

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiac myxoma is the most frequent benign cardiac tumor which accounts for about 50% to 80% of primary cardiac tumors.1)2) Although it can cause valvular heart disease-like heart failure, constitutional symptoms and embolic complications, the diagnosis is often challenging because of its heterogeneous clinical features. These clinical manifestations depend on characteristics of the tumors including size, location, mobility and the surface.3)4) Echocardiography is the most commonly used imaging modality to identify the presence of cardiac masses and to characterize the tumor. However, diagnosis of the tumor depends on the pathologic findings and cardiac myxoma is known to be identified in about 70% of the operated cases with primary cardiac and pericardial tumors.5) In recent years, the number of asymptomatic patients diagnosed as myxomas can increase as cardiac imaging studies are frequently performed as a health screening. We evaluated clinical and echocardiographic findings in patients with cardiac tumors suggesting cardiac myxoma and compared these characteristics of non-myxoma tumors with myxoma.
Go to : 
METHODS
Subjects
We retrospectively reviewed medical records and echocardiographic data in all patients with echocardiographic diagnosis of cardiac myxoma from January 2005 to June 2019 in 4 teaching hospitals in Korea (Chungnam National University Hospital [CNNUH, Daejeon], Chonnam National University Hospital [CNUH, Gwangju], Eulji Medical Center [EMC, Daejeon] and Jeonbuk National University Hospital (JBNUH, Jeonju). The study protocol was approved by the local ethics committee of the Institutional Review Board (IRB) of each hospital (IRB No. CNNUH, 2019-003-008; CNUH, 2019-086; EMC, 2019-03-014; JBNUH, 2019-10-045). The written informed consent was waived by IRBs because this study was retrospective and anonymous clinical data were used for analysis. We followed the Helsinki Declaration Principles to conduct this study.
Demographic and clinical data
We evaluated the baseline demographic data including age, sex, cardiovascular risk factors, past history of stroke or other systemic embolic events, and family history of cardiac myxomas from their medical records. We also investigated referral reasons for echocardiography and initial presenting symptoms. Final pathological diagnosis and postoperative recurrence were examined in the patients who underwent the surgical resection.
Echocardiographic analysis for tumor characteristics
The investigators (Lee SH, Park JH, Cho JY and Chin JY) of each hospital who were blinded to patients' final pathological diagnosis reanalyzed echocardiographic data of the cardiac tumors. Tumor size was measured by width and height based on the attachment site. Characteristics of the myxomas were classified as follows: irregularity of the surface (smooth vs. polypoid), shape (round, ovoid vs. prolapsing), presence of pedicle (narrow stalk vs. broad base), presence of mitral valve (MV) obstruction, calcification and necrosis. The presence of MV obstruction was assessed by the application of continuous wave Doppler on the apical 4-chamber view in the same manner as the evaluation of mitral stenosis in non-tumor cases. Mobility was arbitrarily divided as non-mobile, half-mobile and highly mobile. Tumors without movement along the cardiac cycle were classified as non-mobile and those with movement along the cardiac cycle but not across the mitral annular plane for left atrial tumors were as half-mobile. Highly mobile tumors were defined as the tumors that prolapse across the mitral annular plane during cardiac cycle. In the cases of tumors in other sites rather than left atrium (LA), the investigators classified tumor mobility into one of 3 categories at the investigator's own discretion.
Statistical analysis
Continuous variables are presented as mean±standard deviation and categorical variables as percentages (%). The χ2 test was used for between-group comparison of categorical variables and a Mann-Whitney U test for comparison of the numeric data. The SPSS Statistics 25 (IBM Inc., Chicago, IL, USA) software was used for statistical analyses. In all cases, p values <0.05 were considered statistically significant.
Go to :
RESULTS
Clinical characteristics of study population
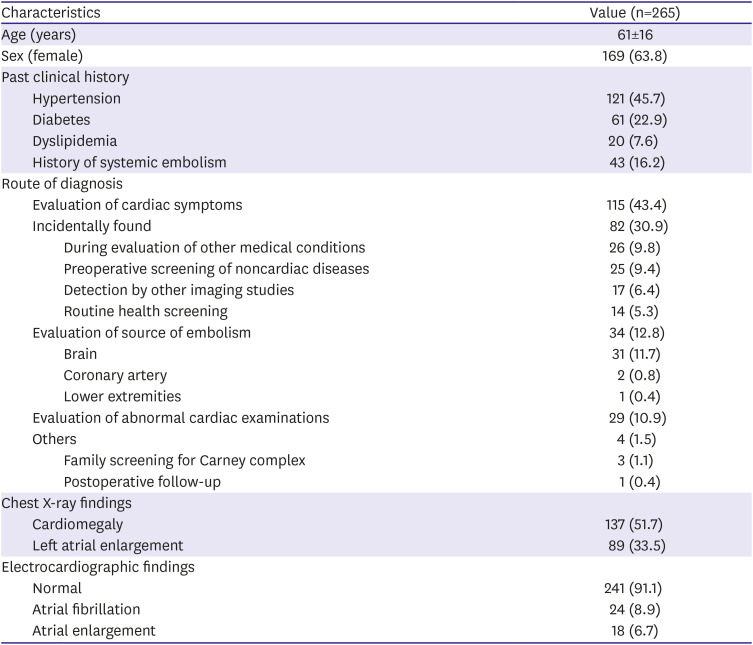
A total of 265 consecutive patients with echocardiographic diagnosis of cardiac myxomas were enrolled (Figure 1). The mean age was 61±16 years (median, 64; range, 4–96 years) and 169 patients (63.8%) were female. Transthoracic echocardiography (TTE) was the initial diagnostic method in 229 patients (86.4%). In the remainders (13.6%), myxomas were incidentally detected by computed tomography which were performed for the evaluation symptoms (cardiac or noncardiac) or for health screening. The assessment of cardiac symptoms was the most common referral reason for echocardiography in 115 patients (43.4%). Other indications included evaluation of cardioembolic source in 34 patients (12.8%), workup for abnormal findings such as murmurs, abnormal electrocardiography or chest radiographs in 29 patients (10.9%), and others including family screening for Carney complex and postoperative follow up in 4 patients (1.5%, Table 1). In 82 patients (30.9%), the tumors were incidentally detected by cardiac imaging studies during health screening or preoperative test for noncardiac surgeries or by other imaging studies during the work-up for other medical conditions without obvious cardiac symptoms.
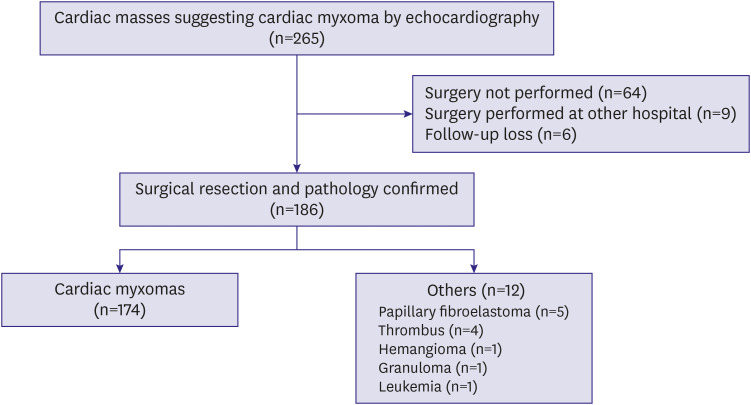 | Figure 1A flow diagram showing the number of patients diagnosed as cardiac myxomas by transthoracic echocardiography.
|
Table 1
Baseline clinical and laboratory characteristics of the participants
![]()
Dyspnea was the most frequent complaint in both symptomatic patents (67.0%) and those who were diagnosed as myxomas for other reasons (61.6%), and followed by chest pain, palpitation, dizziness and syncope (Table 1). Constitutional symptoms were reported in 7.2% of patients, and weight loss and fever were the 2 most common symptoms. Brain accounted for 91.2% of the embolized organs in 34 patients presenting as embolic complications, and the remainders were coronary artery (5.9%) and lower extremity (2.9%) (Table 2).
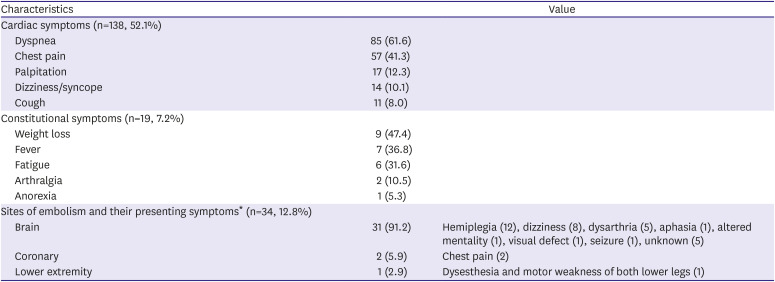
Table 2
Cardiac and constitutional symptoms and site of embolism
![]()
Tumor location and characteristics on echocardiography
Baseline echocardiographic findings were summarized in Table 3. All tumors were solitary. Width and height of the tumors were 38.7±19.8 mm (range, 4–96) and 26.0±12.0 mm (range, 3–67), respectively. Two-hundred and twenty-four (84.5%) myxomas were found in the LA cavity, in which fossa ovalis (83.5%) was the most frequent site, followed by lower septum (7.1%) and posterior wall (5.8%). Right atrium (RA) was the second most commonly involved chamber (8.3%), followed by left ventricle (LV, 1.5%) and right ventricle (RV, 1.5%). MV and tricuspid valve (TV) were involved in 3.4% and 0.8% of patients, respectively.
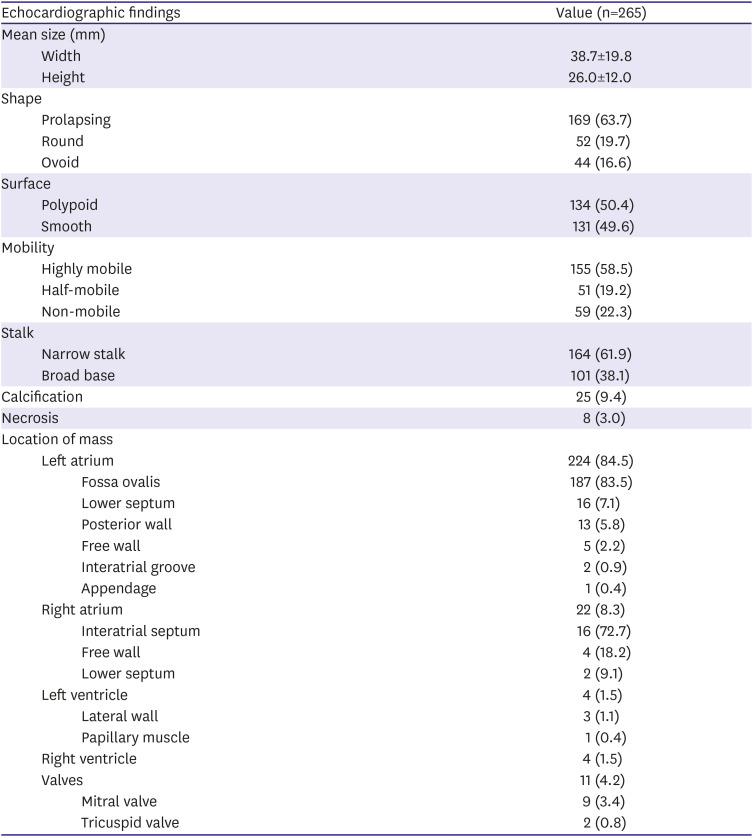
Table 3
Echocardiographic characteristics of the tumors
![]()
The proportion of myxomas with smooth and polypoid surface were almost identical (49.6% vs. 50.4%). Regarding the shape of the tumors, prolapsing tumors across the atrioventricular valves were most frequent (63.7%), followed by round and ovoid shape. Tumors with high mobility and narrow stalk accounted for 58.5% and 61.9%, respectively. MV obstruction resulting from the tumors was complicated in 21.9% of patients with 224 LA myxomas. Significant valvular regurgitation (≥moderate) was only reported in 8 patients (3.6%) with myxoma of the LA. Calcification and necrosis of the tumors were noted in 9.4% and 3.0% of patients, respectively.
Comparison of characteristics of myxomas and myxoma-mimicking other tumors
Surgical resection was performed in 195 patients (73.6%) and 186 of them were pathologically confirmed (Figure 1). Sixty-four patients (24.2%) did not undergo surgery due to refusal of surgery by patients and their families or due to poor medical condition associated with comorbidities. Six patients (2.3%) were lost to follow-up after the diagnosis.
Among 186 patients whose pathological diagnosis were identified, myxomas were confirmed in 174 patients (93.5%). Pathological diagnoses other than myxomas included 5 papillary fibroelastomas (PFEs, 2.7%), 4 thrombi (2.2%), 1 hemangioma (0.5%), 1 granuloma (0.5%) and 1 leukemia (0.5%). Of 174 myxomas, 169 (97.1%) were resected from the atria, 156 from LA (89.7%) and 13 from RA (7.5%), and remainders (2.9%) were removed from the RV, LV and TV. Thrombi were located in the LA in 3 patients (interatrial septum, posterior wall and appendage) and RA in 1 patient. PFEs were removed from the MV (2 patients), TV (1 patient) and LV wall (2 patients), and granuloma was resected from the MV. Hemangioma developed at the lower septum of the LA and leukemia was located at the free wall of the RA. Representative cases showing the difference between the typical myxoma and other tumors mimicking myxoma are shown in the Figure 2.
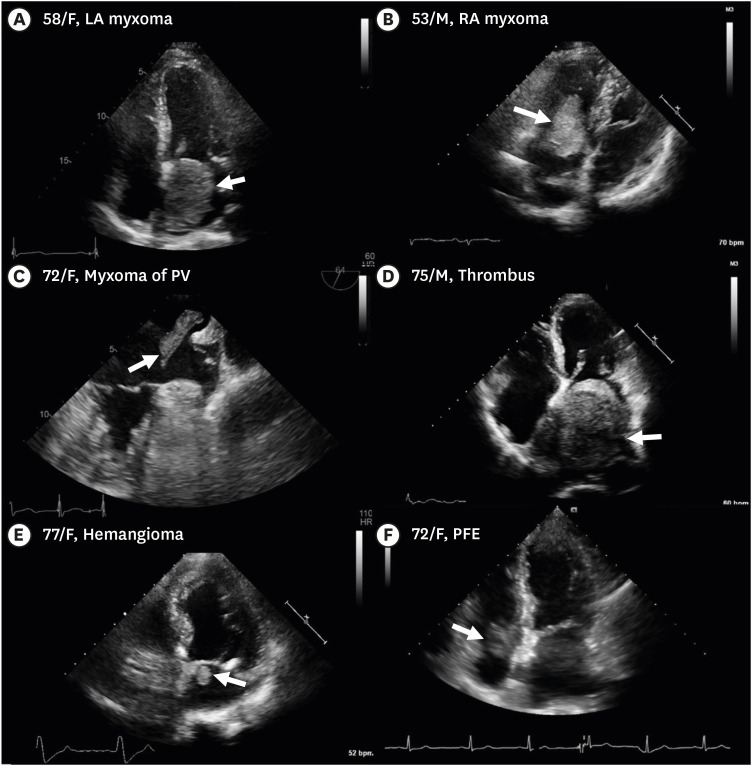 | Figure 2Representative cases. (A) An incidentally detected a 64×49 mm sized myxoma with smooth surface in the LA in a 58-year old woman. (B) A myxoma with polypoid surface in the RA prolapsing through the TV in a 53-year old man. (C) A transesophageal echocardiographic image showing an irregular shaped myxoma measured 34×9 mm in size originating from the left upper PV in the LA cavity in a 72-year old woman with a history of AF and cerebral infarction 3 years ago. (D) An 84×67 mm-sized mass-like thrombus in the LA in a 75-year old man with a history of AF presenting with abdominal pain. (E) A 14×13 mm-sized round echogenic mass below the medial mitral annulus in the LA in a 77-year old woman presenting with chest pain diagnosed as hemangioma. (F) A 22×21 mm-sized round mass proven to be a PFE below the septal leaflet of the TV in the RA in a 72-year old woman presenting with chest pain. Arrows indicate myxomas and masses mimicking myxoma.AF = atrial fibrillation; LA = left atrium; PFE = papillary fibroelastoma; PV = pulmonary vein; RA = right atrium; TV = tricuspid valve.
|
In comparison of patients with myxomas and those with other pathology, tumors or thrombi, symptoms including chest pain were more prevalent in patients with non-myxomas than in those with myxomas (Table 4). Tumors with pathological diagnosis other than myxomas were significantly smaller in width (20.4±13.9 mm vs. 41.4±19.8 mm, p=0.003) and height (12.6±7.7 mm vs. 27.6±11.5 mm, p<0.001) and less frequently found at the LA cavity (87.5% vs. 10.5%, p<0.001) than myxomas. The mean size of thrombi was comparable in width (56.3±22.5 mm vs. 41.4±19.8 mm, p=0.142) and larger in height (40.5±19.5 mm vs. 27.6±11.5 mm, p=0.030) than myxomas. All of the thrombi developed in the atria. Atrial fibrillation (AF) on electrocardiogram was more frequent (75% vs. 7.0%, p<0.001) and the anteroposterior diameter of the LA on TTE was larger (55.0±14.6 mm vs. 41.3±7.7 mm, p=0.001) in patients with thrombi than in those with myxomas.
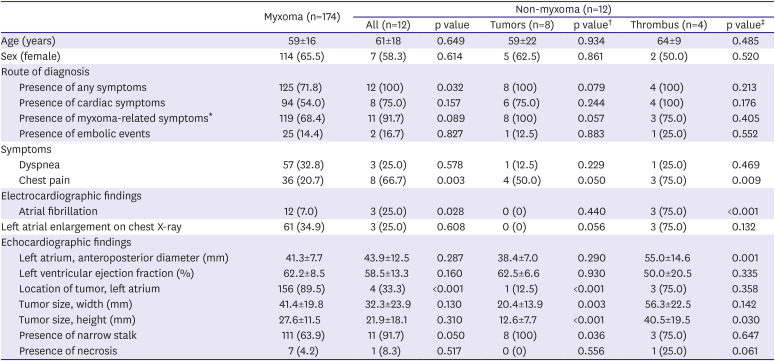
Table 4
Comparison of clinical and echocardiographic characteristics between cardiac myxoma and other etiologies
Values are presented as mean±standard deviation or number (%).
*Myxoma-related symptoms include cardiac or constitutional symptoms; †The p value was calculated between myxomas and non-myxoma tumors; ‡The p value was calculated between myxomas and thrombus.
![]()
Clinical course after diagnosis and/or surgery
The mean follow-up duration was 45.9±47.0 months in overall patients and 54.3±47.9 months in those who underwent surgery. Patients with final diagnosis of myxomas were followed up for 54.2±48.0 months.
Among 195 surgical patients, embolic stroke had developed in 3.6% (7 patients) during postoperative period (6 patients with LA myxoma, and 1 with PFE in the LV cavity). Among 189 surgical patients with sinus rhythm at baseline, postoperative AF developed in 25 patients in total (13.2%) and in 12.6%, 37.5% and 0% in patients with myxomas, other tumors and thrombus, respectively (p=0.096). Newly developed significant valvular regurgitation associated with the tumor after surgery in 187 patients with no or mild regurgitation of the corresponding valve at baseline was reported in 3 patients (1.6%), 2 with RA myxoma and 1 with PFE of the MV. Perioperative mortality rate was 2.1% (4 patients), 3 of which were patients with myxoma. No cardiovascular death was reported. Two died of pneumonia and one died of mediastinitis. Immediate postoperative death developed in one patient diagnosed with a mass in the RA cavity associated with acute lymphocytic leukemia. Six deaths (3.1%) had developed during follow-up after discharge and all of them were noncardiac death. The recurrence rate after surgical resection of myxomas was 1.1% (2 patients), 2 of 3 members in a family with Carney complex. No recurrence was reported in patients with non-myxoma.
In 64 patients who did not undergo surgery, mortality rate was 17.2% (11 patients) during the follow-up for 24.6±36.5 months. All of the known causes of death included non-cardiac causes such as malignancy or pneumonia.
Go to :
DISCUSSION
This is the largest multi-center study involving 265 patients who were diagnosed with myxomas by echocardiography. Among them, 67.1% were referred for echocardiography to evaluate cardiac symptoms or signs or source of embolism, and 30.9% of the tumors were incidentally detected during health screening or by other imaging studies. Dyspnea and chest pain were the 2 most frequent symptoms. Surgical resection and pathological confirmation were performed in 186 patients (70.2%) and 174 (93.5%) of them were identified as myxomas. Other cardiac tumors mistaken for myxomas developed at unusual sites including cardiac valves and showed smaller size than myxomas. Thrombi mimicking myxomas were as large as myxomas and were located in the atria.
Primary cardiac tumors have been reported at an incidence of 0.00138 to 0.03% and 80% of them are benign tumors.6)7) Cardiac myxomas have been well known as the most frequent primary benign cardiac tumors in adults accounting for 50–85% of them.2)7) TTE is a widely available, noninvasive diagnostic method for initial evaluation of cardiac myxomas. In recent years, various imaging studies including TTE are conducted for health screening. A recent study of Cianciulli et al.8) which examined 53 patients who underwent surgery for myxomas from 1993 to 2013 reported that 17% of the tumors were incidentalomas, while another study reported by Karabinis et al.9) that enrolled 153 surgical patients with myxomas from 1993 to 2017 described that 46.4% of patients were asymptomatic. Our current study showed that dyspnea was the most common symptom in symptomatic patients as previously reported,8)10) while 30.9% of patients were diagnosed as an incidentaloma without any cardiac or systemic symptoms. An additional analysis of patients diagnosed within the last 5 years and those diagnosed earlier found that the incidence of incidentalomas was significantly different, 45.8% and 21.9%, respectively, indicating that the incidence of myxomas as an incidentaloma is increasing in recent years.
Myxomas can masquerade as inflammatory or infectious diseases because they can be accompanied by constitutional symptoms such as fever or weight loss.11)12) They might also mimic the clinical characteristics of other cardiac tumors or atrial thrombi and vice versa.13)14)15)16) LA is the well-known, most prevalent site of myxomas with the incidence of 77–95% in recent studies,8)9)10)17)18) and 80% of which are attached to the interatrial septum (Table 5).2) Tumors other than myxomas found in the LA cavity might be confused with myxomas and myxomas involving the sites other than the LA may be mistaken for other tumors. Garatti et al.18) reported that among 102 patients with preoperative diagnosis of myxomas, 4 patients (3.9%) with LA tumors were confuted by pathology after surgery, 3 of which were found to be thrombus and one was primary cardiac sarcoma. This current study demonstrated that 4.2% of patients with preoperative echocardiographic diagnosis of myxomas were established to have other cardiac tumors than myxomas and 2.2% of the masses were proven to be atrial thrombus. Non-myxoma tumors were significantly smaller than myxomas and 75% of them were removed from atrioventricular valves or from the LV. All thrombi were removed from atria and had comparable or larger size than myxomas. Importantly, in patients with AF, the diagnosis of thrombus should be considered primarily, even if it mimics myxoma, because the prevalence of AF was significantly higher in patients finally diagnosed with thrombus than in those with myxomas. If a relatively small-sized tumor is found at a site other than atria, the first presumptive diagnosis should be one of non-myxoma cardiac tumors.
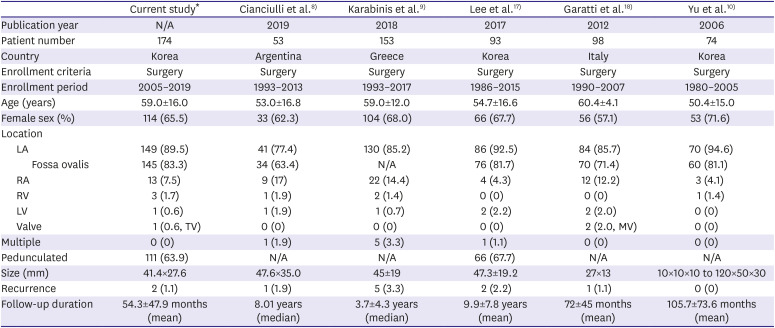
Table 5
Comparison of recent publications including patients with myxomas
| Current study* | Cianciulli et al.8) | Karabinis et al.9) | Lee et al.17) | Garatti et al.18) | Yu et al.10) | |||
|---|---|---|---|---|---|---|---|---|
| Publication year | N/A | 2019 | 2018 | 2017 | 2012 | 2006 | ||
| Patient number | 174 | 53 | 153 | 93 | 98 | 74 | ||
| Country | Korea | Argentina | Greece | Korea | Italy | Korea | ||
| Enrollment criteria | Surgery | Surgery | Surgery | Surgery | Surgery | Surgery | ||
| Enrollment period | 2005–2019 | 1993–2013 | 1993–2017 | 1986–2015 | 1990–2007 | 1980–2005 | ||
| Age (years) | 59.0±16.0 | 53.0±16.8 | 59.0±12.0 | 54.7±16.6 | 60.4±4.1 | 50.4±15.0 | ||
| Female sex (%) | 114 (65.5) | 33 (62.3) | 104 (68.0) | 66 (67.7) | 56 (57.1) | 53 (71.6) | ||
| Location | ||||||||
| LA | 149 (89.5) | 41 (77.4) | 130 (85.2) | 86 (92.5) | 84 (85.7) | 70 (94.6) | ||
| Fossa ovalis | 145 (83.3) | 34 (63.4) | N/A | 76 (81.7) | 70 (71.4) | 60 (81.1) | ||
| RA | 13 (7.5) | 9 (17) | 22 (14.4) | 4 (4.3) | 12 (12.2) | 3 (4.1) | ||
| RV | 3 (1.7) | 1 (1.9) | 2 (1.4) | 0 (0) | 0 (0) | 1 (1.4) | ||
| LV | 1 (0.6) | 1 (1.9) | 1 (0.7) | 2 (2.2) | 2 (2.0) | 0 (0) | ||
| Valve | 1 (0.6, TV) | 0 (0) | 0 (0) | 0 (0) | 2 (2.0, MV) | 0 (0) | ||
| Multiple | 0 (0) | 1 (1.9) | 5 (3.3) | 1 (1.1) | 0 (0) | 0 (0) | ||
| Pedunculated | 111 (63.9) | N/A | N/A | 66 (67.7) | N/A | N/A | ||
| Size (mm) | 41.4×27.6 | 47.6×35.0 | 45±19 | 47.3±19.2 | 27×13 | 10×10×10 to 120×50×30 | ||
| Recurrence | 2 (1.1) | 1 (1.9) | 5 (3.3) | 2 (2.2) | 1 (1.1) | 0 (0) | ||
| Follow-up duration | 54.3±47.9 months (mean) | 8.01 years (median) | 3.7±4.3 years (median) | 9.9±7.8 years (mean) | 72±45 months (mean) | 105.7±73.6 months (mean) | ||
Values are presented as mean±standard deviation or number (%).
LA = left atrium; LV = left ventricle; MV = mitral valve; N/A = not applicable; RA = right atrial enlargement; RV = right ventricle; TV = tricuspid valve.
*This analysis includes patients with pathologically proven myxomas.
![]()
This is a large scale, multi-center study, but has some limitations as a retrospective study. Scheduled clinical and echocardiographic follow-up was not performed and the recurrence rate might be underestimated. Follow-up period was relatively short (mean, 45.9±47.0 months; median, 29.9 months), especially in patients who did not undergo surgical resection. We could not accurately define the clinical course of the unremoved cardiac myxomas themselves because the majority of non-surgical patients could not undergo surgery because of their extremely old age, multiple comorbidities and poor medical conditions. Statistical significance can be underpowered due to a small number of patients with pathological diagnosis of thrombus and other tumors than myxomas. A larger prospective study can clarify the clinical course of the surgical and non-surgical patients with echocardiographic diagnosis of myxomas more clearly.
In conclusion, this study described clinical and echocardiographic characteristics of 265 patients with echocardiographic diagnosis of cardiac myxomas. Incidentalomas accounted for 30.9% in total and showed a trend of recent increment. Of the 73.6% (n=186) of overall patients who underwent surgery, 93.5% (n=174) were confirmed with myxomas among patients with pathologic confirmation (n=186). Patients with myxoma-like thrombus had a higher frequency of AF and LA enlargement, and the myxoma-like thrombus were located in the atria and comparable in size to myxomas. Non-myxoma cardiac tumors developed in unusual locations and were smaller than myxomas.
Go to :
 XML Download
XML Download