

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the beginning of medical science, observation of the “real-world” experience has been a common traditional method to develop new medical therapies. The use of randomized clinical trials (RCTs) has now become the gold standard for proving the efficacy and safety of novel treatments. The evidence generated by this clinical trial model has replaced real-world evidence (RWE) and practice-based observations. The data acquired from RCTs have many advantages, including high internal and external validity, completeness of data, and adjudication of events predefined on study protocols. However, in reality, we frequently encounter diverse and heterogeneous patients in clinical practice, who are not included in RCTs. Patients who are very old, having extreme bodyweight, concomitant medications, and multimorbidities pose a challenge due to a lack of evidence to guide clinical practice. Limited representativeness, high costs, long study duration, and risk of failure pose further challenges for RCTs. Non-randomized observational studies would complement the weaknesses of RCT by providing supplementary data. Moreover, these comprehensive datasets represent large populations, thus, including participants otherwise excluded from RCTs. ‘Real-world’ observation studies use several types of data sources, including regulatory sponsored studies, registries sponsored by learned societies, nationwide cohorts, claims data, investigator-initiated and industry-sponsored studies, and hospital cohorts.1) Electronic medical records have now become the standard method to collect patient data and for administrative work regarding reimbursement and payment. This exponential growth of data is gaining tremendous interest as a novel research tool.
Furthermore, the 21st Century Cures Act (Cures Act) requires the Food and Drug Administration (FDA) to develop programs aimed at accelerating the development of drugs and medical devices. This will also guide the evaluation of RWE to support the approval of previously approved drugs or to fulfill the post-approval study requirements. The FDA is now working on generating evidence supporting the effectiveness and safety of RWE, supporting the findings of RCTs in real-world settings, and developing programs using electronic health records. Appropriate use of the data requires adequate knowledge of the characteristics of the database. Therefore, we sought to summarize the structure of the Korean National Health Information Database (NHID). We also aimed to summarize the findings of recent studies in the field of cardiovascular science, which would be of particular interest to researchers interested in using the NHID data as a new tool to prove their hypotheses.
BASICS OF THE KOREAN NATIONWIDE CLAIMS DATABASE
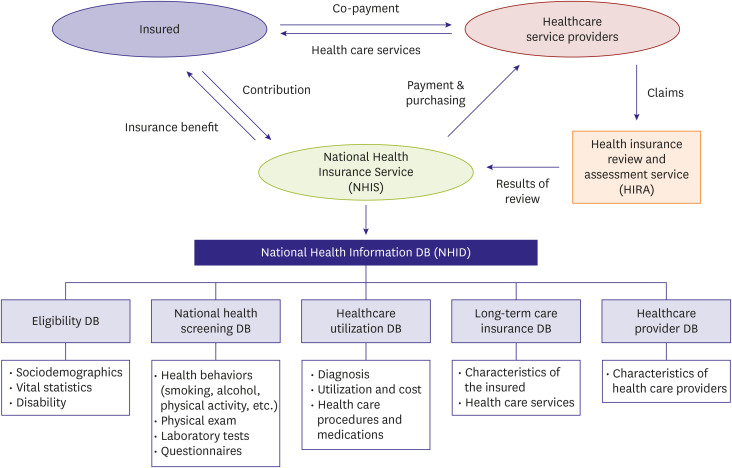
South Korea (hereafter, Korea) implements a single-payer, universal, mostly fee-for-service, and compulsory healthcare insurance system. The National Health Insurance (NHI) system includes the insured, the healthcare providers, and the regulators of the healthcare system, constituting the National Health Insurance Service (NHIS), Health Insurance Review Agency (HIRA), and Ministry of Health and Welfare (Figure 1).2) Those insured by NHI pay monthly insurance contributions for medical services provided by health care providers. The medical aid program covers low-income households with a minimum livelihood. The NHI program managed by NHIS, Medical Aid for low income groups, and long-term care insurance cover 100% of the Korean population, which was approximately 52 million in 2019. Since the NHIS pays costs based on the billing records of health care providers, the NHIS created a database to collect the required information on insurance eligibility, insurance contributions, medical history, and medical institutions. The NHI program provides health care benefits, including diagnosis, laboratory tests, drugs, medical materials, treatment, surgery, rehabilitation, hospitalization, nursing, and transportation by healthcare providers, and health screening services.2)
STRUCTURE OF THE KOREAN NATIONAL HEALTH INSURANCE DATABASE
The Korean NHIS constructed the nationwide claims database called the Korean National Health Insurance Database (NHID),3) which consists of five databases, namely the eligibility database, national health screening database, health care utilization database, long-term care insurance database, and health care provider database (Figure 1).
The eligibility database contains information, including sociodemographic data, use of inpatient and outpatient services, pharmacy dispensing claims, and data of death, compiled by Statistics Korea. The annual reports of Statistics Korea reported a 92% accuracy of cause of death.4)
The national health screening database constitutes detailed lifestyle questionnaires, laboratory results, and anthropometric measurements. Health screening programs comprise general national health screening, health screening program for transitional ages (those aged 40 and 66 years), early childhood health screening program, and cancer screening programs.5) All insured Koreans aged 40 years or older, and their dependents are recommended to undergo biannual general health screening without cost. The participation rate of the general health screening program among eligible participants was 74.8% in 2014.6)
The health care utilization database includes information regarding inpatient and outpatient usage and prescription records, which is the largest component of the NHID. Diagnoses were coded in compliance with the Korean Standard Classification of Diseases (KCD) Version 6, which is based on the International Classification of Diseases 10th Revision (ICD-10). However, diagnoses are currently coded as per KCD7, introduced in 2016.
The long-term care insurance database constitutes information on functional assessment, including physical function, nursing, unique treatments, behavioral symptoms, cognitive function, and rehabilitation needs of the beneficiaries.
The health care provider database includes information regarding health care institutions, health care professionals, and equipment. The database contains de-identified personal information to ensure anonymity. NHI system does not cover medical services conducted for cosmetic purposes. Additionally, information regarding new drugs and procedures that are not covered by the NHI system is not included in the NHID.
KOREAN NATIONAL HEALTH INSURANCE SERVICE - NATIONAL SAMPLE COHORT
Since the size of the NHID is too large, which limits usability and accessibility, the NHIS constructed a representative sample database called NHIS-National Sample Cohort (NHIS-NSC).5)7) NHIS-NSC constitutes approximately a million participants, 2.2% of the total eligible population, who were randomly sampled from the 2002 NHID, and followed for 11 years, until 2013. NHIS-NSC includes information regarding participants' eligibility, history of medical treatment, healthcare providers, and general health screening information.
HEALTH INSURANCE AND REVIEW ASSESSMENT DATABASE
Since the size of the NHID is too large, which limits usability and accessibility, the NHIS constructed a representative sample database called NHIS-National Sample Cohort (NHIS-NSC).8) Researchers have been provided access to the HIRA data since 2009, which was accelerated by promoting “Opening and Sharing Big Data for Value Creation” in 2013. The HIRA data constitutes six files, namely the general information file; healthcare services file, which include inpatient prescriptions; diagnoses file; outpatient prescriptions file; drug master file; and provider information file.8)
Although HIRA data uses the same claims data as the NHID, there are several differences. HIRA data could be analyzed only for a 5-year period beginning from the current year. Recently, this restriction of HIRA data has been changed to the limitation of data size. If the data size is within the limitation, data would be available from 2007. Moreover, HIRA data does not include health screening data, thereby excluding lifestyle questionnaires, laboratory data, and anthropometric information. Further, the mortality data compiled by Statistics Korea was not linked to HIRA data, thus, mortality data could not be analyzed. However, HIRA data does analyze in-hospital death. The eligibility database of the NHID is also not linked to HIRA, thus, HIRA data excludes detailed information regarding participant eligibility.
STRENGTHS AND LIMITATIONS OF THE NHID
The NHID has several strengths (Table 1). First, since the NHID constitutes data for more than 52 million people, it is one of the largest claims datasets. The NHID also contains data regarding all age groups and the entire region, which reduces the possibility of selection bias. Moreover, the NHID is different from the Medicare and Medicaid program of the United States, which are restricted to either elders or those with low income. Second, the NHID includes health screening information containing detailed lifestyle questionnaires, laboratory results, and anthropometric measurements, which are not included in other claims databases. Taiwan has a similar healthcare insurance system as Korea, and the National Health Research Institute collects registration and claims data of the entire population in Taiwan. Various scientific researchers have utilized these reliable data sources and published many relevant papers in cardiovascular science.9)10)11)12)13)14)15)16) However, Taiwan does not implement a health screening program, thus, the claims data do not include lifestyle variables, laboratory results, and anthropometric data. Third, the NHID includes customized cohort datasets, such as NHIS-NSC. Fourth, since the NHID has been linked to other datasets, such as mortality data from Statistics Korea, further detailed information is available for analysis. However, regulations and social consensus are needed to solve this issue. Fifth, the resident registration number would make it more reliable to track for survival. Multiple databases are operated by private insurers in the United States, thus, the mortality data is not reliable. The longitudinal data of this database may be useful for studying long-term outcomes. Sixth, NHIS is also implementing a rare intractable disease (RID) program to offer financial support to patients diagnosed with certain rare and intractable diseases.
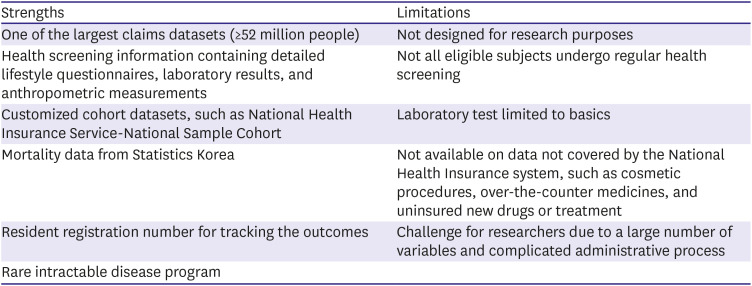
Table 1
Strengths and limitations of Korean National Health Information Database
![]()
The NHID also has several limitations. First, since this dataset was established for recording claims and reimbursements, the dataset may not be optimal for research purposes. There may be a discrepancy between the real disease and the diagnosis claimed by the healthcare providers. Over- or under-diagnosis may pose another limitation. Therefore, validating appropriate operational definitions may be needed before performing the main analysis. Second, since not all eligible subjects undergo regular health screening, the NHID may include data based on only parts of the population. Third, the NHID contains basic laboratory test results, thus, excluding more detailed test results, such as time in therapeutic range in warfarin users, and cardiac enzyme in myocardial infarction patients. Therefore, the NHID may need to include data from other datasets or hospital records. Fourth, the NHID does not include information about healthcare services not covered by the NHI system, such as cosmetic procedures, over-the-counter medicines, and uninsured new drugs or treatment. Fifth, although data are publicly available, the complex data structure containing a large number of variables and complicated administrative process pose a challenge for researchers. Research would require access to the database, a proper statistical approach, and an understanding of operational definitions.
The NHID may be accessed via the Health Insurance Data Service home page (http://nhiss.nhis.or.kr). However, the researchers have to submit a study proposal for acquiring approval from each institutional review board, which is also reviewed by the NHIS review committee. Access to the database is allowed only in designated areas, and remote access is available only for NHIS-NSC. The raw data cannot be retrieved from the NHID server, and only analyzed results can be accessed after acquiring approval. The detailed data of the NHID and substructure are summarized elsewhere.2)3)5)7)8)
CARDIOVASCULAR RESEARCHERS USING THE NATIONAL HEALTH INFORMATION DATABASE AND HEALTH INSURANCE REVIEW AGENCY DATA
NHID and HIRA data may be used in various research areas. Epidemiological studies, describing the prevalence and incidence of disease, temporal trends, or geographical distribution of disease, would be the first steps to reporting basic statistical reports of Korea. These statistics would be important to compare the disease status with other countries. The burden of disease for future generations may be inferred by the current disease status. Atrial fibrillation (AF) is one of the common research topics using NHID and HIRA data. We have summarized recent papers regarding researches on AF (Figure 2).
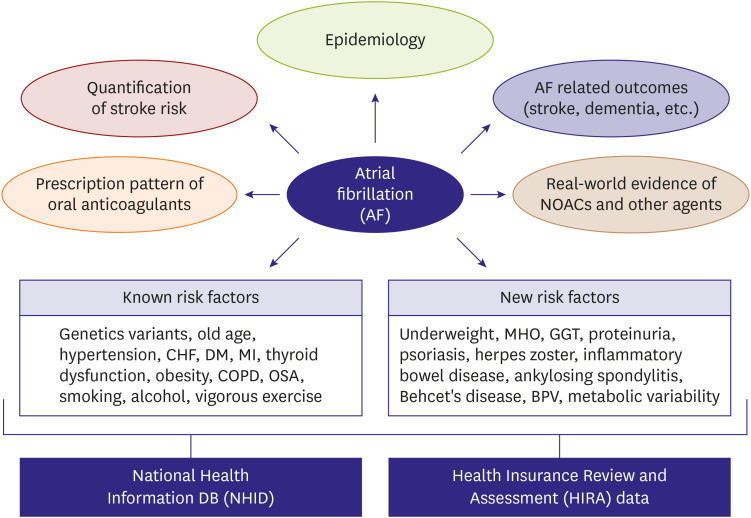
Figure 2
Researches on atrial fibrillation using National Health Information database and Health Insurance Review and Assessment.
BPV = blood pressure variability; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus; GGT = gamma-glutamyl transferase; MHO = metabolically healthy obese; MI = myocardial infarction; NOAC = non-vitamin K antagonist oral anticoagulant; OSA = obstructive sleep apnea.
![]()
Epidemiology of atrial fibrillation
AF is the most common cardiac arrhythmia, and the burden of AF has increased gradually, which now poses a major public healthcare burden.17)18) The temporal trends in the incidence and prevalence of AF in the entire adult population in Korea from 2008 to 2015 have been reported using the NHID.19) The incidence and prevalence of AF have increased gradually in this period. Moreover, the number of patients with a CHA2DS2-VASc score of more than 2 points increased dramatically due to an increase in the elderly population and the prevalence of comorbidities, such as heart failure and diabetes. Kim et al.20) reported that hospitalization for AF, especially due to major bleeding, has increased over the last ten years in Korea. Therefore, AF has resulted in an increment in hospitalization costs due to AF-related complications. AF increased the risk of stroke, hospitalization, and the risk of mortality after adjusting cardiovascular comorbidities.9)21) The risk of all-cause mortality in Korean patients with AF was 3.7-fold higher than that of the general population.22) The most common cause of death was cardiovascular disease (38.5%), and cerebral infarction was the leading specific cause, which also supports evidence suggesting the need to pay more attention to stroke prevention.
Prescription pattern of oral anticoagulants in patients with atrial fibrillation
The prescription pattern of certain drugs has been analyzed using the NHID. Past findings include temporal trends of antithrombotic therapy for stroke prevention in Korean patients with non-valvular AF.23) Asians with AF are usually less likely to receive anticoagulation therapy compared to the Western population. The global registry on long-term oral antithrombotic treatment in patients with atrial fibrillation (GLORIA-AF) registry reports that only 55% of the Asian population with AF were prescribed oral anticoagulants (OAC), whereas 90% of the European population with AF received OAC, and the most common OAC was non-vitamin K antagonist oral anticoagulants (NOACs).24) In line with GLORIA-AF registry, a 50.6% OAC prescription rate was reported in Korean patients with non-valvular AF, and CHA2DS2-VASc score ≥2 in 2015.23) OAC underuse was predominant in female patients, and patients with presence of vascular disease and prior intracranial hemorrhage (ICH). The geographical location and income levels were also associated with AF prevalence and OAC prescription rates.25) Yu et al.26) reported the implications of NOAC introduction on the OAC prescription pattern in patients with AF after full reimbursement of NOAC in July 2015. The difference in penetration of NOAC was influenced by the different medical systems in tertiary referral hospitals, nursing, and public health centers, which resulted in social inequalities of stroke prevention despite full reimbursement. Lee et al.27) reported the changes in patients' characteristics treated with warfarin or NOAC, and whether OAC prescription patterns affected the clinical outcomes. Between 2015 and 2017, NOAC prescriptions increased significantly from 59% to 89%, whereas warfarin use decreased from 41% to 11%. Patients with warfarin changed to younger and with lower CHA2DS2-VASc score, which resulted in improved clinical outcomes. However, patients with NOAC showed consistent lower risks of the composite outcome compared with warfarin despite these changes. These primary results based on the NHID provide insights into improving outcomes by increasing the rate of OAC use for stroke prevention according to guideline recommendations and may also guide planning and decision making regarding health policies.
Optimal anticoagulation therapy in patients with AF who have undergone percutaneous coronary intervention (PCI) is gaining attention. Recent RCTs have highlighted the benefit of double antithrombotic therapy based on NOACs over triple antithrombotic therapy based on warfarin.28)29)30)31) In real-world clinical practice, OAC is under prescribed in patients with AF undergoing PCI due to the fear of bleeding. A recent report examining the prescription pattern of antithrombotic therapy in patients with AF undergoing PCI revealed that the number of patients with AF and PCI has increased constantly, but OAC prescription was only 40% in 2015.32) Furthermore, more than 70% of patients received antiplatelet agents only one-year after PCI.33) Considering that most of these patients have a high risk of stroke, optimal antithrombotic therapy may be necessary after PCI.
Validation of stroke risk calculator
The risk and number of comorbidities may be calculated using formulae, such as the Charlson Comorbidity Index and CHA2DS2-VASc score.34)35) The CHA2DS2-VASc score has been effective in predicting the risk of ischemic stroke in Korean patients with non-valvular AF not receiving OAC.36)37) Therefore, these results highlight the need to introduce OAC in patients with a CHA2DS2-VASc score of more than 2 points, which was adopted in the Korean Guideline of Atrial Fibrillation Management.38)
Real-world evidence of non-vitamin K antagonist oral anticoagulants in Asians with atrial fibrillation
The prescription of NOACs has increased dramatically in Korea. However, only a small number of Asians with AF have been included in pivotal RCTs, thus, evidence based on Asian patients is not sufficient. Asians with AF have a higher risk of stroke and bleeding, especially ICH, compared to non-Asians.39)40) Therefore, evidence regarding the use of NOACs in Asians with AF is needed. Based on the recent increase in the use of NOAC in real-world clinical practice in the Korean population, comparative effectiveness and safety analyses among different OACs using observational cohorts from the administrative claims data may be useful in obtaining a comprehensive dataset studying the use of NOACs in a large-scale Asian population. For treatment comparison using observational cohorts, a number of statistical methods, including multiple regression analysis, propensity score matching, and inverse probability of treatment weighting, were used to minimize the difference among treatment groups. Researchers from Taiwan have published several papers comparing the effectiveness and safety of NOACs and warfarin.10)41) Researchers in Korea have also published several studies comparing the effectiveness and safety of NOACs with warfarin.42)43)44)45)46) Korean researchers have also analyzed special populations, such as patients with low body-weight and liver disease, which were not included in the pivotal RCTs of NOACs.47)48) Since the number of Asian patients with AF was smaller than non-Asian patients, only a small number of underweight patients were included in RCTs.47) Most patients with active liver disease were also excluded from the pivotal NOAC trials.49)50)51)52) However, patients with low-body weight or liver disease may be selected from the health screening database of the NHID. Future research using these variables may produce more novel findings, thus, highlighting one of the strengths of Korean NHID. Another important laboratory variable is serum creatinine. We calculated the creatinine clearance (Cockcroft-Gault Equation) using serum creatinine, body weight, age, and gender. Renal dysfunction is a criterion for dose reduction of NOACs, which aids in the classification of prescription into on-label or off-label dosing. A comparison between on-label rivaroxaban (20 mg daily, R20) and off-label rivaroxaban (15 mg daily, R15) in patients with AF and normal or mildly impaired renal function (CrCl ≥50 mL/min), revealed better outcomes for both R20 and R15 compared to warfarin.44) However, R20 was associated with a slightly lower risk of composite clinical outcome than off-label R15. Another study used creatinine clearance to compare the outcomes between edoxaban and warfarin,53) which revealed that a low dose edoxaban (30 mg daily) showed a higher risk of stroke and systemic embolism compared to warfarin at higher levels of CrCl (>95 mL/min). The FDA label also restricts the use of edoxaban in patients with a CrCl >95 mL/min due to concerns regarding an increased risk of stroke compared to warfarin.54) A recent study, which evaluated the net clinical benefit in the high-risk population, reported that AF patients with a previous history of ICH were excluded from pivotal NOAC trials, thus, there is limited data on optimal anticoagulation therapy among high-risk patients. Among a total of 5,712 patients with AF and prior ICH, NOAC was associated with a significantly lower risk of ICH and stroke compared to warfarin.55) Additionally, NOAC showed consistent benefits compared to warfarin in a population constituting OAC-naïve patients with non-valvular AF and a history of stroke.56)
Health screening information
The national health screening database constitutes lifestyle questionnaires (drinking, smoking, and exercise), laboratory results, and anthropometric measurements data. Heavy drinking of alcohol is a well-known risk factor for AF, but the impact of a high frequency or binge drinking on AF remains unclear. Kim et al.57) reported that frequent drinking and amount of alcohol consumption were significant risk factors for new-onset of AF, whereas heavy consumption per drink was not. The risk of AF could be evaluated using the laboratory parameters. Proteinuria and gamma-glutamyl transferase were found to have predictive values on the risk of AF.58)59)
Variability in the individual laboratory results recorded in the NHID over time may be an interesting topic for research. The health screening database contains serial data of the same patients who undergo biannual health screening examinations. Several variability indices, such as coefficient of variation, standard deviation, variability independent of the mean, and average real variability, could be calculated using serial variables, including body weight, total cholesterol, fasting blood glucose, and serum creatinine.60) High variability of metabolic parameters, such as fasting blood glucose, total cholesterol levels, systolic blood pressure, and body mass index, were independent predictors of mortality and cardiovascular events.60)61) High variabilities of lipid, renal function, blood pressure, and metabolic parameters were associated with the risk of AF, heart failure, myocardial infarction, stroke, and mortality.62)63)64)65)66)67) Mildly abnormal lipid levels were also associated with a higher risk of atherosclerotic cardiovascular disease, whereas lipid variability was not.68)
Rare disease research
Studying a rare disease would be another interesting topic for research using the NHID. The number of patients and the accuracy of diagnosis would be important issues in rare disease research. As prescribed in the previous section, a combination of ICD-10 codes and RID code would increase the accuracy of diagnosis. We have validated the ICD-10 codes with RID code (V127) to define hypertrophic cardiomyopathy (HCM).69) The accuracy, sensitivity, and specificity of the RID code for HCM diagnosis were 92.6%, 91.5%, and 100%, respectively. The prevalence and incidence of HCM in Korea have increased substantially with increasing coexisting modifiable risk factors.70) The risk of AF using the RIF code with special populations, including those with HCM, inflammatory bowel disease, ankylosing spondylitis, and Behcet's disease, has also been reported.69)71)72)73) Considering the population size of the NIHD, research on rare diseases would be feasible, while the NHIS-NSC would not be an appropriate database to study rare diseases.
THE OPERATIONAL DEFINITION OF COVARIATES AND OUTCOMES IN CARDIOVASCULAR RESEARCH
Hypertension
Hypertension is most commonly defined using a combination of three major criteria, including ICD-10 codes I10–I13 or I15 for hypertensive disease usually recorded twice in the outpatient clinic, or once in hospitalization, and a history of prescription of antihypertensive drugs classified as No. 214 in Drug Payment Classification List.74) The detailed information on antihypertensive drugs is summarized in Supplementary Table 1. Research based on the NHIS-National health examinee database reported that systolic blood pressure >140 or diastolic blood pressure >90 mmHg were used as an additional criteria for hypertension.60)75)76) These studies, however, did not include those with hypertensive end-organ damage, such as hypertensive renal (I12) or heart disease (I13), and secondary hypertension (I15). Definitions of the common cardiovascular diseases are summarized in Table 2.
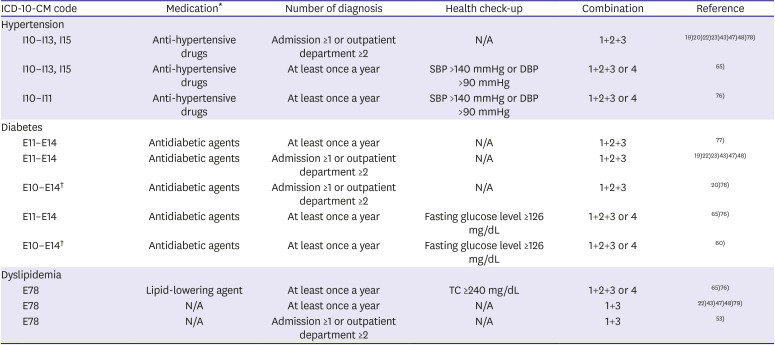
Table 2
Operational definitions of the comorbidities (I)
| ICD-10-CM code | Medication* | Number of diagnosis | Health check-up | Combination | Reference | |
|---|---|---|---|---|---|---|
| Hypertension | ||||||
| I10–I13, I15 | Anti-hypertensive drugs | Admission ≥1 or outpatient department ≥2 | N/A | 1+2+3 | 19)20)22)23)43)47)48)78) | |
| I10–I13, I15 | Anti-hypertensive drugs | At least once a year | SBP >140 mmHg or DBP >90 mmHg | 1+2+3 or 4 | 65) | |
| I10–I11 | Anti-hypertensive drugs | At least once a year | SBP >140 mmHg or DBP >90 mmHg | 1+2+3 or 4 | 76) | |
| Diabetes | ||||||
| E11–E14 | Antidiabetic agents | At least once a year | N/A | 1+2+3 | 77) | |
| E11–E14 | Antidiabetic agents | Admission ≥1 or outpatient department ≥2 | N/A | 1+2+3 | 19)22)23)43)47)48) | |
| E10–E14† | Antidiabetic agents | Admission ≥1 or outpatient department ≥2 | N/A | 1+2+3 | 20)78) | |
| E11–E14 | Antidiabetic agents | At least once a year | Fasting glucose level ≥126 mg/dL | 1+2+3 or 4 | 65)76) | |
| E10–E14† | Antidiabetic agents | At least once a year | Fasting glucose level ≥126 mg/dL | 1+2+3 or 4 | 60) | |
| Dyslipidemia | ||||||
| E78 | Lipid-lowering agent | At least once a year | TC ≥240 mg/dL | 1+2+3 or 4 | 65)76) | |
| E78 | N/A | At least once a year | N/A | 1+3 | 22)43)47)48)79) | |
| E78 | N/A | Admission ≥1 or outpatient department ≥2 | N/A | 1+3 | 53) | |
Combination: 1 = ICD-10-CM code; 2 = Medication; 3 = Number of diagnosis; and 4 = Health check-up.
DBP = diastolic blood pressure; ICD-10 = International Classification of Diseases 10th Revision; N/A = not applicable; SBP = systolic blood pressure; TC = total cholesterol.
*Drug classification codes of medication are summarized in supplementary tables; †E10: type 1 diabetes mellitus.
![]()
Diabetes and dyslipidemia
The Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes Association has summarized the operational definition of diabetes based on the Korean NHID.77) They have also evaluated the proportion of patients with diabetes according to different combinations of diagnosis and prescription data. The Taskforce team concluded the following criteria: 1) ICD-10 codes E11–E14 for diabetes as either principal diagnosis or 1st to 4th additional diagnosis at least once a year; and 2) prescription of antidiabetic agents (Table 2). Moreover, fasting glucose levels ≥126 mg/dL was considered as additional diagnostic criteria for diabetes. The prevalence of diabetes based on this definition was 11.4%. Many studies that did not include data from the Health check-up database used a combination of ICD-10 codes and antidiabetic agents only.78) The detailed information on antidiabetic agents is summarized in Supplementary Table 2.
Myocardial infarction, heart failure, and other comorbidities
Myocardial infarction was diagnosed using ICD-10 codes I21, I22, with more than one diagnosis during admission or at outpatient clinics. Hospitalization with primary diagnostic ICD-10-codes I21, I22 showed a positive predictive value of 92%.80) Heart failure was defined using ICD-10-code I50 with more than one diagnosis during admission or at outpatient clinics. The definitions of peripheral arterial disease, transient ischemic attack, and end-stage renal disease were summarized in Table 3.
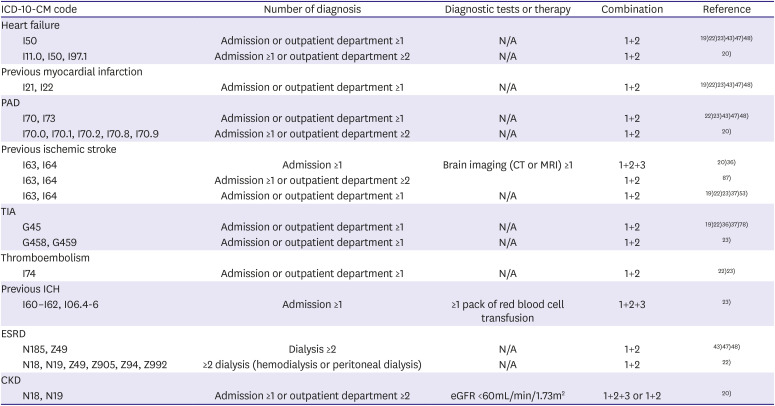
Table 3
Operational definitions of the comorbidities (II)
| ICD-10-CM code | Number of diagnosis | Diagnostic tests or therapy | Combination | Reference | |
|---|---|---|---|---|---|
| Heart failure | |||||
| I50 | Admission or outpatient department ≥1 | N/A | 1+2 | 19)22)23)43)47)48) | |
| I11.0, I50, I97.1 | Admission ≥1 or outpatient department ≥2 | N/A | 1+2 | 20) | |
| Previous myocardial infarction | |||||
| I21, I22 | Admission or outpatient department ≥1 | N/A | 1+2 | 19)22)23)43)47)48) | |
| PAD | |||||
| I70, I73 | Admission or outpatient department ≥1 | N/A | 1+2 | 22)23)43)47)48) | |
| I70.0, I70.1, I70.2, I70.8, I70.9 | Admission ≥1 or outpatient department ≥2 | N/A | 1+2 | 20) | |
| Previous ischemic stroke | |||||
| I63, I64 | Admission ≥1 | Brain imaging (CT or MRI) ≥1 | 1+2+3 | 20)36) | |
| I63, I64 | Admission ≥1 or outpatient department ≥2 | 1+2 | 87) | ||
| I63, I64 | Admission or outpatient department ≥1 | N/A | 1+2 | 19)22)23)37)53) | |
| TIA | |||||
| G45 | Admission or outpatient department ≥1 | N/A | 1+2 | 19)22)36)37)78) | |
| G458, G459 | Admission or outpatient department ≥1 | N/A | 1+2 | 23) | |
| Thromboembolism | |||||
| I74 | Admission or outpatient department ≥1 | N/A | 1+2 | 22)23) | |
| Previous ICH | |||||
| I60–I62, I06.4-6 | Admission ≥1 | ≥1 pack of red blood cell transfusion | 1+2+3 | 23) | |
| ESRD | |||||
| N185, Z49 | Dialysis ≥2 | N/A | 1+2 | 43)47)48) | |
| N18, N19, Z49, Z905, Z94, Z992 | ≥2 dialysis (hemodialysis or peritoneal dialysis) | N/A | 1+2 | 22) | |
| CKD | |||||
| N18, N19 | Admission ≥1 or outpatient department ≥2 | eGFR <60mL/min/1.73m2 | 1+2+3 or 1+2 | 20) | |
Combination: 1 = ICD-10-CM code; 2 = Number of diagnosis; and 3 = Diagnostic tests or therapy.
CKD = chronic kidney disease; CT = computed tomography; eGFR = estimated glomerular filtration rate; ESRD = end-stage renal disease; ICD-10 = International Classification of Diseases 10th Revision; ICH = intracranial hemorrhage; MRI = magnetic resonance imaging; N/A = not applicable; PAD = peripheral arterial disease; TIA = transient ischemic attack.
![]()
Atrial fibrillation
The ICD-10 codes for AF were expressed as ‘I48,’ ‘I48.0–I48.4, I48.9’ or ‘I48, I48.0, I48.1’ in different studies, but these expressions included the same AF patients over different study periods (Table 4).19)20)81)82)83) The KCD was updated in 2011 and 2016, according to the revision of ICD-10-codes. For the accuracy, either one diagnosis during hospitalization or more than twice at outpatient clinics was requited for the diagnosis.81) This criterion was consistent with a Taiwan nationwide population study.84)85) A study validating the accuracy, which included reviewing 628 randomly chosen patients with ICD-10 codes I48 and matching ECG records, revealed a positive predictive value of 94.1% for the definition of AF.83) To confine the analysis on non-valvular AF, patients with a diagnosis of mitral stenosis (I05.0, I05.2, I05.9) or presence of mechanical heart valves (Z95.2–Z95.4) were regarded as valvular AF and were excluded from the final anlysis.19) A washout period of more than one year was set to ensure accuracy of AF incidence.81)82) The prevalence of AF was influenced by the inclusion of a previous history of AF. Yang et al.82) compared different approaches for assessing the prevalence and incidence of AF using the NHID. The formal approach involved examining patients with individual AF diagnosis history and mortality, while the medical use approach involved examining patients who claimed medical expenses annually. The overall prevalence of AF using a formal approach was approximately double that of a medical approach. The formal approach would be more suitable to compare the AF epidemiology among different countries. However, overestimation of patients with AF would pose a limitation for the formal approach. The formal approach may include patients with transient AF, who had not been formally diagnosed and did not visit the hospital for AF for several years. Therefore, the medical use approach would be more suitable to estimate usage of medical services. The prescription pattern of OACs by the medical use approach was 30–50% in Korea, which is consistent with that of Asian AF patients in the GLORIA-AF registry.23)24) Considering the wide variability in the prevalence and incidence of AF in different analysis approaches, careful interpretation, and attention would be needed for comparison with other datasets.
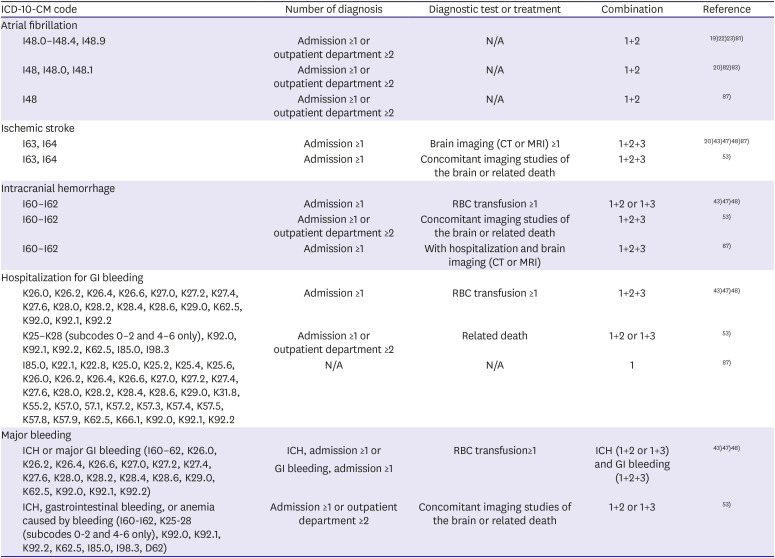
Table 4
Definitions of the outcomes
| ICD-10-CM code | Number of diagnosis | Diagnostic test or treatment | Combination | Reference | |
|---|---|---|---|---|---|
| Atrial fibrillation | |||||
| I48.0–I48.4, I48.9 | Admission ≥1 or outpatient department ≥2 | N/A | 1+2 | 19)22)23)81) | |
| I48, I48.0, I48.1 | Admission ≥1 or outpatient department ≥2 | N/A | 1+2 | 20)82)83) | |
| I48 | Admission ≥1 or outpatient department ≥2 | N/A | 1+2 | 87) | |
| Ischemic stroke | |||||
| I63, I64 | Admission ≥1 | Brain imaging (CT or MRI) ≥1 | 1+2+3 | 20)43)47)48)87) | |
| I63, I64 | Admission ≥1 | Concomitant imaging studies of the brain or related death | 1+2+3 | 53) | |
| Intracranial hemorrhage | |||||
| I60–I62 | Admission ≥1 | RBC transfusion ≥1 | 1+2 or 1+3 | 43)47)48) | |
| I60–I62 | Admission ≥1 or outpatient department ≥2 | Concomitant imaging studies of the brain or related death | 1+2+3 | 53) | |
| I60–I62 | Admission ≥1 | With hospitalization and brain imaging (CT or MRI) | 1+2+3 | 87) | |
| Hospitalization for GI bleeding | |||||
| K26.0, K26.2, K26.4, K26.6, K27.0, K27.2, K27.4, K27.6, K28.0, K28.2, K28.4, K28.6, K29.0, K62.5, K92.0, K92.1, K92.2 | Admission ≥1 | RBC transfusion ≥1 | 1+2+3 | 43)47)48) | |
| K25–K28 (subcodes 0–2 and 4–6 only), K92.0, K92.1, K92.2, K62.5, I85.0, I98.3 | Admission ≥1 or outpatient department ≥2 | Related death | 1+2 or 1+3 | 53) | |
| I85.0, K22.1, K22.8, K25.0, K25.2, K25.4, K25.6, K26.0, K26.2, K26.4, K26.6, K27.0, K27.2, K27.4, K27.6, K28.0, K28.2, K28.4, K28.6, K29.0, K31.8, K55.2, K57.0, 57.1, K57.2, K57.3, K57.4, K57.5, K57.8, K57.9, K62.5, K66.1, K92.0, K92.1, K92.2 | N/A | N/A | 1 | 87) | |
| Major bleeding | |||||
| ICH or major GI bleeding (I60–62, K26.0, K26.2, K26.4, K26.6, K27.0, K27.2, K27.4, K27.6, K28.0, K28.2, K28.4, K28.6, K29.0, K62.5, K92.0, K92.1, K92.2) | ICH, admission ≥1 or GI bleeding, admission ≥1 | RBC transfusion ≥1 | ICH (1+2 or 1+3) and GI bleeding (1+2+3) | 43)47)48) | |
| ICH, gastrointestinal bleeding, or anemia caused by bleeding (I60–I62, K25–28 (subcodes 0–2 and 4–6 only), K92.0, K92.1, K92.2, K62.5, I85.0, I98.3, D62) | Admission ≥1 or outpatient department ≥2 | Concomitant imaging studies of the brain or related death | 1+2 or 1+3 | 53) | |
Combination: 1 = ICD-10-CM code; 2 = Number of diagnosis; and 3 = Diagnostic tests or treatment.
CT = computed tomography; CD-10 = International Classification of Diseases 10th Revision; GI = gastrointestinal; ICH = intracranial hemorrhage; MRI = magnetic resonance imaging; N/A = not applicable; RBC = red blood cell.
![]()
Ischemic stroke
Ischemic stroke was defined by the diagnosis of ICD-10 codes I63 and I64 with hospitalization and concomitant brain imaging studies, involving computed tomography or magnetic resonance image,36)42)43)44)45)46)47)48)86) or related death (Table 4).37)53) This definition has been widely adopted in previous studies using the claims database. The combination of primary diagnostic code of the ICD-10 codes I65 and I64, and brain imaging showed positive predictive value and sensitivity of 92.2% and 91.2%, respectively.80) A study examining patients with a prior history of ischemic stroke revealed that a primary diagnosis at index hospitalization is a prerequisite of the operational definition of ischemic stroke.87)
Intracranial hemorrhage
ICH was defined by the ICD-10 codes I60, I61, and I62 with hospitalization or red blood cell (RBC) transfusion.36)42)43)44)45)46)47)48)86) However, other studies also included hospitalization and concomitant brain imaging studies or related death in the definition of ICH.53)87) Similar to ischemic stroke, when the study population included patients with prior history of ICH, a primary diagnosis at index hospitalization was a prerequisite.87)
Major gastrointestinal bleeding
The operational definition of major gastrointestinal (GI) bleeding varied across research groups (Table 4). Major GI bleeding using the diagnostic codes with hospitalization and RBC transfusion.43)44)45)46)47)48)86) The ICD-10-CM codes for the definition of major GI bleeding varied across working groups. Yu et al.53) defined GI bleeding in accordance with diagnostic codes, including K25-28 (subcodes 0–2 and 4–6 only), K92.0, K92.1, K92.2, K62.5, I85.0, and I98.3, from admission diagnosis or related death. Cho et al.87) reported GI bleeding as per the following codes: I85.0, K22.1, K22.8, K25.0, K25.2, K25.4, K25.6, K26.0, K26.2, K26.4, K26.6, K27.0, K27.2, K27.4, K27.6, K28.0, K28.2, K28.4, K28.6, K29.0, K31.8, K55.2, K57.0, 57.1, K57.2, K57.3, K57.4, K57.5, K57.8, K57.9, K62.5, K66.1, K92.0, K92.1, and K92.2.
Major bleeding
Major bleeding was defined as ICH or major GI bleeding.43)44)45)46)47)48)86) Essentially, the definition of major bleeding includes ICH and major GI bleeding; however, other relevant diagnoses include hospitalization for extracranial or unclassified sites. Cho et al.87) defined major bleeding as fatal bleeding, bleeding necessitating hospitalization, or bleeding that occurred in critical sites, such as intracranial, intraspinal, intraocular, retroperitoneal, or intramuscular with compartment syndrome. Yu et al.53) defined major bleeding as ICH, gastrointestinal bleeding, or anemia caused by bleeding. The diagnostic codes of extracranial or unclassified sites include D62 (acute posthemorrhagic anemia), H05.2 (hemorrhage of orbit), H35.6 (retinal hemorrhage), H43.1 (vitreous hemorrhage), J94.2 (hemothorax), M25.0 (hemarthrosis), and R04 (hemorrhage from respiratory passages including epistaxis and hemoptysis) (Table 4).53)87)
CONCLUSION
The Korean NHID is a nationwide claims database that could be used as a research tool for gathering RWE. The ultimate direction of research using the NHID should aim to improve the welfare of the public, while the findings may help in reducing medical costs and improving public health. Using the results of RWE as a basis for medical practice involves many challenges. Expert advice would be necessary for determining the scientific credibility of the big data analysis until proper technology supplementation is achieved in the future. A step-by-step approach adopted by a team of data scientists, epidemiologists, statisticians, and clinical researchers may be most effective while designing research studies.
 XML Download
XML Download