

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Beta blockers have been the standard treatment for patients with acute myocardial infarction (AMI). Beta blockers have the beneficial effects which reduced ischemia, blood pressure, fatal arrhythmia, and thrombosis.1)234) Guidelines had been established mostly based on randomized trials before reperfusion era. In the era of percutaneous coronary intervention (PCI), there was no prospective randomized trial to show the efficacy of beta blocker therapy on clinical outcomes in AMI patients. In addition, several observational studies have showed inconsistent results.5)6) With evidences of accumulating recent evidences, practical guidelines differ in terms of recommendations regarding indication and duration of beta blockers. In addition, continuous use of beta blocker is often impossible due to adverse drug effect. There was remained unsolved issue whether beta blocker use beyond 1 year after AMI improved outcomes in the reperfusion era. Therefore, we investigated the association of beta blocker therapy with clinical outcomes in patients with AMI who underwent PCI, using a nationwide cohort study using an insurance claims database.
METHODS
Study population
This study is designed as a retrospective cohort using claim data of Korean National Health Insurance Service (KNHIS). The KNHIS as the single insurer of Korean National Health Insurance Program (KNHIP) is currently operating a medical claim database including not only diagnosis, prescription and procedure but also personal data such as age, gender, residential area or the date of death. All of medical service providers and population in Korea have an obligation to join the KNHIP according to national acts. Therefore, the KNHIS database covers almost all of medical behaviors performed in the whole Korean population since 2002. The database is based on Korean Standard Classification of Disease (KCD) 7 code system which is very similar with the International Statistical Classification of Diseases and Related Health Problems (ICD) 10 code system. From 2005 to 2014, we included the lifetime-first users of coronary bare metal or drug eluting stent with diagnostic code of AMI (I21, I22 I23) using the KNHIS database. The exclusion criteria are as follows. 1) no coronary stent implantation, 2) cardiopulmonary resuscitation, 3) all death within 3 months, 4) chronic obstructive pulmonary disease, 5) previous diagnosis of metastatic cancer. In addition, we excluded the patients who never had any anti-platelet agents during follow-up in order to minimize the confounding factor related with the loss of follow-up. The study population was followed for 2 years or until primary end points after stent implantation.
Measurement of variables
The measurement of variables was performed analyzing diagnostic, prescription and procedural code in claim data. We used medical possession rate (MPR) which is calculated as dividing prescription duration by follow-up duration in order to identify long-term use pattern of beta blocker. We classified study population into regular users (MPR ≥80%), irregular users (1–79%), non-users (0%) according to MPR during follow up.7) Baseline characteristics of underlying disease were considered pre-diagnosed if individuals had two consequent diagnoses in out-patient clinic or a single diagnosis during hospitalization. We calculated Charlson comorbidity score which definition was following the Quan's previous study.8) The detailed working definitions of all variables in this study are listed in Supplementary Table 1. The primary end point of this study is the composite of all-cause death, followed myocardial infarction (MI) or all type of stroke. The definition of followed MI is the combination of the main diagnosis of AMI (diagnostic code: I21, I22, I23) confirmed by coronary angiography (procedure code: HA670) during rehospitalization or newly diagnosed sudden cardiac arrest (diagnostic code: I469). We used narrow definition of AMI in order to minimize false-positive detection related with misdiagnosis of previous old MI. All types of stroke include ischemic, hemorrhagic or unknown type of stroke (diagnostic code: I60–64) confirmed with imaging study (examination code: HE101, 201, 135, 235, 236, 451, 461) during hospitalization.
Statistical analysis
The χ2 test or Fisher's exact test were used to compare categorical variables. The student t-test was conducted to compare continuous variables. Univariate and distributional analysis included measures of clinical outcomes. For propensity score matching (PMS), we performed a 1:1 case-control match on the propensity score with a hierarchical sequence until no more matches made. SAS Logistic procedure code was used to create the propensity score. A multivariate Cox proportional-hazards regression model was used to determine the effect of beta blocker as an independent predictor of outcomes. Covariates for the adjustment were selected using multivariate regression analysis. The following variables were included in the Cox proportional-hazard regression model as confounding factors; age, sex, year of study enrollment, hypertension, diabetes mellitus, dyslipidemia, previous stroke, previous MI, heart failure, history of malignancy, stent type, number of stents, in hospital and followed medications (dual antiplatelet, angiotensin II receptor blockers [ARB] or angiotensin converting enzyme [ACE] inhibitor, calcium channel blocker, statin, loop diuretics, and spironolactone). Statistical analysis was performed using the SAS software (SAS institute, ver 9.1, Cary, NC, USA). The statistical significance level was p<0.05.
RESULTS
Prescription rate of beta blocker
We identified a total of 81,752 patients that met eligible criteria for the period between January 2005 and December 2014. Overall, 63,885 (78%) patients were prescribed beta blockers and 17,867 (22%) were not prescribed at discharge (Tables 1 and 2). There was a trend of increase use of beta blockers from 70% in 2005 to 78% in 2014. Among prescribed beta blockers at discharge, the most commonly prescribed medication was carvedilol (52%), followed by bisoprolol (22%). Overall for 2 years, regular users were 53,991 (66%) of patients and non-users were 10,991 (13%). Regular use of beta blockers has been gradually increased from 57% in 2005 to 69% in 2014. During the follow-up, most commonly prescribed agent was carvedilol (45%), followed by bisoprolol (24%).
Table 1
Trends in the use of beta-blockers during hospitalization in patients with AMI underwent coronary stent insertion

Table 2
Prescription pattern of beta-blockers in patients with AMI underwent coronary stent implantation

Baseline characteristics
Overall, mean age was 60 years old and male was 76%. (Table 3) The second-generation drug eluting stent was deployed in 66% and bare metal stent was used in 4.4%. Single stent was implanted in 83% of patients. Prescription rate was 91% of dual antiplatelet therapy, 78% of ARB or ACE inhibitors and 82% of statin at discharge. Compared with no use of beta blockers, regular users were younger, treated more frequently with the second-generation drug eluting stent, had more hypertension and less diabetes mellitus and were prescribed less dual antiplatelet therapy, more ARBs or ACE inhibitors and statin, less spironolactone at discharge. During follow up, regular users were also prescribed more ARBs or ACE inhibitors, but less dual antiplatelet therapy and similar spironolactone.
Table 3
Baseline characteristics according to pattern of beta blocker use

Values are expressed as median (interquartile range), number (%), or mean±standard deviation.
BMS = bare metal stent; CCB = calcium channel blocker; CHF = congestive heart failure; DES = drug-eluting stent; DM = diabetes mellitus; MI = myocardial infarction; RAAS = Renin-angiotensin-aldosterone system.
Clinical outcomes
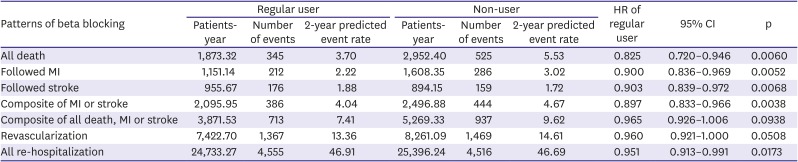
A total of 10,624 patients at each group were matched on the basis of propensity score (Table 4). The baseline characteristics after matching were well balanced. In multivariate regression analysis, age, sex, underlying disease, type of stents, and medications were independent predictors (Table 5). In the matched population, regular beta blocker use was associated with a 29% reduced risk of composite adverse events (all death, MI or stroke) (hazard ratio [HR], 0.717; 95% confidence interval [CI], 0.650–0.791; p<0.001; Table 6). Compared to no use of beta blocker, regular use significantly reduced all death (HR, 0.622; 95% CI, 0.543–0.714; p<0.001) and MI (HR, 0.705; 95% CI, 0.059–0.842; p=0.001), but did not reduce stroke (HR, 1.05; 95% CI, 0.847–1.303; p=0.654).
Table 4
Baseline characteristics before and after propensity score matching
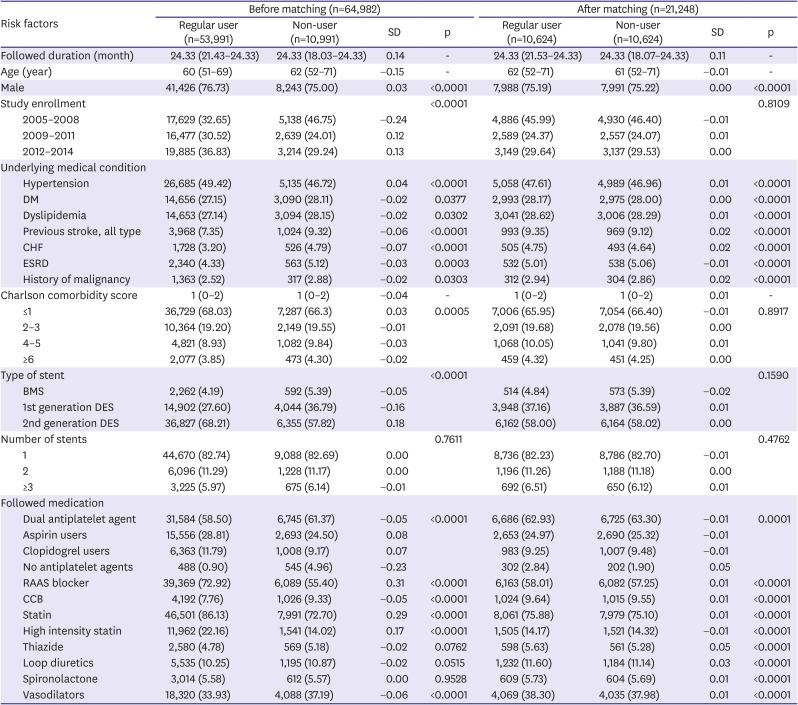
Values are expressed as median (interquartile range) or number (%).
BMS = bare metal stent; CCB = calcium channel blocker; CHF = congestive heart failure; DES = drug-eluting stent; DM = diabetes mellitus; ESRD = end-stage renal disease; RAAS = Renin-angiotensin-aldosterone system; SD = standard deviation.
Table 5
Univariate and multivariate predictors of composite outcomes (all-cause mortality, MI or stroke) after coronary stenting in MI
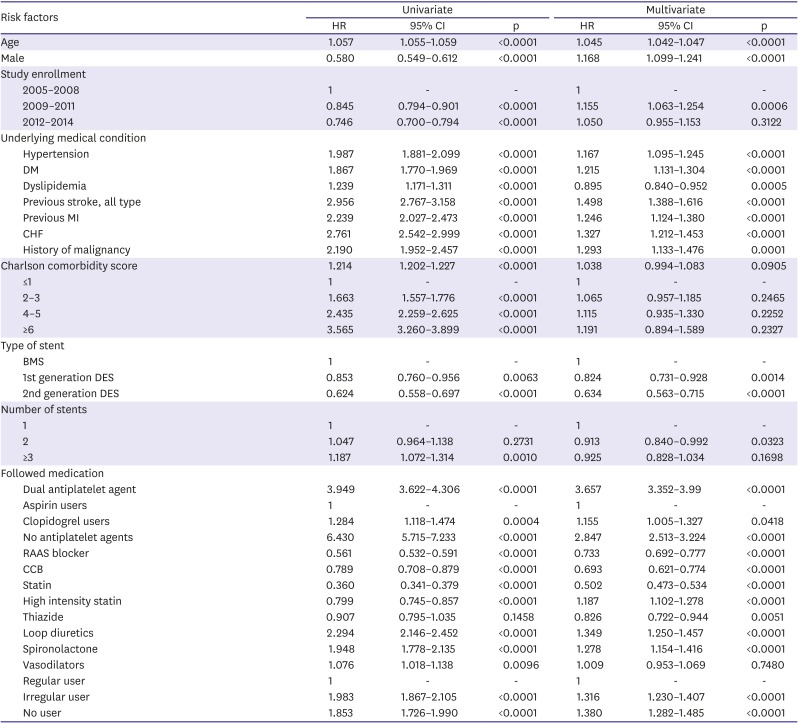
BMS = bare metal stent; CI = confidence interval; CCB = calcium channel blocker; CHF = congestive heart failure; DES = drug-eluting stent; DM = diabetes mellitus; ESRD = end-stage renal disease; HR = hazard ratio; MI = myocardial infarction; RAAS = Renin-angiotensin-aldosterone system; SD = standard deviation.
Table 6
Outcomes after matching
DISCUSSION
The present study was designed to evaluate whether regular beta blocker use might be associated with improved clinical outcome compared with no beta blocker use in patients with AMI treated with PCI. In this nationwide ischemic cohort study, regular beta blocker prescription improved 2 years clinical outcomes.
Beta-blocker have been reported to reduce fatal arrhythmia, ischemia or infarct size and mortality including sudden cardiac death in AMI patients, but most studies had performed in the pre reperfusion era.4)9)10111213) Current guidelines differ in their recommendations for the use of beta blocker after AMI. 2014 American Heart Association (AHA)/American College of Cardiology (ACC) guideline for non-ST elevation acute coronary syndrome suggests that beta blocker therapy is recommended in patients with reduced systolic function as class I, level of evidence C and in patients with normal left ventricular (LV) function as class IIa, level of evidence C.14) 2013 AHA/ACC guideline for ST-elevation myocardial infarction (STEMI) suggests that beta blocker should be continued during and after hospitalization for all patients and with no contraindications.15) Similarly, 2017 European Society of Cardiology (ESC) guideline for STEMI suggests that routine oral beta blocker treatment should be considered during and after hospitalization in all patients without contraindications (Class IIa, level of evidence C).16) 2011 AHA/American College of Cardiology Foundation (ACCF) Secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease recommended beyond 3 years of beta blocker therapy in AMI patients with normal LV function.17) There is no randomized controlled trial to show the efficacy of beta blocker in PCI era. Evidence supporting routine beta blocker therapy following by AMI was lacking in reperfusion era. Beta-blockers did not reduce mortality at 1 year after AMI in patients with heart failure or ventricular dysfunction.5) However, only approximate half of enrolled patients underwent coronary intervention and prescription data was based on point at discharge. A recent meta-analysis which included studies since 2000 showed that beta blocker therapy was not associated to reduce mortality following AMI.18) Conversely, from a registry data, beta blocker at discharge significantly reduced all cause death at 1 year after STEMI in patients treated primary PCI.6) The results from previous studies are inconsistent. Our result of all comer nationwide KNHI database was in line with recommendations from current guidelines for beta blockers therapy in patients with AMI, even after PCI.
Effective duration of beta blocker therapy after AMI has been still unveiled. A single center retrospective study investigated the effect of beta blocker according to the durations of prescription on clinical outcome.19) Beta-blocker therapy after AMI had beneficial effect until 1 years with 29% of mortality reduction, but beta blocker prescription at 1 and 3 years after AMI could not reduce mortality. In addition, 5-year mortality was not significantly decreased in patients who were taking beta blockers at 1 year.20) Most studies had performed based on the information of medication at discharge or small sample size. A few studies tried to provide data of medication at some period point, but not of continued use of the beta blocker. In this study, it is meaningful to compare the patients who were consistently prescribed during follow-up period with patients who never prescribed beta blockers. In contemporary reperfusion era, early revascularization, antiplatelet therapy, ARB or ACE inhibitor, and lipid lowering therapy may likely attenuate the mortality benefit of beta blockers in post AMI. However, this nationwide cohort study showed that beta blocker therapy was associated with mortality reduction at least for 2 years in AMI patients treated with PCI.
A number of limitations must be acknowledged in this study. First of all, there was raised question about the accuracy of the AMI definition using the KCD-10 codes in KNIH claims database. AMI was validated in a previous study with the accuracy of 73%.21) However, we defined AMI as if patients underwent PCI with AMI diagnosis so that the accuracy of diagnosis might be much higher. Diagnosis of AMI was not differentiated into STEMI and non-STEMI due to intrinsic limitation of database. Also, death was defined as the situational status, including hospital death and out of hospital death based on the loss of KNIH qualification. There was a chance of not accurate diagnosis. Uncontrolled covariates may exist. Secondly, this study was not a result of a randomized controlled trial. Consequently, the risk factors not included in the parameters could potentially affect the result. For example, patients who did not receive beta blocker were sicker or at higher risk. Furthermore, we defined regular use as MPR ≥80% but true drug adherence would depend on each patient. There is a possibility to overestimate the effect of beta blocker. Third, we could not adjust several variables, such as LV ejection fraction and time point of primary PCI in patients with STEMI, due to the intrinsic limitation of database. Even though we tried to adjust LV systolic dysfunction using prescription of loop diuretics and spironolactone, the results could be affected by LV function. Despite these limitations, the strength of this study is a large population based all comer dataset to determine the role of beta blocker after PCI in patients with AMI.
In conclusion, use of beta blocker in patients with AMI after PCI was subsequently increased from 2005 to 2014 in Korea. Regular use of beta blocker for 2 years after PCI in AMI patients was associated with improved clinical outcomes compared to no use of beta blocker.
 XML Download
XML Download