

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Angina pectoris is the leading symptom of coronary artery disease (CAD). It is caused by epicardial stenosis, microvascular dysfunction, vasoconstriction in the area of dynamic stenosis or by a combination of the above causes.1) The resulting ischemia of the heart muscle leads to the typical symptoms of angina pectoris.2)
CAD is the number one cause of death worldwide. It is estimated that 17.5 million people died of CAD in 2012, which means approximately 31% of all deaths worldwide.3) The main objectives of the treatment of stable CAD are the improvement of symptoms, tolerance to stress and quality of life, as well as the prevention of ischemia, myocardial infarction, heart failure and premature mortality. Nitrates are the preferred treatment for the symptoms of acute seizures, while beta-blockers are used for prevention.1) The oxygen demand of the myocardium is determined by cardiac work per unit time. There is a linear relationship, both at rest and during exercise. Important influencing factors are blood pressure and heart rate. Heart rate reduction is therefore an important goal for the prevention of angina and is considered an important mechanism of action of drugs recommended as first-line therapy for the treatment of angina in clinical guidelines.2)
Ivabradine has an anti-anginal mode of action for the symptomatic therapy of chronic CAD. The approval is limited as a reserve drug for patients with intolerance or contraindication to beta-blockers. It may be used in combination with beta-blockers in patients who are insufficiently adjusted with an optimal beta-blocker dose. Acting as If channel inhibitor, ivabradine has a solely negative chronotropic effect. The cardiac effects are sinus node-specific and have no influence on intraatrial, atrioventricular or intraventricular transmission. Myocardial contractility and ventricular repolarisation remain unchanged. Ivabradine reduces myocardial oxygen demand through heart rate reduction, which makes its use interesting in patients with pectanginal complaints.4)
To date, national and international professional associations have rated the class of recommendation as IIa with evidence level B for the therapeutic use of ivabradine.2) The current European Society of Cardiology (ESC) guideline on the management of stable CAD2) is solely based on a brief narrative of 4 studies.5)6)7)8) Even the reviews of the recent years are limited due to a small selection of outcomes and unspecific inclusion criteria: Ye et al.9) compared the exercise capacity of 7 studies, while Mengesha et al.10) pooled 3 studies with a follow-up (FU) period of at least 1 year including also patients with heart failure. The present review has identified and systematically evaluated—additionally to the 4 studies of the current ESC guidelines—8 more studies on the use of ivabradine in angina pectoris.11)12)13)14)15)16)17)18)19) With its broader spectrum of outcomes and the inclusion of non-English publications, it clearly outperforms other reviews of recent years. At the same time, it has examined whether the negative results of Study assessInG the morbidity-mortality beNefits of the IF inhibitor ivabradine in patients with coronarY artery disease (SIGNIFY)12) related to the composite outcome of cardiovascular death or non-fatal myocardial infarction are confirmed in the new literature. In SIGNIFY (n=12,049), a statistically significant increase in the combined outcome was observed in a predetermined subgroup, Canadian Cardiovascular Society (CCS) class ≥II, of patients with symptomatic angina pectoris: 7.6% vs. 6.5% with placebo; hazard ratio [HR], 1.18; 95% confidence interval [CI], 1.03, 1.35; p=0.02. Individually, the components of the outcome were not significantly elevated. Thus, this work makes an important contribution to optimal patient care in angina pectoris and decisively supplements the current guideline.
METHODS
The present systematic review was conducted in accordance with the guidance provided by the Cochrane Collaboration20); the protocol was published in advance on PROSPERO (CRD42017062404).
Systematic literature search
The systematic literature search was carried out in November 2019 in the following electronic databases:
1. Cochrane Central Register of Controlled Trials (CENTRAL, 2018, issue 6) of the Cochrane Library
2. MEDLINE (Ovid, 1946 to November 2019)
3. Embase (Ovid, to November 2019)
4. Web of Science Core Collection (Thomson Reuters, 1900 to November 2019).
The search terms “ivabradine” and “angina pectoris” were applied in the known variations as well as the corresponding MeSH term. This includes ‘stable angina’, ‘angina pectoris’ as well as ‘angina’ only. A search for ‘ischemia’ was not conducted to avoid too unspecific search results. No restrictions were defined regarding publication language or publication period. In addition, the 2 databases ClinicalTrials.gov (https://www.ClinicalTrials.gov) and the search database of the International Health Trial Registry of the World Health Organisation were searched for suitable studies (https://apps.who.int/trialsearch/). Furthermore, the reference lists of the included studies have been checked for additional studies and authors of included studies have been contacted due to missing data.
Inclusion criteria
Study type: randomised controlled trials (RCTs), published as full text or abstract only.
Population: patients (≥18 years) with chronic, stable angina pectoris.
Intervention and comparison: ivabradine versus placebo and ivabradine versus other anti-anginal drugs.
Data selection and extraction
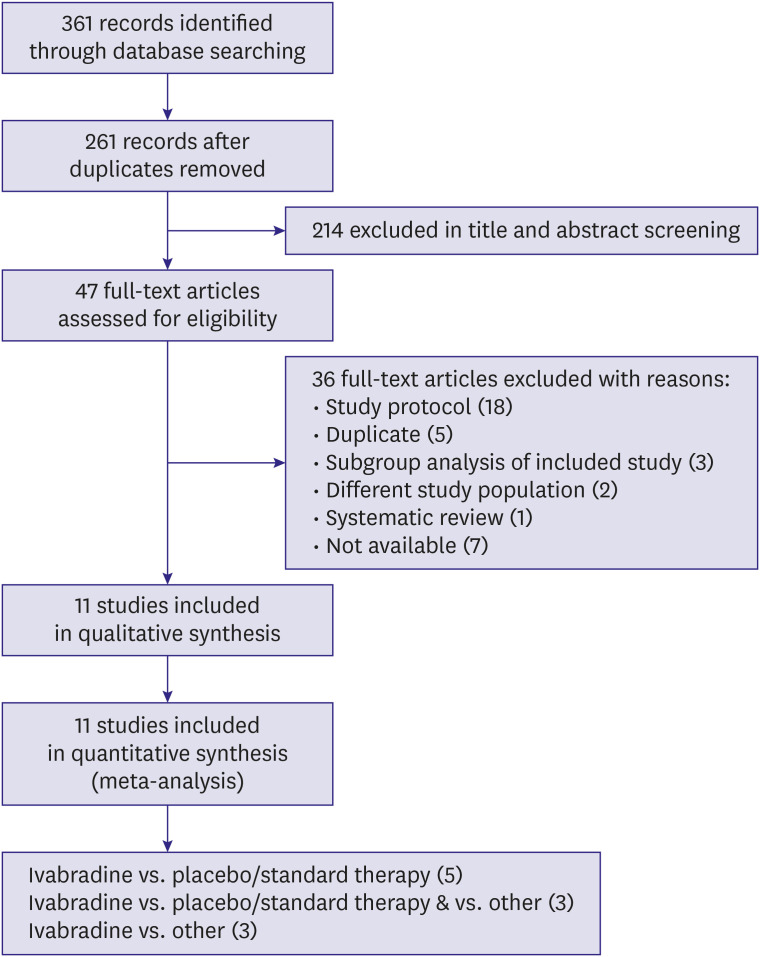
Citations from electronic databases were imported into the reference management software Endnote (version X7) and duplicates were deleted. Two authors (CK, CB) independently searched all matches based on title and abstract and classified them as "included" or "excluded". For all studies marked as "included" by both authors, the full text was then evaluated by 2 independent authors (CK, CB). The selection process is described in detail in a flowchart (Figure 1).
Figure 1
Study flow diagram. The study flow diagram shows the number of included studies over the entire process of screening.
A specially developed data extraction protocol was used for data extraction, which had previously been successfully tested in one of the included studies. The data extraction was performed by one author (CK) and independently controlled by another author (CB).
Risk of bias assessment
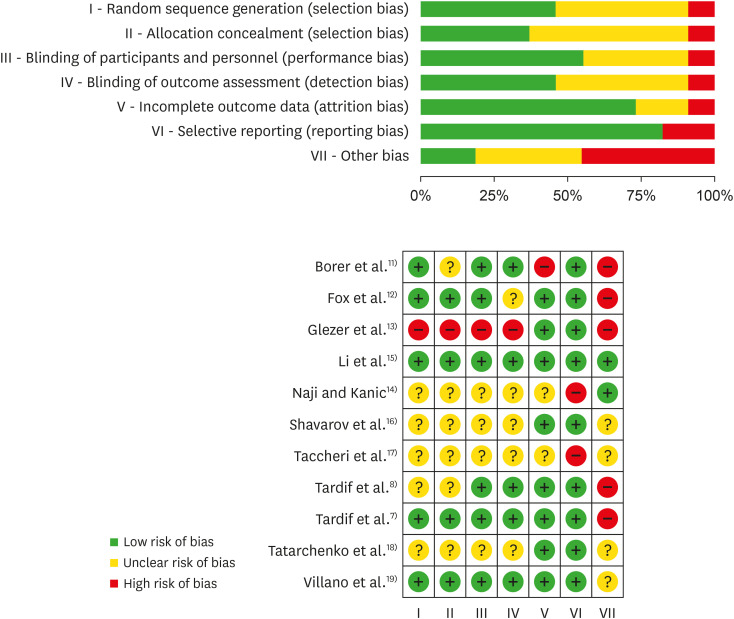
Two authors (CK, CB) independently assessed the risk of bias for each study according to the criteria stated in the Cochrane Manual.20) Seven risk of bias domains were identified.
1. Random sequence generation (selection bias)
2. Allocation concealment (selection bias)
3. Blinding of participants and personnel (performance bias)
4. Blinding of outcome assessment (detection bias)
5. Incomplete outcome data (attrition bias)
6. Selective reporting (reporting bias)
7. Other bias
We assessed each potential source of bias as high, low or unclear and provided a quote from the study report together with a justification for our judgement (results, section risk of bias assessment, and Figure 2).
Evaluation of statistical heterogeneity
When pooling the data by meta-analysis, statistical heterogeneity was evaluated by visual inspection of the forest plot, supplemented by the χ2 test, τ2 and I2 statistics.20)
Meta-analyses and statistics
Meta-analyses were done only where this was meaningful, i.e. if the treatment, participants and the underlying clinical question were similar enough for pooling to make sense. If the average treatment effect was not clinically meaningful, trials were not combined. The statistical analysis was carried out using the RevMan 5 programme.21) Dichotomous data were analysed as risk ratios with 95% CIs. For continuous data, the weighted mean difference (WMD) with 95% CI for outcomes measured in the same way between trials was used.
Due to the identified clinical heterogeneity between individual studies (e.g. duration of ivabradine use, severity of angina pectoris, co-medications), meta-analysis was performed based on the random effects model. The average treatment effect is presented. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system recommended by Cochrane to evaluate the quality of evidence level (GRADE QoE) for each outcome was applied.20)
RESULTS
Results of the systematic search
The systematic literature search in electronic databases resulted in a total of 361 publications. After removal of 100 duplicates, another 214 publications were excluded after title and abstract screening. Of the remaining 47 studies, 36 were found unsuitable after examination of the full texts, so that 11 studies fulfilled the inclusion criteria for qualitative and quantitative analysis.7)8)11)12)13)14)15)16)17)18)19) A schematic illustration of the search process as a flowchart including a detailed breakdown of the individual reasons for exclusion is shown in Figure 1.
Characteristics of included studies
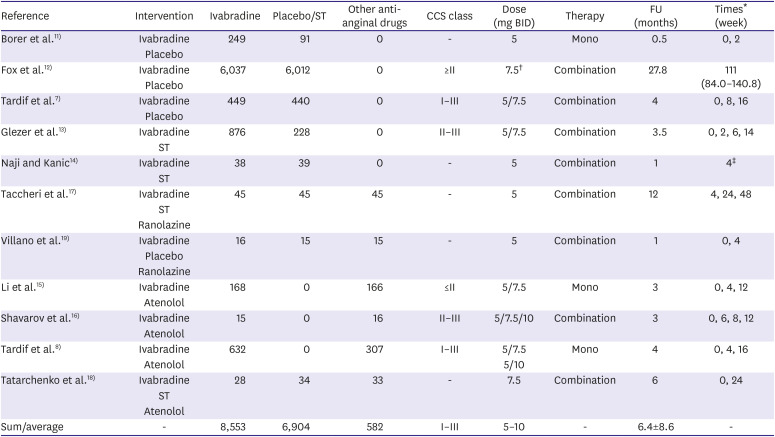
A total of 16,039 patients were assessed with an average FU time of 6.4±8.6 months, with the period of FU corresponding to the duration of ivabradine treatment. Overall, 8,553 patients received ivabradine, 6,904 patients received placebo or standard therapy (ST) and 582 patients received other anti-anginal drugs (atenolol, ranolazine). CCS class ranged from I to III, while the average age was 59.5±3.4 years. Table 1 summarises the main characteristics of the included studies. Supplementary Data 1 provides a detailed tabular overview of all studies included. Regarding study design, we want to highlight that 5 studies14)16)17)18)19) considered very small case numbers (average n=30 per group).
Table 1
Characteristics of included studies
| Reference | Intervention | Ivabradine | Placebo/ST | Other anti-anginal drugs | CCS class | Dose (mg BID) | Therapy | FU (months) | Times* (week) |
|---|---|---|---|---|---|---|---|---|---|
| Borer et al.11) | Ivabradine | 249 | 91 | 0 | - | 5 | Mono | 0.5 | 0, 2 |
| Placebo | |||||||||
| Fox et al.12) | Ivabradine | 6,037 | 6,012 | 0 | ≥II | 7.5† | Combination | 27.8 | 111 (84.0–140.8) |
| Placebo | |||||||||
| Tardif et al.7) | Ivabradine | 449 | 440 | 0 | I–III | 5/7.5 | Combination | 4 | 0, 8, 16 |
| Placebo | |||||||||
| Glezer et al.13) | Ivabradine | 876 | 228 | 0 | II–III | 5/7.5 | Combination | 3.5 | 0, 2, 6, 14 |
| ST | |||||||||
| Naji and Kanic14) | Ivabradine | 38 | 39 | 0 | - | 5 | Combination | 1 | 4‡ |
| ST | |||||||||
| Taccheri et al.17) | Ivabradine | 45 | 45 | 45 | - | 5 | Combination | 12 | 4, 24, 48 |
| ST | |||||||||
| Ranolazine | |||||||||
| Villano et al.19) | Ivabradine | 16 | 15 | 15 | - | 5 | Combination | 1 | 0, 4 |
| Placebo | |||||||||
| Ranolazine | |||||||||
| Li et al.15) | Ivabradine | 168 | 0 | 166 | ≤II | 5/7.5 | Mono | 3 | 0, 4, 12 |
| Atenolol | |||||||||
| Shavarov et al.16) | Ivabradine | 15 | 0 | 16 | II–III | 5/7.5/10 | Combination | 3 | 0, 6, 8, 12 |
| Atenolol | |||||||||
| Tardif et al.8) | Ivabradine | 632 | 0 | 307 | I–III | 5/7.5 | Mono | 4 | 0, 4, 16 |
| Atenolol | 5/10 | ||||||||
| Tatarchenko et al.18) | Ivabradine | 28 | 34 | 33 | - | 7.5 | Combination | 6 | 0, 24 |
| ST | |||||||||
| Atenolol | |||||||||
| Sum/average | - | 8,553 | 6,904 | 582 | I–III | 5–10 | - | 6.4±8.6 | - |
Risk of bias of included studies
Overall, potential risk of bias across included studies ranged from low in case of selective reporting and incomplete outcome data to high in terms of other bias. The letter was mainly due to conflict of interests concerning financial support from the manufacturer.7)8)11)12)13) The overall lowest risk of bias with 7 of 7 low risk domains was assessed for Li et al.,15) the overall highest risk of bias with 5 of 7 high risk domains was assessed for Glezer et al.13) The assessment of the risk of bias for each study using the criteria presented in the Cochrane Manual20) is outlined in Figure 2. A detailed description can be found in Supplementary Data 2.
Results of the outcome analysis
An overview of results can be found in Table 2.
Table 2
Summary of results for all outcomes and comparisons
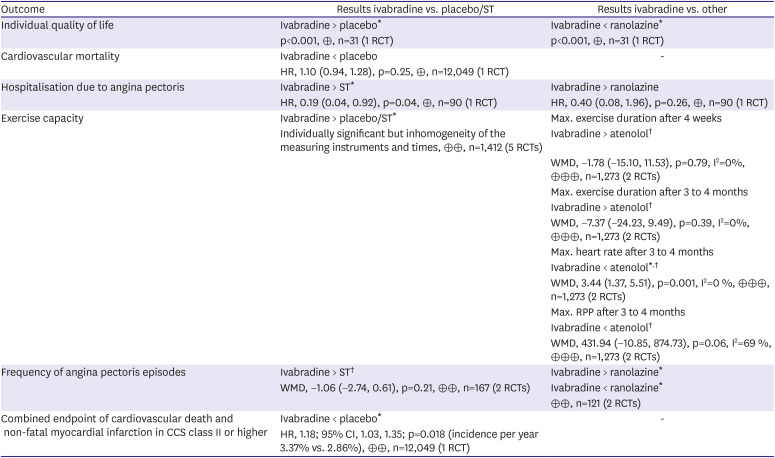
Grading of Recommendations Assessment, Development and Evaluation: ⊕ = very low; ⊕⊕ = low; ⊕⊕⊕ = moderate; ⊕⊕⊕⊕ = high.
CCS = Canadian Cardiovascular Society; CI = confidence interval; HR = hazard ratio; RCT = randomized controlled trial; ST = standard therapy; WMD = weighted mean difference.
*Significant; †Meta-analysis.
Comparison 1: ivabradine versus placebo/standard therapy
2) Cardiovascular mortality
Only one study12) investigated cardiovascular mortality in a total of 12,049 patients. Ivabradine showed no effect on cardiovascular mortality. The cardiovascular death rate in the ivabradine group within an average observation period of 27.8 months was 3.4%, slightly more than the death rate of 3.2% in the placebo group (HR, 1.10; 95% CI, 0.94, 1.28; p=0.25, not significant).
3) Hospitalisation due to angina pectoris
Hospitalisation due to angina pectoris was investigated in one study (n=90).17) In contrast to 2 patients of the ivabradine group (4%), 9 patients (20%) of the ST group had to be hospitalised again within 12 months (HR, 0.19; 95% CI, 0.04, 0.92; p=0.04; statistically significant) due to worsening angina pectoris symptoms. In this small cohort ivabradine showed effects on the hospitalisation rate, however, Taccheri et al.17) report their study results only in the form of a short abstract, thus, the risk of bias cannot be conclusively evaluated.
4) Exercise capacity
Five studies7)11)17)18)19) examined the exercise capacity of patients with angina pectoris. All studies showed a significant advantage of ivabradine over placebo or ST. However, a comparative meta-analysis of the data is not possible due to heterogeneity of outcome definition and measurement (cf. Supplementary Table 1), thus the GRADE QoE was assessed as low.
5) Frequency of angina pectoris episodes
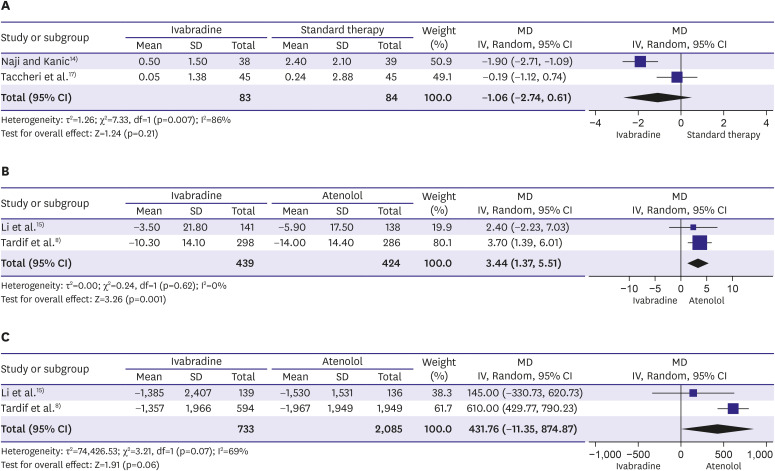
Two studies14)17) examined the frequency of angina pectoris episodes in a total of 168 patients in comparison between ivabradine and ST after one month. Here, the results of individual studies are not congruent, Naji and Kanic14) see a significant reduction by an average of 79% per week while Taccheri et al.17) observe no effect. Meta-analysis of these data shows that, on average, ivabradine has no statistically significant effect on the frequency of angina pectoris episodes (WMD, −1.06; 95% CI, −2.74, 0.61; p=0.21, GRADE QoE low) (Figure 3A).
Figure 3
Forest plot analyses. (A) The frequency of angina pectoris episodes after one month comparing ivabradine vs. standard therapy; (B) The exercise capacity measured by the decrease of the maximum heart rate after 3 to 4 months comparing ivabradine vs. atenolol; (C) Exercise capacity measured by the decrease of the RPP after 3 to 4 months comparing ivabradine vs. atenolol.
CI = confidence interval; MD = mean difference; RPP = rate pressure product; SD = standard deviation.
6) Combined endpoint of cardiovascular death and non-fatal myocardial infarction in CCS class II or higher
In addition to SIGNIFY,12) 2 other studies have also included patients with CCS class II or higher in their clinical studies,13)16) but none of both studies measured the combined outcome of cardiovascular death and non-fatal myocardial infarction. Furthermore, none of the other studies performed a pre-defined subgroup analysis for the CSS class,7)8)11)14)15)16)17)18)19) hence the negative results of SIGNIFY for the CSS class II patient group or higher cannot be supplemented.
Comparison 2: ivabradine versus other anti-anginal drugs
1) Individual quality of life
A total of 6 studies8)15)16)17)18)19) compared ivabradine with other anti-anginal drugs, of which one study (n=31)19) investigated the individual quality of life of patients. Both the SAQ score22) and the EuroQoL VAS23) improved significantly (p<0.01) in the ivabradine and ranolazine groups from baseline to FU after 4 weeks. Overall, ranolazine showed better results for different SAQ and EuroQoL VAS levels than ivabradine (p<0.05) in this very small cohort of patients.
2) Cardiovascular mortality
None of the studies investigated cardiovascular mortality compared to other anti-anginal drugs.
3) Hospitalisation due to angina pectoris
Hospitalisation due to angina pectoris was investigated in one study (n=90).17) Ivabradine showed no relevant effects. Two patients in the ivabradine group (4%) and 5 patients in the ranolazine group (9%) had to be hospitalised again within 12 months due to worsening angina pectoris symptoms (HR, 0.40; 95% CI, 0.08, 1.96; p=0.26; not significant).
4) Exercise capacity
Six studies8)15)16)17)18)19) compared the exercise capacity of patients with angina pectoris between ivabradine and other anti-anginal substances. However, due heterogeneity of outcome definition and measurement, only the data from Li et al.15) and Tardif et al.8) can be combined in a meta-analysis (ivabradine vs. atenolol, n=1,273). Both studies documented the change in maximum exercise duration and time to 1-mm ST segment depression after 4 weeks and after 3 to 4 months as well as the change in maximum heart rate and the rate pressure product (RPP) after 3 to 4 months. With a WMD of −1.78 (−15.10, 11.53), however, no significant difference between ivabradine and atenolol after 4 weeks (p=0.79, I2=0%; not significant) or after 3 to 4 months (p=0.39, I2=0%; not significant) can be determined on average with respect to the maximum exercise duration. In contrast, reduction of the maximum heart rate and RPP after 3 to 4 months shows, on average, an advantage for atenolol in the meta-analysis (WMD, 3.44; 95% CI, 1.37, 5.51; p=0.001; I2=0% and WMD, 431.94; 95% CI, −10.85, 874.73; p=0.06, I2=69%, respectively) (Figure 3B and C). The GRADE QoE was assessed as moderate.
5) Frequency of angina pectoris episodes
Two studies (n=121) examined the frequency of angina pectoris episodes in comparison between ivabradine and ranolazine after 1 month.17)19) In both studies, the administration of ivabradine resulted in a reduction of angina pectoris episodes per week. However, Taccheri et al.17) described an advantage for ivabradine (ivabradine 0.05 vs. ranolazine 0.09 angina pectoris episodes per week, p=0.04), while Villano et al.19) showed an advantage for ranolazine (ivabradine 73.1±18 vs. ranolazine 81.3±17 SAQ points, p=0.001). A combination of the study data in a meta-analysis could not be performed due to the different measurement parameters and missing data.
DISCUSSION
The present systematic review and meta-analysis comprises 11 studies with a total of 16,039 patients with stable angina pectoris, of which 8,553 patients received ivabradine, 6,904 patients received placebo or ST and 582 patients received other anti-anginal drugs (atenolol, ranolazine). The sample size varied between 31 and 12,094 patients. Noteworthy, almost half of the included studies considered only very small case numbers (on average n=30 per group). The ivabradine dose administered was 5 mg, 7.5 mg or 10 mg bis in die (BID), with 10 mg BID noticeably above the manufacturer's recommended maximum daily dose.4) The intervention time with ivabradine differs severely from 2 weeks to 35 months.
Positive effects of ivabradine were observed in few studies with very small case numbers. A comparison between ivabradine and placebo in one study (n=31) showed significant benefits for ivabradine in terms of individual quality of life.19) The GRADE QoE was evaluated as very low due to the small case number and publication bias. One study (n=90) documented significant benefits in hospitalisation duration for ivabradine versus ST.17) Here as well, the GRADE QoE can be assessed as very low due to unclear risk of bias. Five studies7)11)17)18)19) showed statistically significant advantages of ivabradine versus placebo or ST in terms of exercise capacity. However, a meta-analysis was not possible due to heterogeneity of outcome definition and measurement. Regarding the frequency of angina pectoris episodes, our meta-analysis of 2 studies14)17) did not show, on average, a significant benefit of ivabradine versus ST. Studies' GRADE QoE was also assessed as low. The largest manufacturer-sponsored multicentre study in more than 12,000 CAD patients, SIGNIFY,12) showed no significant effect of ivabradine on cardiovascular mortality. The negative results of SIGNIFY12) in the group of patients with CCS class II or higher (n=12,049) with a statistically significant increase in the combined outcome of cardiovascular death and non-fatal myocardial infarction under ivabradine currently provide the best and most comprehensive evidence leading to a critical consideration concerning the use of ivabradine in this patient population. Furthermore, the data indicated a higher risk of bradycardia with ivabradine compared with placebo (17.9% vs. 2.1%) as well as an increase in the absolute incidence of atrial fibrillation by 0.7%.12) One reason for these negative outcomes of SIGNIFY might be the higher dosage of 10 mg BID in some patients, even though, an audit of the data by the European Medicines Agency (EMA) revealed that this higher dose did not fully explain the findings.24) To reduce this risk the EMA gives the following recommendations: dosage of 5 to 7.5 mg BID, no combination with verapamil or diltiazem (inhibitors of cytochrome P450 P3A4), and sole use in angina patients in sinus rhythm with a heart rate ≥70 bpm who remain symptomatic despite anti-anginal therapy. The data from SIGNIFY did not demonstrate a beneficial effect for ivabradine in CAD patients without clinical heart failure, but only for patients with chronic stable angina pectoris who cannot be treated with beta-blockers, or in combination if beta-blockers alone are not sufficient.24)
Compared to other anti-anginal substances, one study (n=31) showed a significant disadvantage of ivabradine versus ranolazine in terms of individual quality of life.19) There was neither a reduction in hospitalisation duration17) nor a significant influence on exercise capacity compared to atenolol.8)15) In contrast, exercise duration could be positively influenced and reduced more, on average, by atenolol than by ivabradine.8)15) The analysis of frequency of angina pectoris episodes compared to ranolazine showed diametrically opposed results in Taccheri et al.17) and Villano et al.19)
Overall, there is no convincing evidence for significant advantages of ivabradine compared to other anti-anginal substances. We acknowledge that these results contrast current literature as Kaski et al.25) and Werdan et al.,26) who summarised that ivabradine represents a useful agent for the symptomatic treatment of patients with angina pectoris, even in relation to different subgroups as monotherapy, combination therapy, elderly, comorbidities, revascularisation and CAD without heart failure25) as well as CCS classification, medical history and medication.26) Their statements should be interpreted with caution as these reviews refer not only to RCTs but mainly to observational studies. Until today, no RCT has been performed scoping the subgroups elderly, comorbidities, or revascularisation. CAD without heart failure can only be covered by SIGNIFY12) unless one refers to post hoc analyses of BEAUTIFUL27) and SHIFT,28) or Amosova et al.,29) which was excluded in the present systematic review in consequence of the inappropriate study design (missing comparability due to uptitration of beta-blockers). The examination of ivabradine in combination with beta-blockers is strongly represented7)12)13)14)16)17)18)19) while only Borer et al.,11) Tardif et al.8) and Li et al.15) examine the monotherapy of ivabradine (Table 1). Borer et al.11) showed significant advantages of ivabradine versus placebo in exercise capacity while Tardif et al.8) and Li et al.15) demonstrate significant disadvantages in exercise capacity vs. atenolol (WMD, 3.44; 95% CI, 1.37, 5.51; p=0.001; I2 = 0% and WMD, 431.94; 95% CI, −10.85, 874.73; p=0.06, I2=69%, respectively) (Figure 3B and C) as well as slightly less reduction in the number of angina attacks (−2.2±4.3 vs. −2.7±12.3).8) This data is in line with the recommendations by the EMA to use ivabradine only if the patient cannot be treated with beta-blockers, or in combination if beta-blockers alone are not sufficient.24) This conclusion is also supported by the consensus statement of Ferrari et al.30) emphasising the synergistic effects of beta-blockers and ivabradine. In contrast to Kaski et al.25) and Werdan et al.,26) latter draws its statements from RCTs7)8)11)12)27)29) demonstrating—similar to the data which current guidelines1)2)3) are based—that there is a great lack of randomised, double-blind, investigator-initiated studies with patient-centred, functional outcomes in an adequately large patient population.
Regarding the reliability of the results, the overall large patient population and similar study characteristics can be highlighted positively. With few exceptions, this led to a negligible statistical heterogeneity of the data. In addition, most studies showed a low to moderate risk of bias. However, some data with respect to randomisation and blinding were missing, so that an adequate assessment of a possible bias was not feasible for all included studies. Another major obstacle in the analysis of the studies is the heterogeneity of outcome definition and measurement. Those varied considerably, especially with regard to exercise capacity. In order to achieve maximum comparability despite the lack of patient-centred functional outcomes, the original protocol was extended by the outcome "frequency of angina pectoris episodes". Otherwise, the original protocol was not changed and strictly adhered to the Cochrane rules, which on the one hand resulted in only a small number of data that we could pool, but on the other hand made these results consistently reliable and dependable.
In conclusion, this systematic review and meta-analysis make an important contribution to optimal patient care in angina pectoris and decisively complements the current ESC guidelines with 8 further studies, whose recommendation IIa so far could only be given with evidence level B for the therapeutic use of ivabradine on the management of stable CAD.2) Overall, the results of the present work are in line with the recommendations by the EMA to use ivabradine only if the patient cannot be treated with beta-blockers, or in combination if beta-blockers alone are not sufficient.
 XML Download
XML Download