (C, arrows).TEE = transesophageal echocardiogram.
|
The incidence of sinus of Valsalva aneurysm and fistula formation is variable, but has documented to be as high as 0.96%.1) In a study by Takach et al.2) over 40 years, 129 cases were noted. Cases of aneurysm/fistula were most commonly associated with a history of endocarditis, bicuspid aortic valve, ventricular septal defects, and Marfan's syndrome. The treatment of choice is surgical correction.3)
 XML Download
XML Download