

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension is a common chronic disease affecting a large section of the general population. In the US, about 33.2% of the general population is hypertensive.1) There are 244.5 million adults with hypertension in China.2) The prevalence of hypertension in other parts of Asia is also considerable.3) In South Korea, the prevalence is approximately 30% in adults.4) In this review, the progression of hypertension from an elevation in blood pressure (BP) to stage 1 and 2 hypertension is discussed, highlighting the role that plays in this process. This offers an opportunity for prevention of hypertension before it develops.
A 2020 VISION OF HYPERTENSION
The epidemiology of hypertension has been carefully documented in the Hong Kong Cardiovascular Prevalence Study.5)6)7) In this population study of healthy people randomly chosen, the prevalence of hypertension was below 2% in young subjects aged 25–34, but the prevalence increased to around 50% in those 65–75 years of age.8) Premenopausal women have much lower BP than men but the BP rises sharply with age such that after the menopause, the sex difference in BP is no longer apparent. Studies in the US also show this sex difference in the trajectory in BP.9)
As hypertension is often asymptomatic, many people with are unaware of it and even if they have been told that their BP is elevated, many stop taking medications and miss follow-up appointments. This gives rise to the so-called ‘rule of halves’—half of the people with hypertension are unaware of it, and among those diagnosed, only half take treatment and among those treated, only half of them have good BP control.10) There are many reasons for the poor control rate. Not checking the BP in apparently healthy people is one of the most important. Therefore, every adult should have his or her BP periodically checked. If the BP is elevated, then rechecking the BP at intervals should be arranged.
Another reason for the poor control of BP is the ineffectiveness of current antihypertensive medications; most patients require more than one drug class to achieve target.11) This may reflect the multiple pathways involved in BP control. Coupled with the ineffectiveness is the presence of side-effects, which may affect compliance. Measures to improve compliance cited in guidelines include combination pills and once-daily formulations.12) More novel ways of treating hypertension are being explored, such as renal denervation,13) splanchnic denervation,14) ROX coupler,15) vaccine16), and antisense DNA.17) These expensive treatments, not without risks, have the merit of bypassing the need for compliance to take daily medications.
Prevention is better than cure. As BP rises with age, this means that prevention should be started early rather than in old age when hypertension is already common. How early is early? At the last count, there are over 100 genes involved in BP control.18) There are so many genes contributing to hypertension that counselling and prenatal diagnosis are not practised. After all, hypertension is not a life-threatening disease that justifies contraception or abortion. Intrauterine growth retardation increases the risk of the metabolic syndrome and hypertension in later life.19) Better antenatal care and postnatal care of pre-term infants20) may prevent cardiovascular diseases including hypertension.
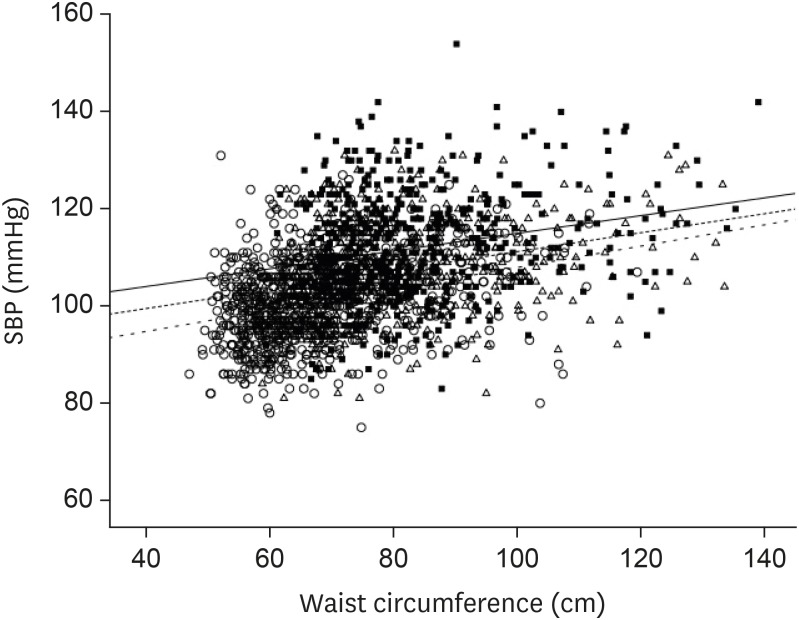
Our own work suggests that childhood obesity is an important determinant of BP in childhood and adolescence.21) In the United States National Health and Nutrition Examination Survey (NHANES), there is a strong relationship between body mass index (or waist circumference) and BP in children (Figure 1).22) Unlike in adults, this relationship is not confounded by antihypertensive medications, smoking and alcohol intake.
Figure 1
Relationship between SBP and body mass index in children in US NHANES 2011–2012. Children aged 8–11, 12–15, and 16–19 years are represented by circles, triangles and squares respectively. The regression lines are shown as solid, dashed and dotted lines respectively.
NHANES = National Health and Nutrition Examination Survey; SBP = systolic blood pressure.
Clearly, here is the window of opportunity for the prevention of hypertension before BP starts to rise. BP control rates are much higher in the young than in the elderly,23) so it should be much easier to achieve BP target in the young. Moreover, a large proportion of young hypertensives may respond to lifestyle measures and not require pharmacological treatment.24)
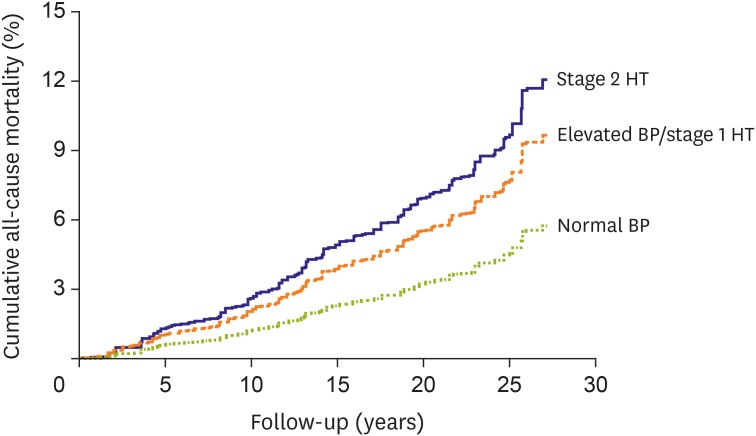
Data from South Korea,25) as well as the USA,26) suggest that prehypertension, or what is now known as stage 1 hypertension, in young adults is already associated with an increase in cardiovascular and mortality risk. We have recently analysed 20-year follow-up data in US NHANES. Compared to young adults with normal BP (<120/80 mmHg), an elevated BP is already associated with increased mortality (Figure 2).27) The current American College of Cardiology/American Heart Association guideline on the prevention, detection, evaluation and management of high BP is therefore timely in defining stage 1 hypertension to include people with a systolic BP of 130–139 mmHg or a diastolic BP of 80–89 mmHg.28) The guideline is based on the findings of Systolic Blood Pressure Intervention Trial.29) We have performed a network meta-analysis on the relationship between outcome and achieved BP in large randomised trials of antihypertensive drugs, and confirmed that an achieved BP of <130/80 mmHg is associated with the best outcome.30)
Figure 2
Kaplan-Meier plot showing the survival curves of US NHANES participants with different levels of BP at baseline. Participants were categorized as normal BP (SBP <120 mmHg and DBP <80 mmHg); elevated BP (SBP 120–129 mmHg and DBP <80 mmHg); stage 1 HT (SBP 130–139 mmHg or DBP 80–89 mmHg); or stage 2 HT (SBP ≥140 mmHg or DBP ≥90 mmHg). Note the curves for elevated BP and stage 1 HT are superimposable and therefore shown as one curve.
BP = blood pressure; DBP = diastolic blood pressure; HT = hypertension; NHANES = National Health and Nutrition Examination Survey; SBP = systolic blood pressure.
In changing the definition of hypertension, the US hypertension guideline makes many people in the general population hypertensive. This may be undesirable in countries that are still struggling to treat stage 2 hypertension, but in countries that have a good health system, it is the next big target to identify people in the community at risk of progression to stage 2 hypertension and cardiovascular events. The characteristics of people with ‘stage 1 hypertension’ are interesting; most of them are male and obese (Table 1).31) Fortunately, as mentioned above, hypertension at this early stage is easy to control and weight loss is less difficult in young people.
Table 1
Characteristics of adult participants with stage I hypertension in NHANES 2015–2016
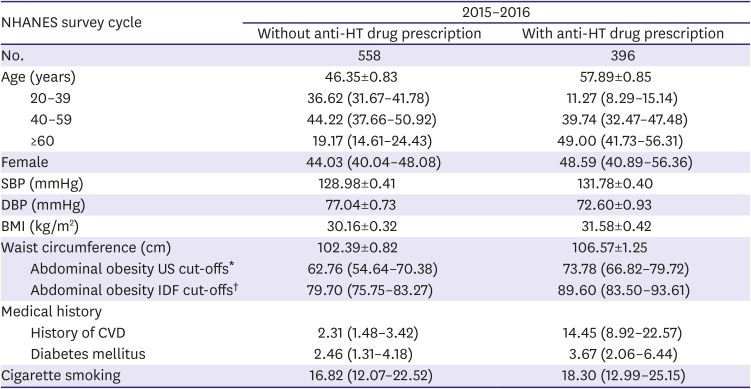
Data are shown as mean±standard error or percentage (95% CI).
BMI = body mass index; CI = confidence interval; CVD = cardiovascular disease; DBP = diastolic blood pressure; HT = hypertension; IDF = International Diabetes Federation; NHANES = National Health and Nutrition Examination Survey; SBP = systolic blood pressure.
*Abdominal obesity is defined as ≥102 cm and ≥88 cm for male and female, respectively; †Abdominal obesity is defined as ≥94 cm and ≥80 cm for male and female, respectively.
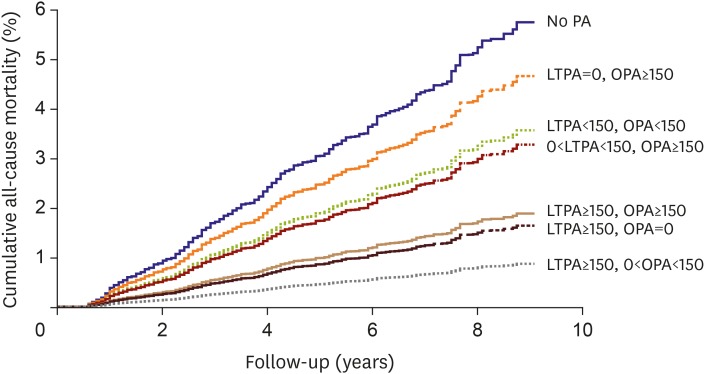
Obesity is a problem that afflicts many parts of the world.32) It is a huge problem in the US, but it is also a problem among the poor in developing countries. In most Asian countries, US-style fast food may not be the main cause of obesity. Instead, changing from a rural to an urban environment with less physical activity (PA), from physically demanding jobs to office jobs, may be an important underlying factor. We compared leisure-time PA (LTPA) with occupational PA recently, and found that while people who had no PA have the highest mortality rate, adequate LTPA was associated with half the risk of death (Figure 3).33)
Figure 3
Kaplan-Meier plot showing the survival curves of each PA group for US NHANES participants aged 18 to 64 years old at baseline. Participants were categorized into groups by their weekly amount of LTPA, OPA, and the tPA. Values for PA are in minutes/week. The groups with LTPA ≥150 minutes/week had higher survival when compared with the group with no PA (all p<0.001).
LTPA = leisure-time physical activity; NHANES = National Health and Nutrition Examination Survey; OPA = occupational physical activity; PA = physical activity; tPA = total physical activity.
In many parts of Asia, rice is part of the staple diet. While it is inherently low in fat, when boiled, it has a high glycaemic index.34) Indeed, the blood glucose profile after eating a bowl of rice is like that of an oral glucose test.35) Before the days of cars, machines and computers, the glucose would be utilised; in modern times, the excess calories are stored as fat.
Hypertension is part of the metabolic syndrome36) and in a large proportion of people with hypertension, obesity is an important underlying cause. Reduction in body weight is the most effective nonpharmacological way of reducing BP (Table 2).28)37) Bariatric surgery can reduce body weight dramatically and the reduction in BP is also equally impressive.38) Less drastic ways of reducing body weight, such as orlistat,39) glucagon-like peptide-1 receptor agonist40) and sodium-glucose cotransporter-2 (SGLT2) inhibitor,41) can also reduce BP. By inhibiting the reabsorption of glucose in the proximal convoluted tubules, SGLT2 inhibitors cause a net loss of up to 300 calories a day. This is weight loss without dieting and without exercise! In addition, there is cardiovascular risk reduction,42) even in non-diabetics. It would not be surprising if this drug class would earn an indication for use in people with hypertension, who are often obese and have other cardiovascular risk factors.
Table 2
Effect of lifestyle modification on SBP
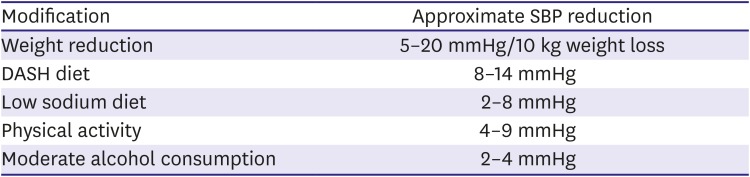
| Modification | Approximate SBP reduction |
|---|---|
| Weight reduction | 5–20 mmHg/10 kg weight loss |
| DASH diet | 8–14 mmHg |
| Low sodium diet | 2–8 mmHg |
| Physical activity | 4–9 mmHg |
| Moderate alcohol consumption | 2–4 mmHg |
Adapted from The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) produced by the National Heart Lung and Blood Institute, US (http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf).37)
DASH = dietary approaches to stop hypertension; SBP = systolic blood pressure.
CONCLUSION
In 2020, detecting and adequately treating hypertension remains an important goal. Cardiovascular risk assessment and promoting a healthy lifestyle in the young are likely to forestall hypertension and future cardiovascular disease. Preventing or reversing hypertension is no longer an impossible dream.
 XML Download
XML Download