

 PDF
PDF Citation
Citation Print
Print



A previously healthy 34-year-old man presented with progressive dyspnea and chest pain after viral infection. Initial transthoracic echocardiography (TTE) depicted massive pericardial effusion and he underwent pericardiocentesis of 900 mL serosanguinous fluid without identifiable malignant cells. Pericarditis-associated pericardial effusion was initially impressed. Nevertheless, follow-up TTE 3 months later demonstrated recurrent pericardial effusion without identifiable pericardial mass. Cardiac magnetic resonance (CMR) imaging revealed a huge mass, located at pericardial space with right atrial compression (Figure 1A), which was also revealed by transoesophageal echocardiography (Figure 1B). A firm tumor in size of 5.5×4.5 cm, which severely adhered to the pericardium and extended to right atrial wall, superior vena cava and aorta, was excised (Figure 1C). The pathologic examination confirmed the diagnosis of primary pericardial angiosarcoma, given the presence of malignant endothelial cells mainly in pericardial soft tissue (Figure 1D and E). Therapy with pembrolizumab and pazopanib was administered. Unfortunately, CMR revealed the recurrence of tumor 4 months after the surgery, and salvage radiotherapy was performed.
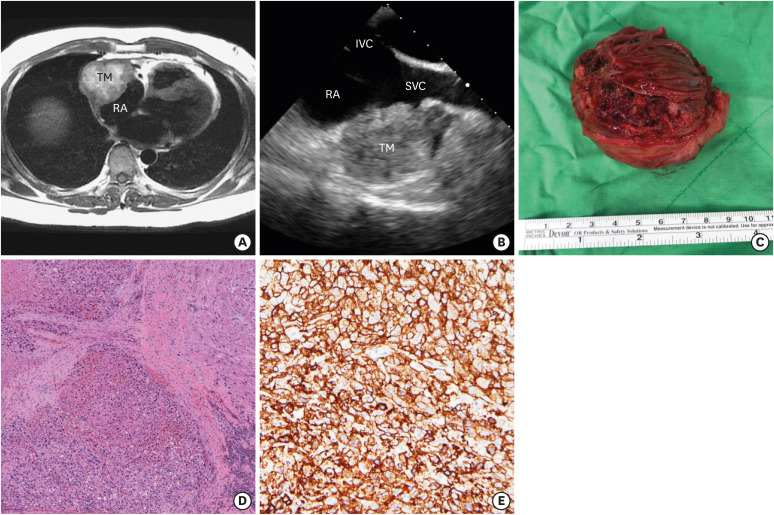 | Figure 1Primary pericardial angiosarcoma. (A) CMR image revealed a huge hyperintense T1-weighted mass at pericardial space with right atrial compression. (B) TEE demonstrated the tumor, located adjacent to RA and SVC. (C) The excised tumor, in size of 5.5×4.5 cm, showed prominent necrosis and hemorrhage. (D) Pericardial soft tissue with infiltration of malignant endothelial cells (H&E, ×40). (E) The tumor cells were positive for CD34 immunohistochemical staining (×200).CMR = cardiac magnetic resonance; H&E = hematoxylin and eosin stain; IVC = inferior vena cava; RA = right atrium; SVC = superior vena cava; TEE = transoesophageal echocardiography; TM = tumor mass.
|
Primary pericardial angiosarcoma is extremely rare, and clinical prognosis of this disease is unfavorable.1) It is particularly difficult to diagnose pericardial malignancy at the early stage by TTE alone.2) Sequential imaging studies, such as computed tomography or CMR, are warranted to prevent erroneous diagnosis, particularly for those with undetermined and recurrent pericardial effusion.3) Furthermore, a positron emission tomography scan, which was not performed in our case, plays a role on evaluating the extent of primary tumor, as well as the possibility of distant metastasis.4)
 XML Download
XML Download