

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular (CV) disease is the universal leading cause of death for virtually all ethnic groups worldwide. However, the risk of CV disease, its prevalence, natural history, and outcomes can differ vastly according to ethnicity.1)2)3) In addition, treatment policies, therapeutic requirements, and the response to therapy including the incidence of adverse drug reactions may differ among regions and races.4)5)6) Furthermore, an increasing body of evidence has suggested that East Asians may have a different risk-benefit profile for antithrombotic therapy (antiplatelet and anticoagulation therapy), namely a lower risk of thrombosis and an increased risk of bleeding.7)8)9) For example, despite having higher on-clopidogrel platelet reactivity during antiplatelet therapy, East Asian patients showed similar or lower rates of ischemic events after percutaneous coronary intervention (PCI).10)11)12)13)14) Similarly, during anticoagulation using warfarin, despite maintenance of similar international normalized ratios (INRs), the rate of intracranial hemorrhage was reported to be higher in East Asians compared with Westerners, and thus the warfarin maintenance target is recommended at a lower range of INR when used in East Asians.15)16)
RACIAL DIFFERENCES IN EPIDEMIOLOGY
There are several studies that report differences in the incidence of thrombotic and bleeding events according to ethnicity. In a study of California residents using comprehensive hospital discharge data, regardless of gender or whether the cause of the venous thromboembolism (VTE) was secondary or idiopathic, Asians/Pacific Islanders showed the lowest adjusted rates of VTE among various ethnic groups. The prevalence of VTE was 70% lower in Asians/Pacific Islanders compared with African Americans. Other studies also showed that East Asians tended to have a lower incidence of VTE than other races, while African Americans tended to have the highest incidence of VTE.17)18) In another analysis of patients prescribed with clopidogrel after PCI, black race was a strong predictor of stent thrombosis (hazard ratio [HR], 2.07; 95% confidence interval [CI], 1.18–3.63; p=0.011)19) In addition, sub-analysis from the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance trial, a trial that enrolled approximately 15,000 patients with atherothrombosis, showed that CV mortality, ischemic heart disease, and stroke were significantly lower in the Asian population than in the other groups.(Asians vs. Blacks vs. Whites vs. Hispanics: 6.2% vs. 8.6% vs. 7.1% vs. 6.8%, respectively)20) Furthermore, other registry-based PCI studies from Korea and Japan have reported lower incidences of stent thrombosis during the first generation drug-eluting stent era (0.2% per year vs. 0.6% per year).10)11)12)
Contrary to thrombotic events, the risk of bleeding seems to be higher in East Asians compared with Westerners.20)21) In a study of US patients with atrial fibrillation (AF), warfarin-associated intracranial hemorrhage was higher in the Asian population than in Western population, despite a similar INR range.15) The A Correlation between on-ClopidogrEL platelet reactivity and BLEEDing events in PCI-treated patients (ACCEL-BLEED) trial, which examined the relationship between platelet reactivity and bleeding episode among patients receiving PCI, reported that East Asians were more likely to bleed than Westerners with the same platelet reactivity.22)
Taken together, these findings demonstrate that ethnicity may play an important role in the incidence of various thrombotic and bleeding events after antithrombotic therapy. Mostly, Africans (or African Americans) seem to have the highest risk of thrombotic events while East Asians seem to have the highest risk of bleeding.
CLINICAL EVIDENCE FOR RACIAL DIFFERENCE
Aspirin
The use of low-dose aspirin for the primary prevention of CV events remains controversial because the increased risk of bleeding may offset the overall benefit.23)24) Considering the overall increased risk of bleeding in East Asians, this controversy may be especially pertinent to the East Asian population. In a meta-analysis of low-dose aspirin for primary prevention, investigators report a more profound increased risk of intracerebral hemorrhage in Asians compared with non-Asians. The relative risk (RR) of intracerebral hemorrhage in the Asian-populations trials was 1.84 (95% CI, 1.04–3.27; 2 trials), whereas in the non-Asian population trials the risk increase was insignificant (RR, 1.14; 95% CI, 0.89–1.46; 8 trials)25) Likewise, gastrointestinal (GI) bleeding, a clinically relevant adverse effect by aspirin,26)27) occurred more often in East Asians. This can be mostly attributed to the higher prevalence of Helicobacter pylori infection and the genetic variation in relation to cytochrome P450 (CYP450) polymorphism.16)28) In this regard, risk of bleeding risk with aspirin can be minimized with a low-dose strategy. Aspirin given at 75 mg daily is estimated to reduce the risk of GI bleeding by 40% compared with 300 mg daily and by 30% with 150 mg daily.29) This may be one of the reasons why a lower dose of aspirin is prescribed in Asian countries than in the United states where the standard dose of aspirin is 325mg.30) Also, in East Asians, owing to the higher risk of H. pylori infection and the subsequent risk for GI bleeding, it is recommended that a GI-protective agent be used in the presence of risk factors such as old age, prior nonsteroidal anti-inflammatory drugs use, concomitant antiplatelet and anticoagulation use, current smoking, and a prior history of bleeding.27)
P2Y12 receptor inhibitors
Clopidogrel
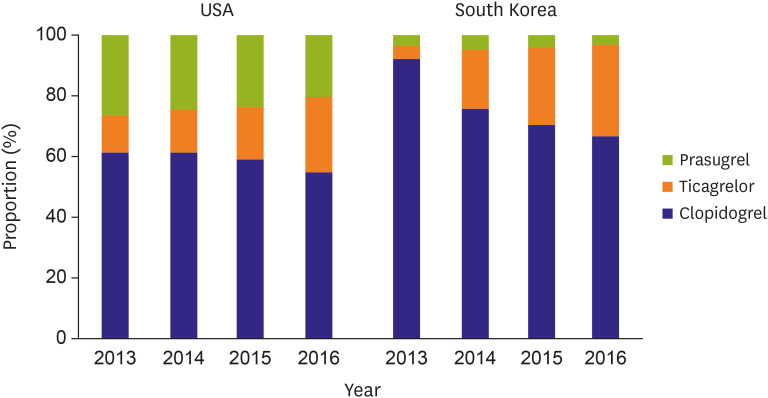
Ethnic differences in response to platelet P2Y12 receptor inhibitors have been reported in multiple papers. In particular, East Asians are known to have a less profound response to clopidogrel compared to Westerners.31)32) After clopidogrel loading (600 mg), the proportion of patients with high on-treatment platelet reactivity was higher in East Asian than Westerners (40.1–63.5% vs. 20–35%)33)34) However, despite a less robust response to clopidogrel, the rates of ischemic events after PCI is similar or even lower in East Asians compared with Westerners. This phenomenon described as the East Asian Paradox.10)11)12)35) This may explain why clopidogrel is still the most frequently used P2Y12 inhibitor in East Asia (Figure 1).36)37) On the other end of the spectrum is bleeding, which has been reported to be higher in East Asians.22)31)32) In the ACCEL-BLEED study, Bleeding Academic Research Consortium (BARC) bleeding occurred within one month of discharge in approximately 30% of the Korean population. Further, the low platelet response (LPR) cutoff was higher in East Asians than that derived from Westerners, suggesting that with the same platelet response to clopidogrel, East Asians are more likely to be in the LPR group, a group that is about 4 times more likely to experience a BARC type 2 or greater bleeding.33)38)39)40)
Third generation P2Y12 receptor inhibitor
Unlike clopidogrel, third generation P2Y12 inhibitors have been shown to have a more profound antiplatelet effect in the East Asian populations.31) As described earlier, the need for clinical trials in the Asian population is the greatest for these new and very potent P2Y12 inhibitors, since as a population, the risk of ischemia is lower and that of bleeding is higher in East Asians. The Dose confIrmation Study assessing anti-Platelet Effects of AZD6140 vs. clopidogRel in non–ST-segment Elevation myocardial infarction-2 (n=609) and PLATelet inhibition and patient Outcomes (PLATO) pharmacokinetics (n=6,381) studies showed a similar degree of platelet inhibition in Asians at a dose which was lower than that in the Western population.41) The bioavailability of ticagrelor in East Asians was found to be approximately 39% higher when compared to Westerners. In patients with ST segment elevation myocardial infarction (STEMI), platelet reactivity decreased very effectively in Asians when taking ticagrelor (180 mg for loading dose [LD], 90 mg twice daily for maintenance dose [MD])42) In particular, about 95% of patients were found to be equivalent to LPR (platelet reactivity unit [PRU] <85), when PRU was measured 48 hours after administration. PLATO trial (n=18,624) where patients were randomized 1:1 to ticagrelor (180 mg LD, 90 mg twice daily MD) of clopidogrel (600 mg LD, 75mg once daily MD), showed a 16% decrease in the risk of CV death, myocardial infarction (MI) or stroke in the ticagrelor arm. The benefit observed with ticagrelor treatment within the first 30 days of treatment continued throughout the treatment period up to 12 months.43) In a retrospective subgroup analysis comparing Asian versus non-Asian patients from that study, there was no interaction between ethnicity and treatment effect. The risk of CV death, MI or stroke and major bleeding was comparable in Asian and non-Asian patients.44) However, in the 2 dedicated randomized trials performed in East Asians, the results were quite different (Figure 2). In the PHase the International study of ticagreLor and clinical Outcomes in Asian acute coronary syndrome patients trial, where 801 East Asian (Japanese, Taiwanese, and South Korean) patients with acute coronary syndrome (ACS) were randomized between ticagrelor and clopidogrel, the overall major bleeding rate was 10.3% in the ticagrelor group and 6.8% in the clopidogrel group. In the TIcagrelor versus Clopidogrel in Asian/KOREAn patients with ACS intended for invasive management trial, where 800 Koreans with ACS were randomly assigned to ticagrelor or clopidogrel, clinically significant bleeding was higher in the ticagrelor group compared with the clopidogrel group (11.7% [45/400] vs. 5.3% [21/400]; HR, 2.26; 95% CI, 1.34–3.79; p=0.002).45) Although this study was underpowered for efficacy outcomes, the composite of death from CV causes, MI, or stroke was numerically higher in the ticagrelor arm (9.2% [36/400] vs. 5.8% [23/400]; HR, 1.62; 95% CI, 0.96–2.74; p=0.07).
Figure 2
Comparison of the primary efficacy endpoint from studies which compared clopidogrel vs. potent P2Y12 inhibitors.
ACS = acute coronary syndrome; CI = confidence interval; HR = hazard ratio; PHILO = PHase the International study of ticagreLor and clinical Outcomes in Asian acute coronary syndrome patients; PRASFIT = PRASugrel compared with clopidogrel For Japanese patIenTs; TICA KOREA = TIcagrelor versus Clopidogrel in Asian/KOREAn patients with acute coronary syndrome intended for invasive management; TRILOGY = TaRgeted platelet Inhibition to cLarify the Optimal strateGy to medicallY manage.
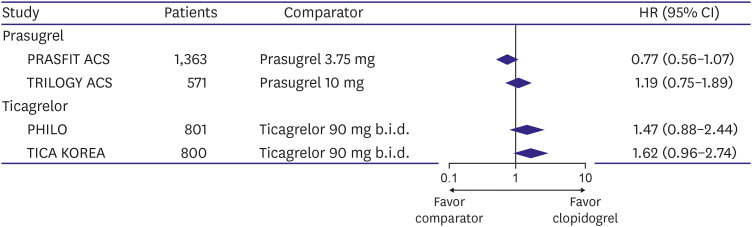
For prasugrel, a pharmacodynamic study in Japan demonstrated that with a decreased LD of 15 mg and a MD of 3.75 mg daily, the antiplatelet effect was achieved significantly faster and stronger than the standard dose of clopidogrel (300 mg LD, 75 mg daily MD).46) The TaRgeted platelet Inhibition to cLarify the Optimal strateGy to medicallY manage-ACS (n=7,243) trial was a study comparing the results of prasugrel 10 mg daily and clopidogrel 75 mg daily with aspirin in non-STEMI patients. In the entire cohort, prasugrel showed excellent propensity (HR, 0.91; 95% CI, 0.79–1.05) in CV death, MI, or stroke, but the opposite result was shown in Asians (HR, 1.19; 95% CI, 0.75–1.89).43) The PRASugrel compared with clopidogrel For Japanese patIenTs with ACS undergoing PCI (n=1,363) trial compared the efficacy of clopidogrel and prasugrel after PCI in the Japanese ACS population. Prasugrel was administered at a dose that was much lower (20 mg LD, 3.75 mg daily MD) than which was studied in the pivotal TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet inhibitioN with prasugrel–Thrombolysis In Myocardial Infarction-38 trial, based on the results of the phase II pharmacodynamic study.47)48) At 24 weeks, ischemic events were numerically lower in the prasugrel compared with the clopidogrel group although the difference did not reach statistical significance due to the small sample size (9.4% vs. 11.8%; HR, 0.77; 95% CI, 0.56–1.07; p=0.12).
Table 1 shows the recommended doses of various P2Y12 inhibitors in the US, Europe, Japan. As described earlier, despite less activation of clopidogrel, the recommended dose in Japan is the same as in the US or Europe, while the dose for prasugrel and ticagrelor is lower in Japan than that recommended in Europe or the US (Table 1).4)5)6)49) Taken together, despite the positive results in pivotal trials performed in mostly Westerners, it remains to be seen whether the newer and more potent antiplatelet agents have a definite benefit in treating ACS patients in East Asia.
Table 1
Recommended dose of P2Y12 receptor inhibitors of Korean, Japanese, American, and European guidelines for acute coronary syndrome

Anticoagulant
Warfarin
Warfarin is known to effectively reduce thromboembolism in cardiac arrhythmia such as AF.50)51) In one meta-analysis of 6 clinical trials, warfarin reduced the risk of stroke by up to 64%.52) In contrast to European and American guidelines for AF, where the recommend target INR is 2.0 to 3.0 for warfarin,53)54) the recommended target may be slightly different according to ethnicity.55) In fact in the Global Anticoagulant Registry in the FIELD–Atrial Fibrillation registry, which included 3,621 East Asians (21% of 13,541), investigators found that mean INR was lower in Asians compared with Westerners.(2.0 vs. 2.4).56)
The concerns of using warfarin in Asia are complex. First, East Asians have higher bleeding rates when treated with warfarin. The may be due to higher risk of bleeding per se in East Asians, but it may also be due to the fact that there is a higher variability of INR in Asians when using warfarin. In particular the risk of intracranial hemorrhage seems to be higher in East Asians compared with Westerners (1.75% vs. 0.34%; HR, 4.06; CI, 2.48–6.66; p<0.001).15) Secondly, it is more difficult to maintain the time in therapeutic range (TTR) for warfarin in East Asians. Lower levels of TTR in East Asians may be due to diet, body weight, etc. In a recent global AF cohort of 15,400 patients, mean TTRs for East Asian were 36.0%, which were lower than that for North Americans (50.9%) and Western Europeans (62.4%).57) Some investigators have even suggested that a lower range of INR would be more adequate in Asians.58)59) This is supported by the J-RHYTHM registry, where the suggested appropriate INR target in Asians was 1.6 to 2.6, which is lower than in targets in Westerners.60)
Non-vitamin K antagonists
Several studies have shown that non-vitamin K antagonists oral anticoagulant (NOACs) have a significant benefit over warfarin when used for prevention of stroke in patients with AF. NOACs are more effective, safe, and convenient compared with warfarin, and therefore, its usage is rapidly increasing. Four large-scale pivotal randomized trials (Randomized Evaluation of Long-term anticoagulation therapY, Rivaroxaban Once daily oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation, Apixaban for Reduction In STroke and Other ThromboemboLic Events in Atrial Fibrillation, and Effective aNticoaGulation with factor xA next GEneration in Atrial Fibrillation) have been performed with NOACs.61)62)63)64)65) Of the 71,783 patients included in the 4 randomized controlled trials, 7,650 were Asian (mostly East Asian). In a meta-analysis, the efficacy and safety of NOACs at standard dose (dabigatran 150 mg, edoxaban 60 mg, rivaroxaban 20 mg, and apixaban 5 mg) was compared between Asians and Westerners.66) NOACs used at the standard dose significantly reduced stroke/systemic embolic event (SEE) in both Western and Asian subjects. However, the magnitude of effect was more pronounced in Asians. (interaction p=0.045) Stroke/SEE, ischemic stroke, MI, and all-cause mortality were similar between NOACs and warfarin when used at the lower dose in both the Asian and Western populations. Bleeding outcomes were mostly significantly in favor of NOACs regardless of ethnicity. However, for major bleeding, hemorrhagic stroke and GI bleeding, the protective effect was more profound in Asians when using the standard dose of NOACs (interaction p value 0.004, 0.046, 0.041, respectively).67)
One nationwide cohort study in South Korea (n=21,679) demonstrated that reduced dose of NOACs showed similar effectiveness and safety compared with the regular dose in patients with low body weight (50–60 kg; HR, 0.907; 95% CI, 0.775–1.059; p=0.217)68)
The a Study to Compare the Safety of Rivaroxaban versus Acetylsalicylic Acid in Addition to Either Clopidogrel or Ticagrelor Therapy in Participants with ACS-1 trial enrolled patients (n=3,037) with ACS and randomized those patients to either aspirin (100 mg/d) or rivaroxaban (2.5 mg twice daily) on top of a P2Y12 receptor inhibitor (clopidogrel or ticagrelor). Compared with participants from Westerners, those from Asia and Pacific region (about 80% patients from Korean and Japan) had the highest risk of significant bleeding (HR, 3.24; 95% CI, 1.27–8.22; p=0.014) and the numerically lowest risk of ischemic events (HR, 0.44; 95% CI, 0.14–1.37; p=0.156).69)
EXPLANATION FOR RACIAL DIFFERENCES
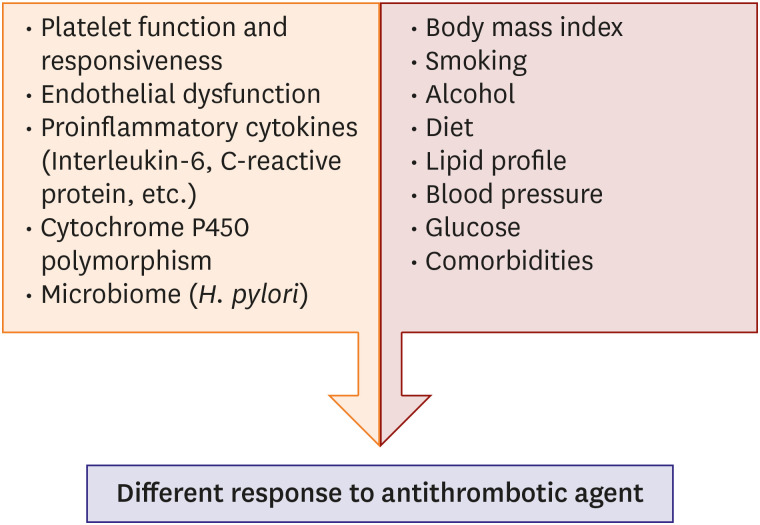
To explain racial difference, we need a more comprehensive understanding of the process of thrombogenesis. The production of blood clots is controlled by very complex interactions, such as blood cell components, plasma components, and blood vessel walls. It is known that there are various differences between races in the process of thrombogenesis (coagulation, fibrinolysis, and inflammation) (Figure 3).18)70)
Differences in platelet function and responsiveness are determined by some genetic factors. Bray et al.71) who previously examined racial differences in patients with coronary artery disease found that epinephrine- and adenosine diphosphonate-induced aggregation and heritability in collagen-induced platelet aggregation was stronger in African Americans compared with Westerners. A cross-sectional study looking at the risk of atherosclerosis in various communities showed that platelet activation markers evaluated by flow cytometry in African Americans were very high.72) Differences are also observed in the coagulation index. Ex vivo experiments showed that African Americans had the highest platelet-fibrin clot.73) There are also genetic factors that affect the activation of antiplatelet agents. It is well-known that clopidogrel activation is very susceptible to levels of the CYP450 enzyme (in particular the CYP2C19 polymorphism).74) There are multiple alleles ('2–'8) of the CYP2C19 which are associated with the loss-of-function and frequency of these alleles differ vastly between different ethnicity. Approximately 30% of Westerners were carriers of the CYP2C19 LoF allele, most of which were '2 allele. On the other hand, about 60% of East Asians were carriers of the LoF alleles, of which about 50% were '2 alleles, and the rest were '3 alleles known to be involved in response to the antiplatelet agent.75) Hispanic races are known to have higher average platelet count than other races, and in this regard to recent study.76)
There are also non-genetic factors that may explain racial differences of thrombogenicity and bleeding tendency. Data from the Multi-Ethnic Study of Atherosclerosis cohort suggests that differences in hemostatic factor and plasma endothelial marker levels seem to coincide with rank ordering of CV risk across racial and ethnic groups. In that study, Western populations showed more thrombogenic and dysfunctional endothelial profiles than did East Asians.77) Likewise, proinflammatory cytokines (e.g., interleukin-6, fibrinogen, and C-reactive protein [CRP]), which are known to be associated with the pro-atherosclerotic phenotype, are be higher in Westerners than in East Asians.78) For example, a Canadian comparison of CRP concentration among 1,250 adults of South Asian, East Asian, Western, and Aboriginal descent revealed significant racial/ethnic differences.79) Mean(±standard error) age- and sex-adjusted CRP concentrations were 1.18±0.13 mg/L in East Asians, 2.06±0.12 mg/L in Westerners. Collectively, the unique genetic and demographic characteristics of East Asians may result in a unique balancing point between ischemia and bleeding, where bleeding risk plays a bigger role in determining both the duration and intensity of antithrombotic therapy.80)
CONCLUSION
Many studies have shown that there are differences in thrombogenicity and bleeding propensity among races. In particular, East Asians seem to have a lower risk of atherothrombotic events and a higher risk of bleeding events compared with the Western population.2)3) Therefore, a ‘one-size-fits-all’ strategy using regimens and doses tested and confirmed in mostly Western populations may not be the optimal treatment strategy for other ethnic groups including East Asians. However, East Asians account for small proportion of most large clinical trials, which consist mainly of Westerners (Table 2). Thus, before mechanically applying the current Western-oriented US and European guidelines, we need studies focused on our region and population characteristics. Furthermore, now in the era of precision and personalized medicine, it may be necessary to pursue efforts to apply genetic data and individualized risk profiles in determining the ideal antithrombotic strategy.
Table 2
Proportion of East Asian populations in large randomized clinical trials of acute coronary syndrome and AF
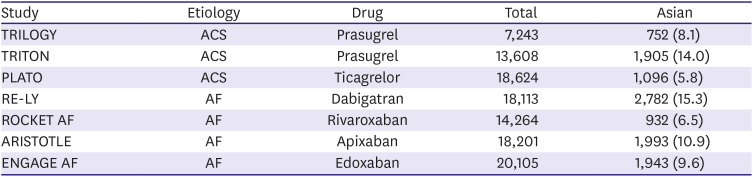
Values are presented as number (%).
ACS = acute coronary syndrome; AF = atrial fibrillation; ARISTOTLE = Apixaban for Reduction In STroke and Other ThromboemboLic Events in Atrial Fibrillation; ENGAGE = Effective aNticoaGulation with factor xA next GEneration in Atrial Fibrillation; PLATO = PLATelet inhibition and patient Outcomes; RE-LY = Randomized Evaluation of Long-term anticoagulation therapY; ROCKET AF = Rivaroxaban Once daily oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation; TRILOGY = TaRgeted platelet Inhibition to cLarify the Optimal strateGy to medicallY manage; TRITON = TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet inhibitioN with prasugrel.
 XML Download
XML Download