

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The diagnostic and therapeutic strategies in patients with coronary artery disease have focused on identifying and alleviating both extent and severity of myocardial ischemia as it is the most important prognosticator.1) Thus, fractional flow reserve (FFR) has been a standard method for identifying ischemia-related epicardial coronary stenosis, accruing an abundance of clinical evidence on the benefit of FFR-guided treatment decisions.2)3) However, high FFR values (>0.80) do not necessarily imply freedom from future events. Indeed, clinical events still occur in patients who are deferred based on high FFR.2)
The microvasculature is one of main coronary circulatory system, and the presence of microvascular disease can be the cause of clinical events in patients without epicardial coronary stenosis.4) In a cardiac catheterization laboratory, its presence can be assessed using a single pressure/temperature-sensor coronary wire or a Doppler wire. Previous studies have demonstrated the added prognostic implications of coronary flow reserve (CFR) and index of microcirculatory resistance (IMR) in patients with high FFR,4)5) and the recent European guidelines supported the importance of invasive physiologic assessment using CFR and IMR in patients with stable coronary artery disease.6) However, long-term follow-up results according to pattern of FFR, CFR, and IMR in large numbers of patients are not yet available. This multinational and multicenter study sought to investigate the long-term prognostic implications of CFR and IMR in patients with coronary artery disease.
METHODS
Patient population
The present study was a patient-level pooled analysis of three prospective registries whose results have been previously published.4)5)7)8)9) The first study prospectively enrolled consecutive patients from five university hospitals in Korea (519 patients, 737 vessels), each undergoing clinically indicated invasive coronary angiography, and FFR, CFR, and IMR measurement for at least one coronary artery.5) The second study was an institutional registry of Tsuchiura Kyodo General Hospital, Ibaraki, Japan that included 643 patients (643 vessels) submitting to invasive angiography and physiologic assessment, including FFR, CFR, and IMR.7) The third study prospectively enrolled patients with FFR, CFR, and IMR data on at least one intermediate-grade stenosis from Hospital Clinico San Carlos, Madrid, Spain.8) In all such studies, patients with hemodynamic instability, left ventricular dysfunction, or a culprit vessel of acute coronary syndrome were excluded. Individual patient data for pooled analysis were collected using standardized spreadsheets. For all variables included, standardized definitions were used. Invasive physiologic indices were also cross-checked and confirmed by each study's principal investigators.
Among the 1,397 patients (1,694 vessels) enrolled overall, those undergoing percutaneous coronary intervention (PCI) were excluded, leaving 867 patients (1,152 vessels) who did not undergo PCI for the current analysis. Only one of the deferred patients was lost to follow-up. Study protocols were designed in accord with the Declaration of Helsinki and were authorized by Institutional Review Boards or Ethics Committees at corresponding centers. All patient participants granted written informed consent. The study protocols were in accordance with the Declaration of Helsinki. The study protocol of International Collaboration of Comprehensive Physiologic Assessment was registered at ClinicalTrials.gov (NCT03690713).
Angiographic analysis and coronary physiologic measurements
Coronary angiography was performed by standard techniques. All angiograms were analyzed at local core laboratories in blinded fashion. Percent diameter stenosis, minimum luminal diameter, reference-vessel size, and lesion length were measured. All coronary physiologic parameters were measured following diagnostic angiography. A guide catheter (5-7 Fr) without side holes was used to engage coronary arteries, and a pressure/temperature-sensor guide wire (St. Jude Medical [Abbott Vascular], St. Paul, MN, USA) was used to measure FFR and CFR.
To derive resting mean transit time (Tmn), a thermodilution curve was obtained by delivering three injections (3–4 mL each) of room-temperature saline. Hyperemia was induced by intravenous infusion of adenosine (140 µg/kg/min) via peripheral or central vein. Proximal aortic pressure (Pa), distal arterial pressure (Pd), and hyperemic Tmn were then measured during sustained hyperemia. Once measurements were complete, the guidewire was pulled back to the guide catheter, and potential pressure drift was checked. CFR was calculated as resting Tmn/hyperemic Tmn. For lesions with low FFR (≤0.80), PCI was recommended, as stipulated by current guidelines. However, decisions regarding PCI were at the discretion of operators. Patients who underwent PCI were excluded from the final analysis. The uncorrected IMR was calculated as Pd × Tmn during hyperemia. All IMR values were corrected by Yong's formula (Pa × Tmn × ([1.35 × Pd/Pa] − 0.32).
Cutpoints for physiologic indices and classification of patients
Cutpoints were set at FFR ≤0.80 (low FFR), CFR ≤2 (low CFR), and IMR ≥23 U (high IMR), as previously described.4)5)10)11)12) Patients with high FFR (>0.80) were grouped by CFR and IMR values as follows: 1) Group A (high CFR and low IMR); 2) Group B (high CFR and high IMR); 3) Group C (low CFR and low IMR); and 4) Group D (low CFR and high IMR).
Patient follow-up, outcome measurements, and adjudication of clinical events
Clinical data were obtained at outpatient clinic visits or by telephone contact if needed. The primary study endpoint was patient-oriented composite outcome (POCO), including all-cause mortality, any MI, and any revascularization. Secondary endpoints were individual components of POCO. As a sensitivity analysis, vessel-oriented composite outcome (VOCO), which included vessel-related cardiac death, vessel-specific myocardial infarction (MI), and vessel-specific revascularization was assessed. All clinical outcomes were defined as stipulated by the Academic Research Consortium, including the addendum to the definition of MI.13) In the absence of a clear non-cardiac cause, all deaths were considered cardiac related.
Statistical analysis
Categorical variables were expressed as numbers and relative frequencies (percentages), and continuous variables as means and standard deviations or medians with interquartile ranges (Q1–Q3) according to related distributions, which were checked by the Kolmogorov-Smirnov test. Linear regression analysis was used to estimate correlation coefficients of quantitative variables. Kappa values were calculated to gauge classification agreement, using established cutpoints of each invasive physiologic index. Event rates were calculated from Kaplan-Meier censoring estimates and presented with cumulative incidences, using log-rank or Breslow test to compare survival curves between groups. Cox proportional hazard regression was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for between-group comparisons. The assumption of proportionality was assessed graphically by log-minus-log plot, and Cox proportional hazard models for all clinical outcomes satisfied the proportional hazards assumption.
Data were analyzed on a per-patient basis for clinical characteristics and outcomes, and on a per-vessel basis for comparison of lesion characteristics and physiologic indices. The vessel of lowest FFR served as representative for per-patient analysis in instances of multivessel measurements. In per-vessel analyses, a generalized estimating equation (GEE) was applied to adjust for intrasubject variability among vessels of the same patient. Estimated means and 95% CIs were presented as summary statistics. A GEE procedure with pairwise comparison was invoked to address per-vessel variables in the four-group classification. No post-hoc adjustment was done. For the per-vessel comparison of the risk of VOCO, a marginal Cox proportional hazard regression model was used.
To identify independent predictors of POCO, a multivariable Cox model was used. Covariates of clinical relevance or showing univariate relations with outcomes (p<0.1) were entered into marginal multivariable Cox models. Candidate variables were carefully chosen, given the number of events available, to ensure parsimony of final models. We calculated Harrell's c-statistics (with 95% CI) to validate each model's discriminant function, assessing gains (with or without integrated physiologic indices) as relative integrated discrimination improvement (IDI). Each analysis incorporated a participating center as a random effect. All probability values were 2-sided, with p values <0.05 considered statistically significant. Standard software applications (SPSS v18.0 [SPSS Inc, Chicago, IL, USA] and SAS v9.3 [SAS Institute, Inc., Cary, NC, USA]) were used for statistical analyses.
RESULTS
Baseline characteristics of patients and vessels
Table 1 shows clinical, angiographic, and physiologic characteristics of the 867 patients (1,152 vessels) selected for study. Most presented with stable ischemic heart disease (IHD), and in those with acute coronary syndrome, non-culprit vessels were physiologically interrogated. Anatomic severity of epicardial coronary stenosis was largely of intermediate grade (mean diameter stenosis, 40.9±15.6%; mean FFR, 0.88±0.07), and FFR values were ≤0.80 in 164 vessels (14.2%). Mean CFR was 3.03±1.28, with CFR ≤2.0 in 300 vessels (26.0%), and median IMR was 17.4 U (Q1–Q3, 12.8–24.3 U), 324 vessels (28.1%) showing high IMR values. Supplementary Figure 1 depicts the distributions of FFR, CFR, and IMR.
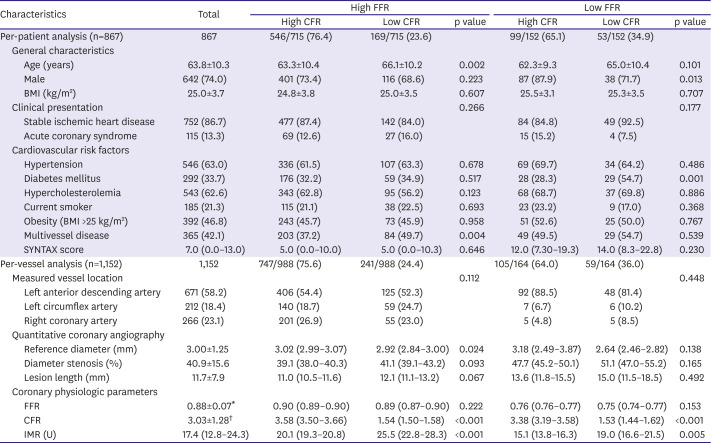
Table 1
General characteristics of deferred population and target vessels
Values expressed as mean±standard deviation, median (interquartile ranges, 25th–75th), estimated mean (95% confidence interval) (per-vessel analysis), or number (%). Generalized estimating equation model or maximum likelihood χ2 test used for overall and between group comparisons in per-vessel analysis.
BMI = body-mass index; CFR = coronary flow reserve; FFR = fractional flow reserve; IMR = index of microcirculatory resistance; MI = myocardial infarction; PCI = percutaneous coronary intervention.
*FFR: median, 0.88 (Q1–Q3: 0.83–0.93); †CFR: median, 2.86 (Q1–Q3: 2.00–4.00).
![]()
FFR and CFR showed modest correlation (r=0.113, p<0.001) and low categorical agreement (κ=0.095, p<0.001), with discordance in 268 patients (30.9%) (Figure 1). IMR was highest in patients of high FFR and low CFR (overall comparison p<0.001) (Table 1).
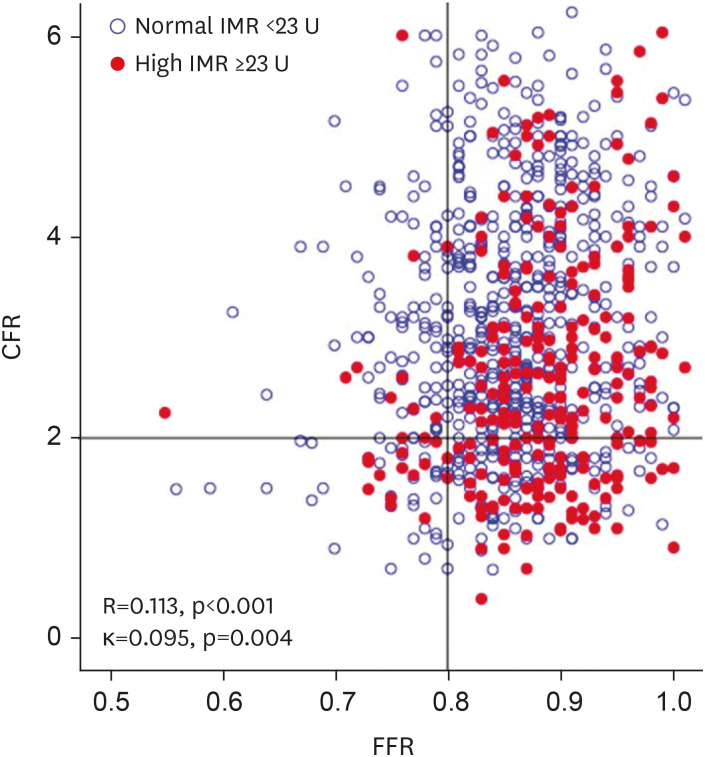
Figure 1
Distribution of deferred patients according to FFR and CFR.
Distribution of patients with deferred revascularization is presented according to FFR and CFR. Red dots indicate high index of microcirculatory resistance (IMR, ≥23 U). All IMR values corrected by Yong's formula (Pa × Tmn × ([1.35 × Pd/Pa] − 0.32).
CFR = coronary flow reserve; FFR = fractional flow reserve; IMR = index of microcirculatory resistance.
![]()
Clinical outcomes of deferred patients by FFR and CFR
Figure 2 presents the 5-year risk of POCO among deferred patients with high or low FFR according to the CFR level. In patients with high FFR, those with low CFR were at significantly greater risk in terms of POCO (14.9% vs. 8.6%, HR, 1.846; 95% CI, 1.083–3.146; p=0.024) and cardiac death or MI (HR, 5.662; 95% CI, 1.984–16.154; p=0.001) than those with high CFR. Similarly, those with low CFR showed significantly greater risk of POCO than those with high CFR in patients with low FFR (34.8% vs. 14.0%, HR, 2.383; 95% CI, 1.066–5.329; p=0.034) (Figure 2 and Supplementary Table 1).
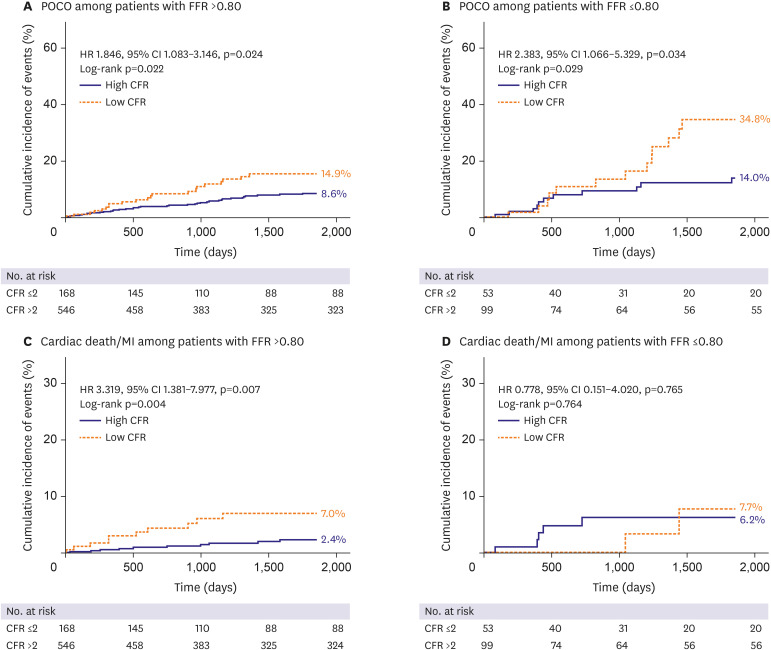
Figure 2
Impact of coronary flow reserve on cumulative incidence of clinical outcomes.
Cumulative incidence POCO in patients with (A) low FFR (≤0.80) and (B) high FFR (>0.80), shown by CFR values.
CFR = coronary flow reserve; CI = confidence intervals; FFR = fractional flow reserve; HR = hazard ratio; MI = myocardial infarction; POCO = patient-oriented composite outcome.
![]()
Clinical outcomes by CFR and IMR in absence of functionally significant epicardial coronary stenosis
When evaluating distributions of CFR and IMR in patients with high FFR, modest correlation (r=0.230, p<0.001) and low categorical agreement (κ=0.159, p<0.001) were evident, but discordance of CFR and IMR was demonstrable in 33.8% (242/715) of patients with high FFR (Figure 3 and Table 2). On the other hand, severity of angiographic stenosis did not differ in the 4-group classifications (by CFR and IMR), and although FFR values differed in the four groups, the absolute difference was within 0.02. Distributions of clinical risk factors were mostly similar, except for age and proportion of multivessel disease. Group D showed the lowest CFR and highest IMR values (both p<0.001) overall (Table 2).
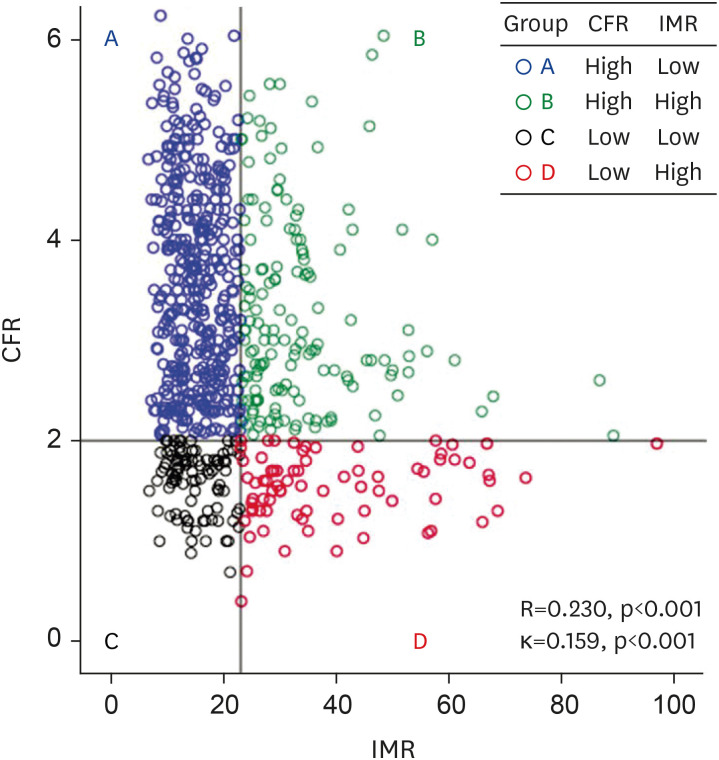
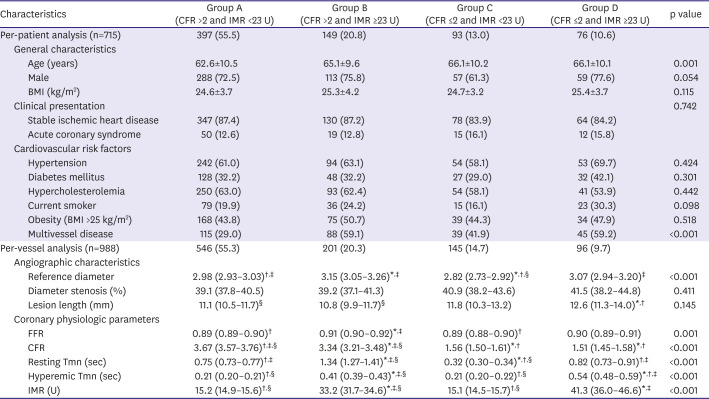
Figure 3
Distribution of deferred patients with high fractional flow reserve (>0.80) by CFR and IMR.
Since there was weak correlation between CFR and IMR and agreement between the 2 indices was low, therefore, 4 different patterns were observed.
CFR = coronary flow reserve; IMR = index of microcirculatory resistance.
![]()
Table 2
Angiographic and physiologic differences in deferred patients with high FFR, shown by microvascular function
Values expressed as mean±standard deviation (per-patients analysis), estimated mean (95% confidence interval) (per-vessel analysis), or number (%). Generalized estimating equation model or maximum likelihood χ2 test used for overall and between-group comparisons in per-vessel analysis.
CFR = coronary flow reserve; FFR = fractional flow reserve; IMR = index of microcirculatory resistance; MI = myocardial infarction; Pa = aortic pressure; Pd = distal pressure; Tmn = mean transit time.
*p<0.05 vs group A; †p<0.05 vs group B; ‡p<0.05 vs group C; §p<0.05 vs group D.
![]()
Among these patients, the total cumulative incidence of POCO and VOCO were 11.9% (83 events) and 7.3% (70 events) at 5 years. Risks of POCO were comparable in groups A, B, and C, as were individual clinical outcomes. Group D (low CFR and high IMR, indicating overt microvascular disease), showed significantly higher risk of POCO than the other groups (overall comparison p=0.013), surpassing that of group A by nearly 3-fold (21.2% vs. 8.0%, HR, 2.873; 95% CI, 1.476–5.594; p=0.002). The risk of cardiac death or MI in Group D was also higher than that of Group A (10.4% vs. 2.3%, HR, 5.662; 95% CI, 1.984–16.154; p=0.001) (Figure 4 and Table 3). Per-vessel analysis also showed significantly greater risk of VOCO only in group D, compared with other groups (overall comparison p=0.018), again surpassing that of group A by nearly 3-fold (HR, 3.029; 95% CI, 1.468–6.248; p=0.003) (Supplementary Figure 2).
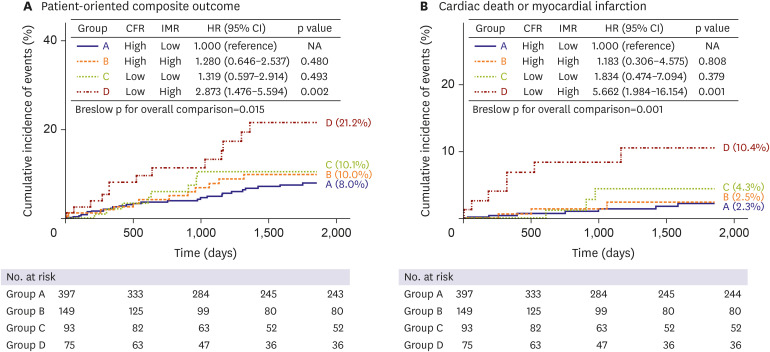
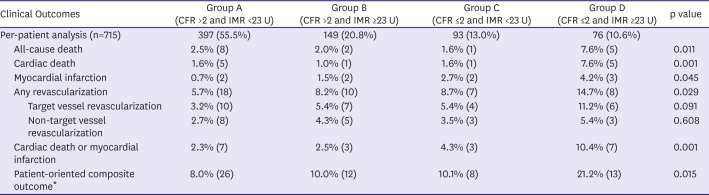
Figure 4
Clinical outcomes by microvascular status, based on CFR and IMR in deferred patients with high fractional flow reserves (>0.80).
Cumulative incidences of (A) patient-oriented composite outcomes and (B) cardiac death or myocardial infarction in 4 patient groups divided by CFR and IMR in patients with deferred revascularization based on high fractional flow reserve (>0.80).
CFR = coronary flow reserve; CI = confidence intervals; HR = hazard ratio; IMR = index of microcirculatory resistance; NA = not applicable; PCI = percutaneous intervention.
![]()
Table 3
Clinical outcomes of deferred patients with high FFR shown by CFR and IMR
Data expressed as cumulative incidences of clinical outcomes and number of events. Cumulative incidences of clinical outcomes represent Kaplan-Meier estimates during median follow-up of 1,854.5 days (Q1–Q3, 763.8–1,855.0 days). The p values for log-rank or Breslow test in survival analysis.
CFR = coronary flow reserve; FFR = fractional flow reserve; IMR = index of microcirculatory resistance.
*Patient-oriented composite outcomes include all-cause mortality, any myocardial infarction, and any revascularization.
![]()
Additive prognostic values of CFR and IMR in absence of functionally significant epicardial coronary stenosis
In patients with high FFR, the presence of diabetes mellitus or multivessel disease showed an independent association with occurrence of POCO. When incorporating CFR and IMR into the multivariable model, the presence of overt microvascular disease also proved independently predictive of POCO; and this model with physiologic classification showed significantly more improvement in relative IDI (0.248, p=0.046) (Table 4).
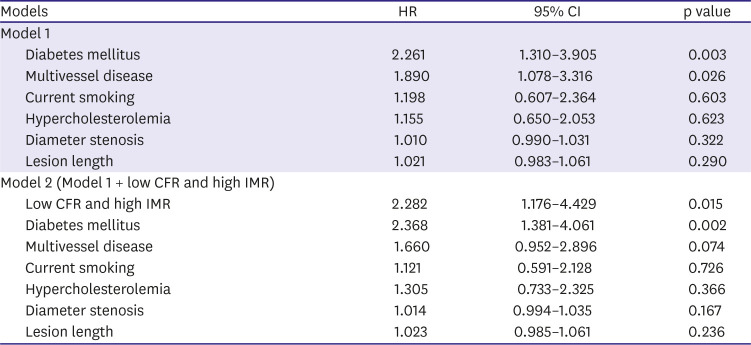
Table 4
Independent predictors of patient-oriented composite outcomes* in deferred patients with high FFR
C-index of models: model 1, 0.674 (95% CI, 0.606–0.742) and model 2, 0.691 (95% CI, 0.618–764); relative integrated discrimination improvement of 0.248 in model 2 (p=0.046).
CFR = coronary flow reserve; CI = confidence interval; HR = hazard ratio; IMR = index of microcirculatory resistance.
*Patient-oriented composite outcomes include all-cause mortality, any myocardial infarction, and any revascularization.
![]()
DISCUSSION
The current study was undertaken to investigate long-term clinical outcomes of deferred patients relative to microvascular status. The main findings are as follows: 1) Patients with low CFR showed significantly greater risk of POCO than those with high CFR, regardless of FFR level. In patients with high FFR, those with low CFR also showed significantly greater risk of cardiac death or MI than those with high CFR; 2) high-FFR patients stratified by CFR and IMR into 4 groups demonstrated no clear differences in clinical and angiographic characteristics; 3) patients with low CFR and high IMR (overt microvascular disease) showed significantly greater risk of POCO, driven by greater risk of all individual components of POCO, including cardiac death or MI; and 4) overt microvascular disease was found independently associated with occurrence of POCO, and integrating physiologically defined overt microvascular disease improved the ability to discriminate risk of POCO.
Currently, FFR-guided treatment decision is a standard approach, the advantages over an angiography-guided strategy having been established through randomized clinical trials and large-scale registries.2)14)15)16)17) However, clinical events still occur in patients with high FFR (>0.80). In the FAME 2 trial, 15.7% of patients in the high-FFR registry arm (FFR >0.80) experienced death, MI, or urgent revascularization during 5-year follow-up. Furthermore, 10.1% of this same arm was suffered by persistent angina at 5 years. Because the coronary circulatory system is multicompartmental, the absence of significant epicardial coronary stenosis does not exclude potential IHD. Nevertheless, diagnosis and treatment of IHD have primarily focused on the epicardial coronary arterial system.
In earlier studies, patients with depressed (vs. preserved) Doppler-derived coronary flow velocity reserve have shown significantly increased risks of major adverse cardiovascular events.18)19)20) Studies of thermodilution-derived CFR have reported similar findings,4)5) although relatively small numbers of low-CFR patients were involved, and the role of CFR as a risk factor for death or MI was not clearly defined. Herein, we evaluated a multinational patient population in the course of comprehensive physiologic assessment, showing a significantly greater risk of POCO for patients with low (vs. high) CFR, regardless of FFR level. In addition to greater risk of any revascularization, the risk of cardiac death or MI was also elevated in the high-FFR/low-CFR population subset. Given the similarities in severity of angiographic stenosis and FFR, CFR stratification in high-FFR patients seems to originate from differences in microvascular status, underscoring the importance of measuring CFR in patients lacking functionally significant epicardial stenosis.
CFR is based on the ratio of hyperemic and resting coronary flow (or flow velocity), so various combinations of resting and hyperemic flow conditions may account for low CFR. By combining CFR with IMR, which reflects hyperemic microvascular resistance, underlying mechanisms of myocardial ischemia or microvascular dysfunction are better delineated. The current study rested on 4-patient grouping of both CFR and IMR in a population of patients with high FFR. Although CFR and IMR showed a significant correlation, the degrees of correlation and categorical agreement demonstrated were quite weak. These clinical and physiologic backdrops are precisely why discordance between CFR and IMR is an important and prognostically relevant issue.
In the current study, preserved CFR and yet high IMR in group B were chiefly due to high resting Tmn (low resting coronary flow), despite increased microvascular resistance; and those patients with high CFR and high IMR showed no increased risk of clinical events. This result is supported by a previous study, which showed the low potential for myocardial ischemia in preserved CFR patients with low resting and hyperemic flow.21) Conversely, depressed CFR in Group C was mainly due to the low resting Tmn (high resting flow). Hyperemic Tmn values did not differ in groups C and A (high CFR and low IMR). Although high resting coronary flow may result from disturbed autoregulatory processes in coronary circulation,19) intra-individual variability in resting conditions,22) or uncontrolled blood pressure or heart rate,21) there was no increased risk of clinical events in this group. This finding can be explained in part with the constraints of CFR, which is dependent on the resting condition of a patient.23)
Only group D, displaying concordantly abnormal CFR and IMR, showed significantly increased risk of POCO, surpassing the other groups. All individual components of POCO, including cardiac death, MI, and any revascularization, were also highest in group D. Even after multivariable adjustment, the presence of overt microvascular disease was independently associated with occurrence of POCO, and integrating overt microvascular disease significantly improved the ability to discriminate POCO risk. Thus, the importance of comprehensive physiologic assessment using both CFR and IMR in high-FFR patients is apparent. Furthermore, the current results support the recent European Society of Cardiology guidelines for chronic coronary syndrome which recommended the measurement of CFR and IMR in patients with recurrent chest pain but lack of functionally significant epicardial coronary stenosis as class IIa recommendation.6)
In terms of underlying mechanisms for subsequent clinical events in the face of functionally insignificant epicardial coronary stenosis, previous studies have implicated a mechanistic link involving microvascular disease, endothelial dysfunction, and inflammatory activity that precedes intimal thickening, macrovascular lipid deposition, thin-cap fibroatheroma (TCFA) proclivity, and coronary vasomotor dysfunction.24)25)26)27)28)29) Of note, Dhawan et al.29) reported that coronary flow velocity reserve <2.0 was an independent predictor of virtual histology-intravascular ultrasound-defined TCFA. Similarly, Usui et al.30) also demonstrated high IMR was associated with both the presence of optical coherence tomography-defined TCFA and plaque rupture in non-culprit lesions of acute coronary syndrome.
Ischemia-directed revascularization is a standard care for patients with IHD. However, it should be noted that high FFR does not necessarily imply absence of IHD or freedom from future cardiovascular events. There are heterogeneous mechanisms and presentations of IHD requiring more comprehensive pursuit of possible causes. Our data indicate significantly increased risks of clinical events in patients with abnormal CFR and IMR results. In such patients with higher risk of future clinical events, meticulous management of comorbidities, intensified secondary prevention, patient education, close follow-up and surveillance for future adverse clinical events are needed.
Some limitations of the present study deserve mention. First, the decision to perform PCI was at the discretion of the operators, thereby allowing potential selection bias (especially in instances of low FFR but preserved CFR). In addition, intravascular imaging (i.e., intravascular ultrasound) was not routinely performed, so pure microvascular disease and diffuse atherosclerotic narrowing could not be discriminated in patients with high FFR and low CFR. Also, participating investigators were not blinded to physiologic indices, perhaps influencing management strategies in these patients, and results of non-invasive tests were not available in our study. In addition, information about medical treatment was not systematically collected. Finally, this study was not a randomized controlled trial, so inherent limitations of such registries may apply.
In patients consigned to deferred revascularization, those with low CFR showed significantly greater risk of POCO than those with high CFR, regardless of FFR. Furthermore, in patients with high FFR, those with overt microvascular disease (low CFR and high IMR) showed significantly greater risk of POCO and cardiac death or MI. Comprehensive physiologic assessment for microvascular function would be helpful to better predict future clinical events in patients with functionally insignificant coronary stenosis.
 XML Download
XML Download