

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In acute ST-segment elevation myocardial infarction (STEMI), it is vital to reduce the time delay to reperfusion, which is delivered mostly by primary percutaneous coronary intervention (PCI), a preferred strategy over thrombolytic therapy.1)2)3) Initial efforts were focused on the reduction of time delay in the hospital, the door-to-balloon (D-B) time, in part because it can be executed swiftly by mobilizing personnel and facilities within a medical institute. Indeed, D-B time has been substantially improved over the last decades in the developed countries, including Korea.4)5) Observational data demonstrated higher mortality among the patients with longer D-B time than mortality among those with shorter time.6)7) However, the association between D-B time and mortality has been inconsistent across the clinical studies,6)7)8)9) and recent data from a population based registry of United States, Taiwan, Korea has shown that clinical outcomes remained unchanged despite of the significant decline in D-B time during study period.5)10)11)
Effect of reducing D-B time may be limited because D-B time is just one fraction of total ischemic time. Systemic time delay, which is the time from first-medical contact (FMC) to reperfusion, is more relevant target because it constitutes to the total time to reperfusion modifiable by the health care system. In Danish registry,12) systemic time delay was an independent determinant of mortality in patients with STEMI treated with primary PCI. Recognizing the importance of systemic time delay, latest guidelines set the goal of systemic time delay 90 minutes or less in patients with STEMI undergoing primary PCI.13)14) For this goal, collaborative effort with health care delivery system within a community is highly recommended.13)14)
One practical way to reduce systemic time delay is making STEMI diagnosis by on-site electrocardiogram (ECG) transmission via emergency medical system (EMS) in the pre-hospital setting, and immediately activating the catheterization laboratory of intervention center. Pre-hospital ECG transmission and interpretation has been shown to expedite the triage of STEMI patients, reduce the systemic time delay, and improve clinical outcomes.15)16)17) Therefore, performance of ECG at the site of FMC by EMS personnel earned high-level recommendation by contemporary guidelines for the management of STEMI.13)14) Pre-hospital triage network has been set up in various city or rural communities of different countries around world, and its beneficial effect has been demonstrated repeatedly.18)19)20)21)22) However, utilization of pre-hospital ECG is still low, and the potential benefit of the program is not fully materialized in the real world.23) In Korea, pre-hospital ECG transmission has not been adopted in community-based emergency transport system, despite of the fact that pre-hospital time delay was not improved over the years among patients with STEMI.24) To introduce the pre-hospital triage system into the community, a groundwork to identify the feasibility and efficacy of the pre-hospital ECG transmission was a necessary priority. Therefore, Busan Regional Cardiocerebrovascular Center (BRCC) and Busan Metropolitan City Fire and Safety Headquarters (BMFSH) jointly developed a pre-hospital ECG transmission program and conducted the program to set up a regional network for facilitating reperfusion in patients with STEMI.
METHODS
Preparation for pre-hospital ECG transmission program
BRCC at Dong-A University Hospital and BMFSH worked together to establish the infrastructure and software of the program. To conduct the 12-lead ECG examination and transmission, securing additional personnel (up to 3 EMS personnel per one 119 ambulance) and ECG equipment were essential requirement. After several conferences with municipal officers, these requirements were fulfilled by mid-2016 with the funding from Busan Metropolitan City. Additionally, BRCC and BMFSH jointly developed the ECG transmission protocol in ambulance and ECG education course for EMS personnel. Thus, 4 courses of lecture on the cardiovascular disease and 4 courses of intensified ECG lecture (each course consist of 6 hours) were provided to the 119 EMS personnel of Busan-Ulsan metropolitan region. The EMS personnel also received 4 courses of ECG transmission practice training. The education program was rated as satisfactory among 95% of trainees in 2016 survey.
Implementation of pre-hospital electrocardiogram transmission program and participants
Busan Metropolitan City is a second largest city in Korea, with population of 3.5 million and area of 770 km2. In the city, PCI-capable hospitals in 24 hours/7 days basis are mainly concentrated in central part of the city, and such hospitals are sparse or non-existent in the large area of peripheral region (Supplementary Figure 1). Therefore, among the safety stations of Busan Metropolis, those in the peripheral area were first considered for program participation. BRCC and 6 tertiary hospitals capable of primary PCI in 24 hours/7 days basis, together with 22 safety stations belonging to 11 local headquarters of BMFSH participated in this program (Figure 1).
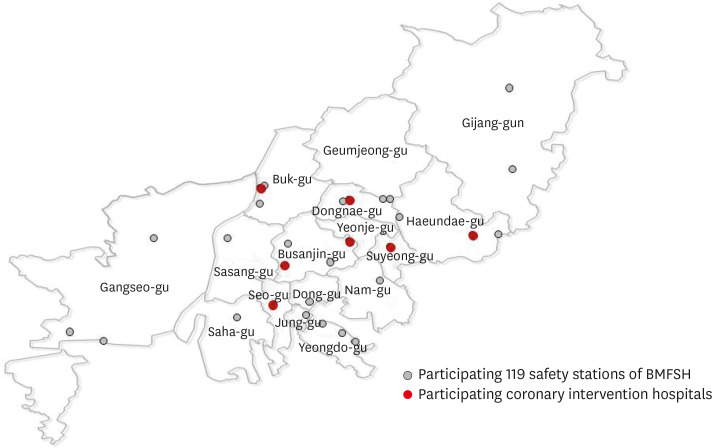
Figure 1
Location of 22 stations of BMFSH and 7 primary PCI-performing hospitals (6 regional hospitals and Busan Regional Cardio-Cerebrovascular Center), participating in the pre-hospital ECG transmission program.
BMFSH = Busan Metropolitan City Fire and Safety Headquarters; ECG = electrocardiogram; PCI = percutaneous coronary intervention.
![]()
Patients living in the area under the jurisdiction of 22 participating BMFSH stations who required medical evacuation of 119 EMS for acute chest pain were eligible for inclusion from August 18, 2016 to January 31, 2017. Patients with 18 years or older who suffered anterior chest pain which is not caused by trauma and severe enough to call 119 EMS were included in the program. No other specific exclusion criteria was applied. ECG recording and transmission was conducted for all those subjects as directed in the protocol.
According to the protocol, the pre-hospital ECG transmission was conducted as follows. On contact with patient with severe precordial chest pain not caused by external injury, trained 119 EMS personnel performed a 12-lead ECG recording at a paper speed of 25 mm/s and amplitude of 10 mm/mV in the ambulance and transmitted acquired ECG images to the on-duty cardiologist in BRCC. To save the time, the ECG print-out of ECG was photographed by 119 EMS personnel and transmitted to mobile phone of the on-duty cardiologist. Transmitted ECG was promptly interpreted by on-duty cardiologist of BRCC. Once diagnosis of ST-segment elevation is made on the basis of the international criteria,25) the on-duty cardiologist directed the 119 EMS personnel to transport the patients to the nearest participating hospital, and alerted the emergency staff of the involved hospital in advance to immediately activate the cardiac catheterization laboratory and prepare for the primary PCI. Thus, primary PCI was performed in the nearest hospital from the FMC site, either Regional Center or other hospital participating in the program, depending on the distance of triage. Patients with ST elevation on the pre-hospital ECG were not sent directly to the cardiac catheterization laboratory, and underwent basic examination including ECG and laboratory test in the emergency room.
Study objectives and definitions
Primary objective of the study was reduction in the time delay to reperfusion in patients with STEMI undergoing primary PCI after implementation of the pre-hospital ECG program. Thus, systemic time delay to reperfusion (FMC to balloon time, FMC-B time) and in-hospital delay (D-B time) were compared between patients with STEMI transferred by EMS with prehospital ECG program and those transferred by EMS in conventional ways. Study group consisted of patients with STEMI treated with primary PCI who were included in the prehospital ECG transmission program. For indirect comparison, control group consisted of STEMI patients who were transported by 119 EMS and underwent primary PCI during previous 12 months (August 2015–July 2016) before the program was implemented. Control group included patients transferred directly to PCI centers by 119 EMS as well as those who were redirected from PCI-incapable hospitals to which initial transport by 119 EMS was made. Inclusion of the latter cases was necessary because it represents the common practice of STEMI patients triage in the Korean communities. Aside from time interval, proportion of patients who had FMC-B time within 90 minutes and D-B time within 60 minutes, as recommended by guidelines,13)14) were also compared between two groups. Secondary objective was efficacy of ECG transmission by 119 EMS, so the time taken for ECG transmission and quality of transmitted ECG image were examined. Time taken for ECG transmission was measured by 119 EMS personnel, and grouped into 3 time groups (transmission within 3, 5, and 7 minutes). Quality of ECG images was rated as high (sharp and clear), moderate (not high but interpretable), and low (difficult to interpret) by the on-duty cardiologist. The study protocol was approved by an institutional review board of the Dong-A University Hospital.
Criteria of ST-segment elevation in 12-lead ECG in the present study was adopted from the Third Universal Definition of Myocardial Infarction as new ST-segment elevation at the J point of at least two contiguous leads of ≥2 mm (≥0.2 mV) in men or ≥1.5 mm (0.15 mV) in women in leads V2 and V3 or ≥1 mm in any other contiguous precordial leads or the limb leads for either gender.25) In order to monitor the interpretation of transmitted ECG, cardiologists in Regional Cardiocerebrovascular Center have met regularly to evaluate ST-segment changes on ECG and to discuss cases. First Medical Contact was defined as described in European guideline, i.e., the time point when the patient is either initially assessed by a physician, paramedic, or nurse or other trained EMS personnel who can obtain and interpret the ECG, and deliver initial interventions.14) Door time was defined as the time of hospital arrival, and balloon time as first coronary balloon inflation time. Final diagnosis of STEMI was registered from the discharge record of participating hospitals.
Statistical analysis
Categorical variables were described as frequencies and percentages and were analyzed with chi-square tests. Continuous variables were presented with mean±standard deviation or median and interquartile range (IQR), and they were compared by Student's t-test or Mann-Whitney U test respectively, depending on the normality test of variables. Analyses were conducted with the use of SPSS version 20.0. A p value of 0.05 or less was considered to indicate statistical significance.
RESULTS
Between August 18, 2016 to January 31, 2017, a total of 289 on-site ECG transmissions were made by 119 EMS personnel. Of these, 42 ECGs were interpreted as ST-segment elevation in the leads. Final diagnosis of STEMI was made in 20 patients who underwent primary PCI. Those patients comprised the study group. Of 22 patients without STEMI, three patients had non-ST-segment elevation acute coronary syndrome and 3 had aortic aneurysm. Three of the 22 patients were diagnosed with variant angina and 7 patients were finally diagnosed with various disease (Table 1). Six patients refused coronary angiography, so the investigators could not determine whether they were actually STEMI or other diseases with resembling STEMI ECG, such as acute myopericarditis or stress induced cardiomyopathy. For control group, 95 STEMI patients who were transported by 119 EMS and underwent primary PCI from August 2015 to July 2016, prior to implementation of prehospital ECG program, were enrolled. When compared with 95 patients in control group, baseline characteristics were similar in 20 patients involved in pre-hospital ECG transmission program (Table 2).
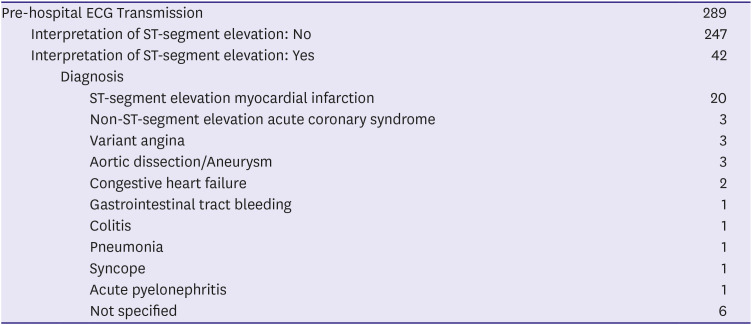

Table 1
Cases of pre-hospital ECG transmission with results of ECG interpretation and clinical diagnosis after triage
![]()
Table 2
Baseline characteristics of study subjects
Data was expressed as means±SD or number (%).
DBP = diastolic blood pressure; SBP = systolic blood pressure; SD = standard deviation.
![]()
The time delay to reperfusion in the study and control groups are shown in Table 3. The details of the distribution of variables and used statistical methods were presented in the Supplementary Table 1 in the supplement. The time delay to reperfusion was reduced with the implementation of pre-hospital ECG transmission program. Figure 2 presents box-whiskers graph of FMC-B and D-B times for the two groups of patients. FMC-B time was significantly reduced in the study group than in the control group (median [IQR], 76.0 [62.2–98.7] versus 90.0 [75.0–112.0], p<0.01) by non-parametric analysis. D-B time was significantly different (median [IQR], 45.0 [34.0–69.5] versus 58.0 [51.0–68.0], p=0.03) between the two groups. The proportion of the patients with FMC-B time shorter than 90 minutes rose after implementation of pre-hospital ECG transmission (75.0% in the study group vs. 51.6% in the control group, p=0.08). The proportion of the patients with D-B time less than 60 minutes also tended to increase (75.0% in the study group versus 61.1% in the control group, p=0.31) (Figure 3). All patients in the study group was transported directly to the PCI-capable hospital without visiting PCI-incapable hospitals en route. In contrast, 11 out of 95 patients (11. 6%) in the control group were transferred to PCI-capable hospitals via PCI-incapable hospitals along the way.
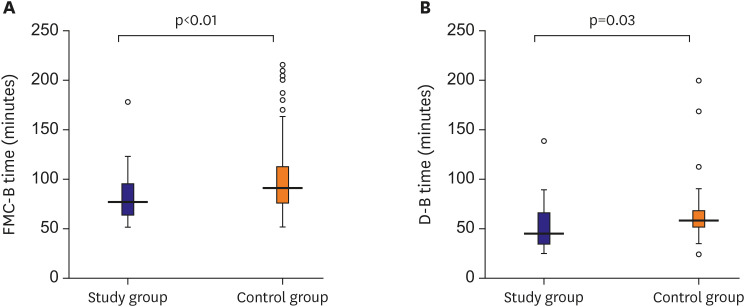
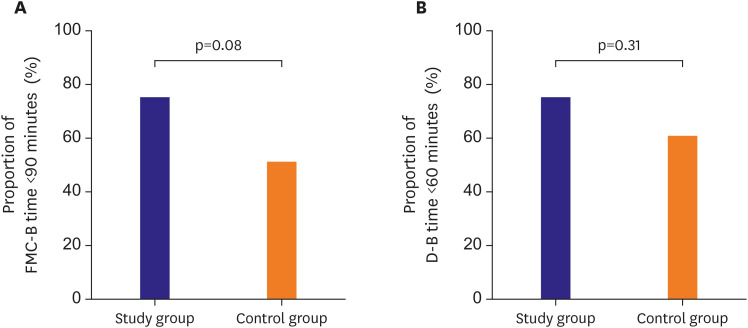

Figure 2
Box plots showing median levels of the time delay to reperfusion of the patients in the study group compared with the control group. (A) shows FMC-B time between the study and control groups, and (B) shows D-B time. Boxes show interquartile ranges.
D-B = door to balloon; FMC-B = first medical contact to balloon.
![]()
Figure 3
Proportion of patients with FMC-B time less than 90 minutes (A), and proportion of patients with D-B time less than 60 minutes (B).
D-B = door to balloon; FMC-B = first medical contact to balloon.
![]()
Table 3
Comparison of the time delay to reperfusion between the study and control groups
D-B = door to balloon; FMC-B = first-medical contact to balloon; FMC-D = first-medical contact to door.
![]()
In the survey to estimate the efficacy of pre-hospital ECG transmission program, ECG examination and transmission was executed by paramedics within 3 minutes in 31.0%, within 5 minutes in 88.1%, and within 7 minutes in 99.2% of the cases. Quality of ECG image was rated as high in 29.5%, moderate in 63.6%, and low in 6.9% of 289 ECGs transmitted.
DISCUSSION
In recent years, pre-hospital delay is increasingly important determinant of total ischemic time in STEMI, because it became clear that shortening of in-hospital delay, D-B time, alone is not enough to further reduce mortality.10) Thus, emphasis has been shifted to minimizing the time delay covering the pre-hospital phase, and time from the FMC to reperfusion, the systemic time delay, is the new target for reducing ischemic time in STEMI guidelines.13)14) On-site diagnosis and triage of STEMI patients by pre-hospital ECG transmission is a practical strategy proven to reduce the systemic delay and patient mortality.15)16)17) However, pre-hospital ECG transmission program has never been adopted in community-based emergency patient transport system in Korea despite the fact that pre-hospital time delay remain unchanged, with median symptom-to-hospital arrival 150 minutes in recent survey.24)
This project was the first attempt in Korea to develop and implement a community-based pre-hospital ECG transmission program by collaborative effort from regional health care center, emergency medical system, and municipal office. After the period of preparations which include securing the personnel, equipment in the emergency vehicle and delivering dedicated educational programs for the EMS personnel, BRCC and BMFSH jointly produced pre-hospital ECG transmission protocol. As a measure of efficacy of the protocol, on-site ECG transmission was completed within 5 minutes by trained EMS personnel in the majority of the cases in this study. New technology of sending ECG directly to a mobile phone of duty cardiologist in this study also allowed prompt review of ECG irrespective of physician's location within or outside the hospital. Quality of ECG image was less satisfactory, resulting in over-interpretation of ST-segment elevation in the study.
After implementing the pre-hospital ECG program in the metropolitan community, we could observe the significant reduction of time to reperfusion in patients who underwent primary PCI. In addition, pre-hospital ECG transmission was also associated with a higher proportion of patients treated within the targeted time windiows of guidelines, FMC-B time less than 90 minutes and D-B time less than 60 minutes. The results of the present study are concordant with previous data of other countries which demonstrated reduced treatment delay in both in-hospital and pre-hospital phases with the triage strategy based on-site diagnosis of STEMI using pre-hospital ECG.15)18)19)20)22)26)27) Every constitute of time delay has been shown to be affected by pre-hospital ECG program, which includes time from symptom to hospital arrival, time from FMC to balloon, and time from symptom to balloon inflation.15)18)19)20)22)26)27) On-site diagnosis of STEMI can reduce pre-hospital time delay by direct transport to the PCI-capable hospital and bypassing the PCI-incapable hospital,15) which was also exhibited in this study. Further, it has been shown that safety of patients was not compromised during direct transport of patient to the intervention center despite skipping the primary care of nearby hospital.26) In addition, the D-B time has been consistently reduced in previous studies,15)18)19)20)21)23)26)27) indicating that pre-hospital notification to the intervention center facilitate the in-hospital process of preparation for primary PCI. By reducing both the pre- and in-hospital time delay, pre-hospital ECG transmission program in the present study and others provide sufficient evidence that it can achieve the goal of minimizing the systemic time delay, a total ischemic time targeted by health care system, in the triage of STEMI patients. The expanded use of pre-hospital ECG should be encouraged to realize the full potential of this program in wider regions of community, and at nationwide level.
There are some limitations to mention in this study. First, the number of the study subjects was too small to conduct full analysis such as influence of diverse practice among different PCI centers. Although we observed a significant reduction in the time to reperfusion with the implementation of pre-hospital ECG program, further study with large numbers of population will be necessary to clarify the impact of the program. The results of this study just show the prehospital ECG transmission can be as feasible and effective in Korean community as demonstrated previously in other countries. Second, there might be systemic bias related to time course. We used the data obtained before the program as control, and the comparative analysis between “before” and “after” could be affected by the changes in other processes that might occur within the study period. However, the control group data was obtained during the 12 months immediately before the study period, and the changes of device, technologies, pharmacotherapy, etc. between two time period could be minimal. Third, the rate of false-positive interpretation of ECG was high in this study, resulting in unnecessary activation of cardiac catheterization laboratory. Of the 42 subjects transferred to PCI facilities based on the of ST-segment elevation on transmitted ECG, only 20 subjects were confirmed as STEMI. This was primarily due to poor image of ECG picture sent to mobile phone of duty cardiologist who chose worse diagnosis in the presence of ambiguous ECG rather than missing STEMI patients. Because of absence of built-in software in ECG equipment for transmitting the ECG directly to mobile phone, the EMS personnel had to take a picture of ECG print-out in the ambulance. This drawback needs improvement, and we are developing an application program which allows transmitting of high-quality ECG image directly to mobile, either Android or iOS system. Another reason for the false-positive interpretation may be the inherent limitations of standard 12-lead ECG to diagnose STEMI accurately. In addition, various conditions may present with ST-segment elevation on surface ECG, mimicking STEMI. Fourth, the nature of the study did not allow the evaluation of clinical outcomes. Because this project was not designed as a clinical trial, only limited access to the patients' data was permitted. Only time intervals, basic demographic data, and initial vital signs were available. Thus, the time interval to reperfusion was the primary objective of this study. Lastly, symptom to FMC time, the patient delay, was not covered in the program. Although this is another important determinant of ischemic time in STEMI, it is the most difficult factor to control, and not modifiable by health care system. Reducing the patient delay would require nationwide effort to enhance public awareness of symptom of STEMI and necessary steps in response to symptoms. At the present time, it is practical to focus on the time constitute amenable to medical transport system, which is the systemic time delay, i.e., time from FMC to reperfusion. Reducing the prehospital phase of the systemic delay is the novel target in STEMI triage. Implementation of pre-hospital ECG transmission in larger population of broader area will be necessary to identify the clinical benefit conferred by this program among the patients with STEMI in Korea.
In conclusion, we developed and conducted a pre-hospital ECG transmission program for expeditious triage of patients with STEMI for primary PCI in the metropolitan community. Prompt on-site ECG transmission and diagnosis were feasible in most cases. Statistically significant reductions of systemic time delay and door-to-balloon time were observed with pre-hospital ECG transmission program. Proportion of patients treated within the targeted time window also increased. These encouraging results suggest that use of pre-hospital ECG should be expanded to realize the full potential of this program in wider community regions and at nationwide level.
 XML Download
XML Download