

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the national statistics of Korea, two leading causes of death in 2018 were cancer and cardiovascular disease.1) There are many evidences that both conditions share common risk factors and each affects the prognosis of the other.2)3) Most cardiologists are aware of that some anti-cancer agents can cause acute and chronic cardiovascular toxic effect.4)5)6)7)8)9)10)11)12)13) There were many efforts to understand the pathophysiology of cardiotoxicity of anti-cancer agents14)15) and to detect early changes of cardiac function during chemotherapeutic periods.16)17) However, the innovation of anti-cancer therapy challenges cardiologists to establish new cardiac function monitoring strategy for novel anti-cancer agents, such as immune check point inhibitors. It is important for cardiologists to be familiar with current strategies for cardiac function monitoring on updated recommendations of not only cardiology,4)5)6) but also oncology societies,18)19)20) to deal with cardiotoxicity of unfamiliar anti-cancer agents. This review tried to suggest the cardiac function monitoring strategies for newly encountered potential cardiotoxic anti-cancer agents and to summarize the cardiovascular complications of novel anti-cancer immunotherapies including immune checkpoint inhibitor (ICI) and chimeric antigen receptor (CAR) T-cell therapy.
Go to : 
CARDIAC FUNCTION MONITORING STRATEGY FOR NEWLY ENCOUNTERED POSSIBLE CARDIOTOXIC ANTI-CANCER AGENTS
Screening before initiation of anti-cancer therapy
For the novel anti-cancer agent that physician does not have enough clinical experiences with to determine the characteristics of cardiovascular complications, it is important to assess risk factors for cardiotoxicity before starting anti-cancer therapy. Common risk factors are listed in Table 1.
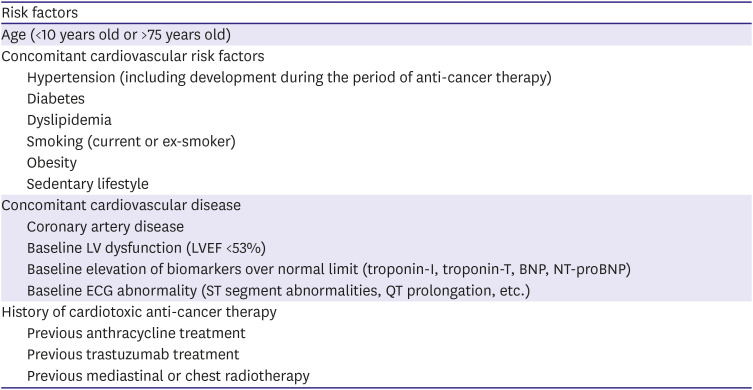
Table 1
Risk factors for development of cardiotoxicity before anti-cancer therapy
BNP = brain natriuretic peptide; ECG = electrocardiogram; LV = left ventricular; LVEF = left ventricular ejection fraction; NT-proBNP = N terminal pro-BNP.
![]()
Patient with high-risk for the development of cardiotoxicity should be consulted to cardiologist before initiating novel anti-cancer therapy and pre-emptive cardiac function monitoring plan should be prepared in advance. Sharing information of novel anti-cancer agents and treatment schedule can help not only cardiologist but also oncologist to manage unexpected cardiotoxic complication of new agents.
Monitoring strategy for cardiovascular complication of novel anti-cancer agent
The biomarkers and electrocardiogram (ECG) are useful tools for the detection of subclinical cardiotoxicity during cancer treatment. Elevation of troponins (troponin-I and -T) and brain natriuretic peptide (BNP)/N-terminal proBNP (NT-proBNP) are very sensitive surrogate marker for detection of early myocardial damage.21)22) Troponin-I (Tn-I) level elevates within 72 hours after anthracycline based chemotherapy and some patients maintain high Tn-I level after 1 months.23)24) NT-proBNP level also rose in breast cancer patients with asymptomatic reduction of left ventricular ejection fraction (LVEF). NT-proBNP was measured every 3 weeks in this study and LVEF was measured baseline and at the end of 4 cycle of doxorubicin based chemotherapy.25) Most recommendations did not suggest timing of biomarker evaluation, but it may need to be measured within 2–3 weeks after each cycle of novel anti-cancer therapy for the early detection of subclinical cardiotoxicity.
Tyrosine kinase inhibitors are well known for QT prolongation5) and concomitant atrial fibrillation in cancer patients is at high risk for thromboembolic events.19) It is important to assess ECG repeatedly to detect changes from baseline ECG and concomitant arrhythmia before and during the treatment. There are no definite recommended intervals for ECG assessment, but cardiologist and oncologist may determine the schedule according to novel anti-cancer agent treatment protocol before initiating therapy.
It is now routine practice that assessment of baseline LVEF before initiating anti-cancer therapy by imaging modalities. European society of cardiology recommended to use echocardiography, nuclear cardiac imaging (multigated radionuclide angiography; MUGA) and cardiac magnetic resonance (CMR) imaging to detect cardiotoxicity.5) Recently oncology society20) recommends echocardiography as a first-line imaging modality because it can provide additional information such as global longitudinal strain. MUGA is no longer recommended for the assessment of LVEF because non-irradiating imaging modality is usually more preferred.20) Because routine use of repetitive CMR imaging is not yet clinically feasible in most centers, echocardiography is the most appropriate modality for cardiac function monitoring during cancer treatment.26) Normal cut-off value of LVEF is 50% in recommendations of some societies18)20) and 53% in other societies.4)5)6)19) Normal cut-off values of LVEF is 53% by echocardiography or 50% by MUGA. Proposed cardiotoxicity monitoring strategy for novel anti-cancer therapy is demonstrated in Figure 1.
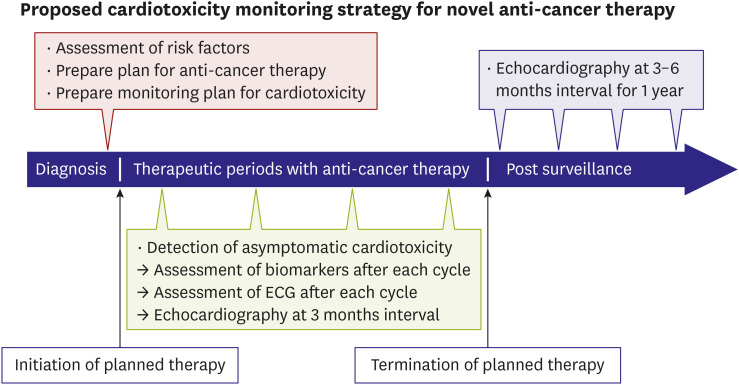
There is no precise recommendation for the surveillance of cardiac function after cancer therapy, especially in new agents which has little information about cardiotoxicity. Echocardiographic evaluation of at 3–6 months interval may be reasonable for cardiac function monitoring after completion of novel anti-cancer therapy despite a few evidence. Post treatment surveillance can be also discussed and planned before initiating cancer treatment between cardiologists and oncologists.
Go to :
CARDIOVASCULAR COMPLICATIONS OF CANCER IMMUNOTHERAPIES
Cancer immunotherapy including ICI and CAR T-cell therapy has dramatically improved outcomes of various cancer patients.27) ICI is a novel anti-cancer therapy that amplifies T cell mediated immune responses against cancer cells. They increase antitumor immunity by blocking intrinsic down regulators of immunity, such as cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death 1 (PD-1) or its ligand, programmed cell death ligand 1 (PD-L1).28) Several ICIs have increased overall survival for patients with various cancers and are approved by the US Food and Drug Administration (FDA) (Table 2).28)
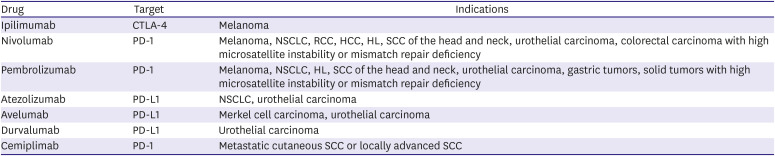
Table 2
US Food and Drug Administration-approved immune check point inhibitors and indications
CTLA-4 = cytotoxic T-lymphocyte antigen 4; HCC = hepatocellular carcinoma; HL = Hodgkin lymphoma; NSCLC = non-small cell lung cancer; PD-1 = programmed cell death 1; PD-L1 = programmed cell death ligand 1; RCC = renal cell carcinoma; SCC = squamous cell carcinoma.
![]()
CAR T-cells are T lymphocytes that have been genetically modified to express T-cell receptors (TCRs) that can recognize tumor-specific antigens. In CAR T-cell immunotherapy, the patient's own T cells are extracted, genetically engineered to target tumor-associated antigens, expanded, and infused back into the patient's body where they continue to multiply, recognize, and destroy cancer cells.29) The US FDA has approved 2 agents that express CD19 on the surface. These agents are currently approved and used for refractory or relapsed acute lymphocytic leukemia and diffuse large B-cell lymphoma. However, preliminary results from several phase I clinical trials of CAR T cells targeting B-cell maturation antigen have shown highly encouraging results in relapsed/refractory multiple myeloma.27)29)
Incidence
In 2016, 2 cases of fatal fulminant myocarditis were reported following combination ICI therapy, both occurring after the first dose of therapy.30) Further interrogation of immunotherapy trial data revealed 18 cases (0.09%) of myocarditis among 20,594 subjects in the pharmacovigilance database.30) The incidence of myocarditis was higher in patients receiving a combination of nivolumab and ipilimumab (0.27%) than in those receiving nivolumab alone (0.06%). Of concern, 50% of ICI-associated myocarditis cases were fatal. A cohort study of patients from a multicenter registry reported a prevalence of 1.14%, which increased to as high as 2.4% for combination therapy with anti-PD-1/anti-CTLA-4.31) ICI associated myocarditis usually occurs early after exposure to an ICI.30)31)32)33) Among 101 cases of ICI associated myocarditis from World Health Organization's VigiBase, 64% occurred after the first or second dose, and 76% occurred within the first 6 weeks of treatment.32) Another report of 35 cases of ICI-associated myocarditis from 8 centers revealed that 81% occurred within the first 4 cycles of ICI therapy (median 34 days from start of therapy).31) Recently, operational definition of cancer therapy associated myocarditis was proposed to facilitate case ascertainment and to report and therefore to enhance the understanding of the incidence, outcomes, and risk factors.34) ICI-associated cardiotoxic effects can extend beyond myocarditis. Heart failure with left ventricular dysfunction but without the evidence of myocarditis on biopsy, pericardial disease and temporal arteritis can also occur.35)36) Arrhythmias and cardiac conduction disease were common cardiotoxic effects including atrial fibrillation (30%), ventricular tachyarrhythmia (27%) and conduction abnormalities (17%).35)
Cytokine release syndrome (CRS) is the most known toxicity of CAR T cells and consists of a constellation of signs and symptoms caused by inflammatory cytokines released by the activated CAR T cells and other immune cells.37) Although CRS is reported to occur frequently (58–93%, Table 3), the toxic effects mediated by the cytokine release are most often mild. However, 20–50% of patients with CRS develop life-threatening complications such as vascular leak syndrome with circulatory collapse and multiorgan failure.27) Symptom onset can occur within minutes to hours or days after infusion begins, coinciding with maximal T-cell expansion. Median time to development of CRS after CAR T-cell infusion is 2.2 days.27) The highest risk is in the first 2 weeks after infusion but theoretically it could occur as long as CAR T cells persist in the circulation, which could be years. In the pivotal randomized clinical trials, myocardial infarction was not observed,38)39)40) cardiac arrest was reported in 4 patients with death occurring in 1 patient, and heart failure in 2 patients following CAR T-cell therapy.29)38)39)40)

Table 3
Incidence of cytokine release syndrome in pivotal randomized clinical trials
| Trial | Type of cancer | Type of CAR T cell | CRS (%) |
|---|---|---|---|
| ZUMA-138) | Relapsed/refractory large B-cell lymphoma | Axicabtagene | 94/101 (93.1) |
| ELIANA39) | Relapsed/refractory B-cell lymphoblastic leukemia | Tisagenlecleucel | 58/75 (77.3) |
| JULIET40) | Relapsed/refractory diffuse large B-cell lymphoma | Tisagenlecleucel | 64/111 (57.7) |
![]()
Mechanisms
Although the exact pathophysiology of ICI associated cardiotoxicity is not well understood, suggested mechanisms include a shared antigen or homologous antigen between the tumor and myocardium or certain TCRs targeting dissimilar antigens.30)41) These are analogous to proposed mechanisms of viral-mediated myocarditis in which the heart is targeted by a process of molecular mimicry.41) As in viral myocarditis, ICI associated myocarditis has been described to have T-cell infiltration of the myocardium.30) Preclinical studies also revealed that CTLA-4, PD-1, and PD-L1 have also important roles in cardiac immune regulation, with abrogation of this pathway resulting in autoimmune myocarditis and cardiac failure.42)43)44)45)46) Fatal autoimmune myocarditis mediated by CD8 T cells was noted in CTLA-4 knockout mice.42) Deletion of PD-1 in mice showed development of spontaneous myocarditis and dilated cardiomyopathy.43)44)
Cytokine release is an expected effect (on-target) caused by immune activation by CAR T cells and is mostly mild, however, some patients develop life-threatening complications caused by systematic circulatory collapse.27) Underlying mechanism of severe cardiac dysfunction during CRS is unclear, but resembles cardiomyopathy associated with sepsis and stress. Among a wide variety of cytokines, interleukin-6 (IL-6) is considered to be a key mediator of the systemic adverse effects.47) Rarely, off-target cross reactivity against titin may also occur, which may lead to cardiogenic shock, and 2 deaths have been attributed to this cause.48)
Diagnosis
Because ICI associated myocarditis is a diagnosis of exclusion, it is important to rule out other more common cardiac conditions including acute coronary syndrome or stress induced cardiomyopathy. The initial guidelines for the management of immune related adverse events separated myocarditis into 4 grades of severity (grade 1–grade 4), with grade 1 being the mildest and grade 4 being the most severe by way of a life-threatening clinical presentation.49) The guidelines recommended that any grade of severity required further workup, which entailed cardiac biomarkers, ECG, chest x-ray, echocardiogram, and consideration of CMR and invasive testing, such as coronary angiography and endomyocardial biopsy (EMB).49) The clinical syndrome associated with myocarditis is broad and can encompass a spectrum of symptoms including palpitations, chest pain and dyspnea. Biomarkers for myocardial necrosis is important for the diagnosis of ICI associated myocarditis. Registry data show that troponin was the most sensitive test, with increased troponin level noted in 94% of patients with myocarditis.31) However, an increased troponin level is not specific for myocarditis, and a normal troponin level, especially in cases that appear late after initiation of ICIs, does not exclude ICI associated myocarditis.27) Troponin level has also been shown to have prognostic value in patients with ICI myocarditis, with a higher troponin level associated with worse outcomes.31) CMR is the gold standard noninvasive test for the diagnosis of myocarditis because of its excellent spatial resolution and additive ability to provide tissue characterization.50)51) Increased capillary permeability associated with myocarditis leads to increased myocardial water content and cellular necrosis, which can be detected by CMR on T1- and T2-weighted images, late gadolinium enhancement and extracellular volume fraction. CMR has sensitivity of 76% and specificity of 96% for diagnosing myocarditis of other causes.52)53) The Lake Louise Criteria, for the CMR diagnosis of myocarditis, have been developed and validated.51) EMB is considered as the gold standard for the diagnosis of myocarditis. Although it is highly specific for diagnosis, the myocardial involvement with ICI-associated myocarditis is usually patchy, which makes EMB less sensitive.27) Recently, operational definition of cancer therapy-associated myocarditis was proposed to categorize the event in terms of the level of certainty (definite, probable, and possible) with which myocarditis can be defined (Table 4).34)
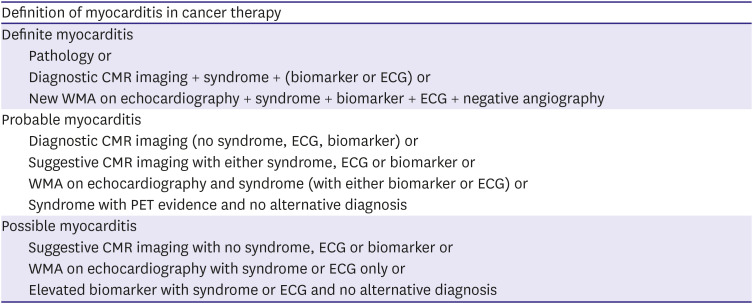
Table 4
Proposed definition of myocarditis in cancer therapy
CMR = cardiac magnetic resonance; ECG = electrocardiography; PET = positron emission tomography; WMA = wall motion abnormality.
![]()
The hallmarks of CRS are fever and tachycardia that may be associated with hypotension and hypoxia. It is a systemic inflammatory response that can affect multiple organs, ranging in severity from mild to severe, with life-threatening conditions including cardiac dysfunction, adult respiratory distress syndrome, neurologic toxicity, coagulopathy, and liver and renal failure.29) However, sepsis, tumor lysis syndrome, pulmonary embolism, primary cardiac event and other systemic illness should be excluded for the diagnosis of CRS. The grading of CRS has varied among different centers using commercially approved and investigational T-cell therapy, making toxicity and management comparisons between studies difficult.29) Recently, multidisciplinary expert group reported a consensus CRS grading scale using fever, hypotension, and hypoxia as principal determinants and grading of severity based on the need for vasopressor support and supplemental oxygen requirement (Table 5).54)

Table 5
American Society for Transplantation and Cellular Therapy cytokine release syndrome consensus grading
Fever is defined as temperature ≥38°C not attributable to any other cause. In patients who have CRS then receive antipyretic or anti-cytokine therapy such as tocilizumab or steroids, fever is no longer required to grade subsequent CRS severity. In this case, CRS grading is driven by hypotension and/or hypoxia. CRS grade is determined by the more severe event: hypotension or hypoxia not attributable to any other cause. For example, a patient with temperature of 39.5°C, hypotension requiring 1 vasopressor, and hypoxia requiring low-flow nasal cannula is classified as grade 3 CRS. Low-flow nasal cannula is defined as oxygen delivered at ≤6 L/min. Low flow also includes blow-by oxygen delivery, sometimes used in pediatrics. High-flow nasal cannula is defined as oxygen delivered at >6 L/min.
BiPAP = bilevel positive airway pressure; CPAP = continuous positive airway pressure; CRS = cytokine release syndrome.
![]()
Management and long-term surveillance
The management of ICI associated myocarditis is largely based on early clinical experience.27) Cessation of ICI therapy and immunosuppression are the cornerstones of treatment. High-dose corticosteroids (methylprednisolone 1,000 mg/day for first 3 day followed by oral prednisone 1 mg/kg) are usually the first line of therapy in the acute phase. Antithymocyte globulin and intravenous immunoglobulin can be considered for unstable patients. Concomitant standard heart failure management should also be initiated, especially if the LVEF is reduced. While the optimal length of treatment with immunosuppressive agents is not clear, it is reasonable to continue until resolution of symptoms and normalization of LVEF, biomarker and conduction abnormality.27) Surveillance for cardiotoxicity in patients receiving ICI can be helpful for prompt recognition and risk stratification, particularly for high-risk patients such as those with preexisting autoimmune disease, diabetes, or cardiovascular comorbidities.27) However, currently, there are no guidelines regarding screening and surveillance of ICI-related cardiotoxicity in asymptomatic patients.
The management of CAR T-cell therapy related CRS is also based on clinical experience without clear guidelines. Supportive care includes inotropes and ventilation supports for hypotension and hypoxia. Patients should be transferred to an intensive care unit if vasopressor or mechanical ventilation is required. Tocilizumab, a monoclonal anti-IL-6 receptor antibody is approved by the FDA as a first-line agent to be used for the management of CRS-related toxicity.55) Tocilizumab 8 mg/kg infused over 1 hour, maximum 800 mg per dose, repeat every 8 hours as needed for patients with grade 2–4 CRS. Some concerns exist that tocilizumab may lessen the efficacy of the CAR T cells as it is unclear to what extent the cytokine-mediated immune response is required for the antitumor response.29)56) Thus, there has been some hesitation toward its utilization in early CRS. There is no universal consensus regarding the timing of tocilizumab initiation (with respect to the severity of CRS) and practices are likely to vary among different institutions.29) Corticosteroids are also effective in the treatment of CRS but are generally considered as second-line therapy.27)
Go to :
CONCLUSION
Many novel anti-cancer therapies including cancer immunotherapies have dramatically improved outcomes of various cancer patients. However, considering the increasing burden of cardiotoxicity of novel anti-cancer therapies, additional effort needs to be directed toward formulating specific evidence-based recommendations for the monitoring of novel anti-cancer therapy and the pre-emptive prevention of cardiotoxicity.
Go to :
 XML Download
XML Download