

 PDF
PDF Citation
Citation Print
Print



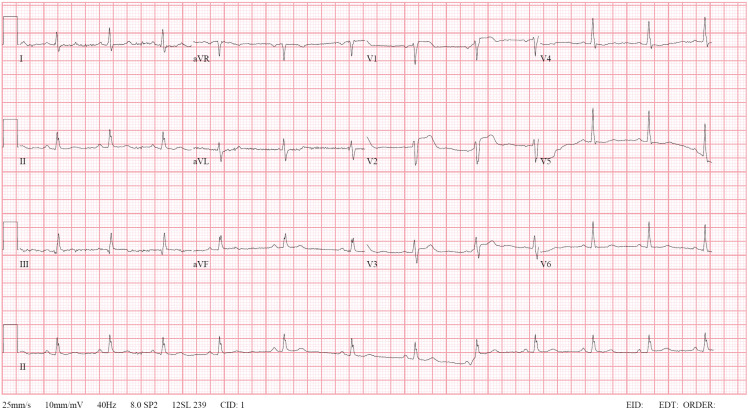
A 48-year-old male visited to the emergency room with chest pain. Electrocardiography showed ST elevations in the precordial leads (Figure 1), and ST-segment elevation myocardial infarction in the left anterior descending (LAD) artery territory was diagnosed. Coronary angiography (CAG) showed significant lesions of the mid-LAD artery and septal branch, and percutaneous coronary intervention (PCI) for the mid-LAD artery lesion was performed (Supplementary Videos 1 and 2). The right coronary artery (RCA) could not be identified despite using pigtail catheter (Supplementary Video 3). The procedure was finished after planning computed tomography coronary angiography (CTCA) to confirm the RCA anatomy.
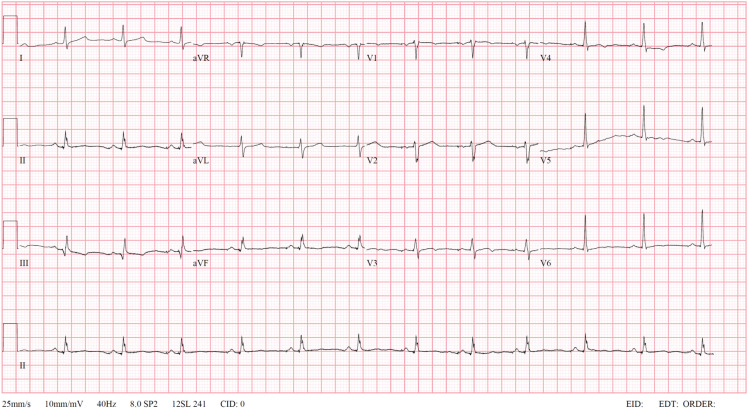
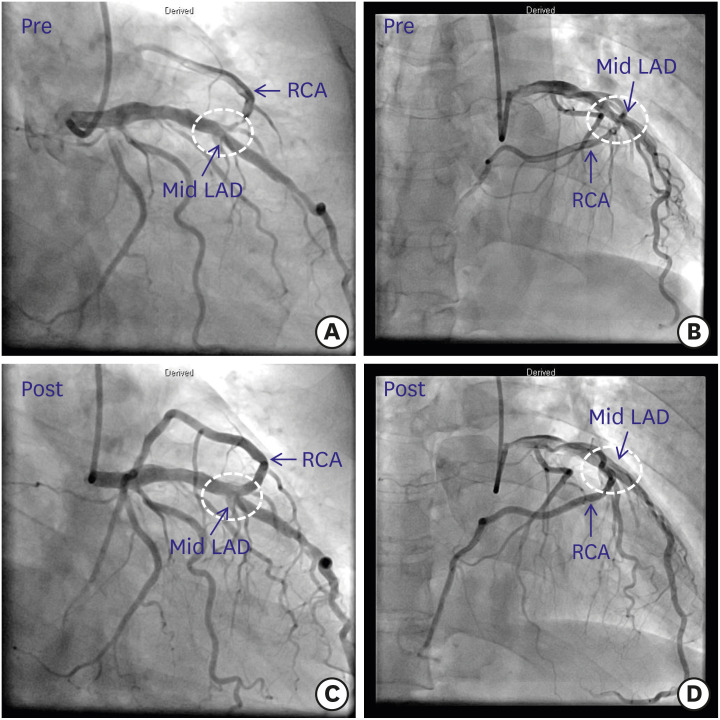
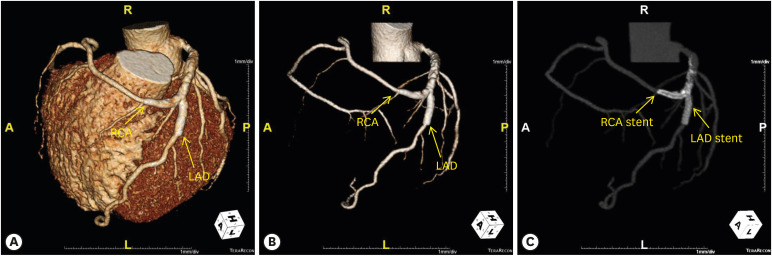
After the procedure, he no longer complained of chest pain, and electrocardiography showed improvement in ST elevations in the precordial leads (Figure 2). Transthoracic echocardiography showed a diastolic D-shape of left ventricle, suggesting right ventricular infarction (Supplementary Video 4). Transradial CAG on the next day revealed an anomalous origin of the RCA arising from the mid-LAD artery with significant stenosis of the RCA ostium. This bifurcation site was treated using T stenting technique (Figure 3). CTCA also confirmed an anomalous course of the RCA and showed the patency of the stents (Figure 4).
A single coronary artery is an extremely rare congenital anomaly of the coronary system in structurally normal heart.1)2)3) To our knowledge, only one patient has been reported to undergo PCI for a true LAD artery/RCA bifurcation lesion treated using two-stent technique.4) We emphasize the importance of clinical effort to evaluate all coronary arteries in patients with coronary artery anomalies.

 XML Download
XML Download