

 PDF
PDF Citation
Citation Print
Print



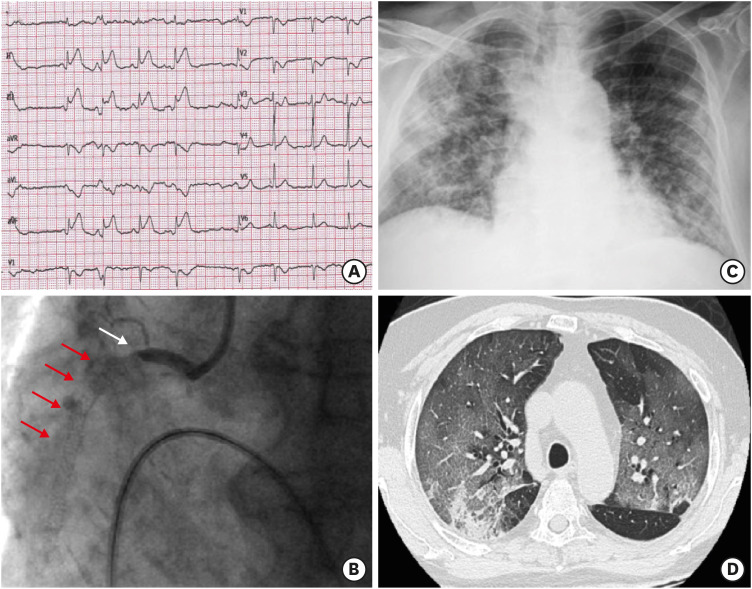
A 79-year-old man presented at our hospital with acute myocardial infarction after he had been successfully treated with percutaneous coronary intervention 2 years earlier, and discharged on dual antiplatelet therapy (clopidogrel 75 mg/day for 12 months and aspirin 100 mg/day indefinitely). The patient had remained asymptomatic after the procedure but had started complaining of fever and cough the week before hospitalization. An intense chest pain was present at admission while the electrocardiogram showed a significant ST-elevation in the inferior leads (Figure 1A). Coronary angiography documented an occlusive in-stent thrombotic lesion of the proximal right coronary artery, that was immediately treated (Figure 1B). A severe bilateral pneumonia was documented at chest X-ray and confirmed at computed tomography (Figure 1C and D). Nasopharyngeal swab tested positive for coronavirus disease 2019 (COVID-19) infection. Arterial blood gas analysis on oxygen therapy showed severe hypoxemia with a PaO2/FiO2 ratio of 100. The patient was treated with noninvasive ventilation but died a few hours later of severe acute respiratory distress syndrome.
Patients with chronic coronary artery disease have an increased probability of developing an acute coronary syndrome (ACS) during acute infections.1) COVID-19 may affect the cardiovascular system in multiple ways and these mechanisms can interact each other: direct myocardial involvement mediated via angiotensin-converting enzyme 22); hypoxemia due to severe COVID-19 infection3); cytokines storm and high concentrations of inflammatory mediators that could lead to atherosclerotic plaque instability and rupture4); repeated floods of catecholamines due to anxiety.5)
This case of diffuse COVID-19 pneumonia seems to confirm the role of severe infection as a precipitating factor for ACS in patients with chronic coronary artery disease, and causal relationship.
 XML Download
XML Download