

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
This clinical practice position statement, a product of the Fatty Liver Research Group (FLRG) of the Korean Diabetes Association (KDA), proposes recommendations for the diagnosis, progression and/or severity assessment, management, and follow-up of non-alcoholic fatty liver disease (NAFLD) in patients with type 2 diabetes mellitus (T2DM). The literature was retrieved by an extensive PubMed search up to April 2019. After extensive reviews and discussions for the last 3 years by the research group, two sentinel reviews were published in Diabetes and Metabolism Journal in 2019. The draft of the statement was presented and discussed in a session of the FLRG during the 32nd KDA scientific meeting in 2019. Then, the statement was further discussed, edited and updated until the final acceptance of the statement in the journal. Epidemiological evidence suggests a strong bidirectional relationship between type 2 diabetes mellitus (T2DM) and non-alcoholic fatty liver disease (NAFLD), including the development and severity of NAFLD, progression to non-alcoholic steatohepatitis (NASH), and advanced fibrosis, independent of liver enzymes [1]. Furthermore, the coexistence of T2DM and NAFLD results in an unfavorable metabolic profile and an increasing cardiovascular (CV) risk [234]. Although steatosis can be defined by various clinically available diagnostic tools, it can be numerically and strictly defined by assessing liver fat: ≥5% of fat-containing hepatocytes in histology; proton density fat fraction (PDFF) ≥5% on magnetic resonance imaging (MRI), or >5.5% on proton magnetic resonance spectroscopy (1H-MRS) [56]. The definitive diagnosis of NASH requires a liver biopsy.
Among many treatments for NAFLD in patients with T2DM, weight reduction is the only approved option for NAFLD. However, it is not easy to maintain weight loss by only lifestyle modification strategies, so additional pharmacological options should be supported. To date, although many drugs have been investigated, pioglitazone could be the first-line therapy in patients with T2DM and NAFLD. Many drugs are currently being developed and investigated, and combination strategies will be introduced for the treatment of NAFLD and diabetes in the future.
Go to : 
PREVALENCE OF NAFLD IN PATIENTS WITH T2DM
Keynotes
-The prevalence of NAFLD in patients with T2DM is more than two times higher than that in the normal population.
-NAFLD is a risk factor for T2DM.
NAFLD is the most common liver disorder, affecting 20% to 40% of adults; the prevalence rates differ according to the diagnostic method, age, sex, and ethnicity [678]. In patients with T2DM, NAFLD prevalence ranges from 70% to 95%; the rate is extremely high, up to 98%, in patients with morbid obesity [8]. In the general Korean population, NAFLD prevalence ranges from 16.1% to 25.2% (Table 1) [910].
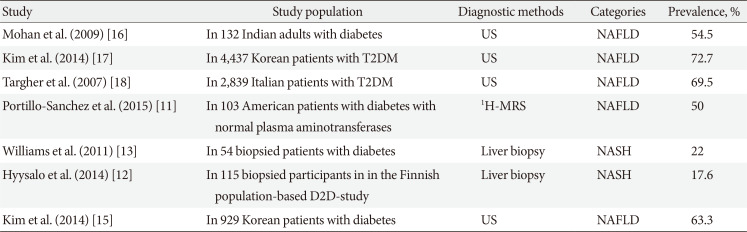
Table 1
The prevalence of NAFLD and NASH in patients with diabetes
| Study | Study population | Diagnostic methods | Categories | Prevalence, % |
|---|---|---|---|---|
| Mohan et al. (2009) [16] | In 132 Indian adults with diabetes | US | NAFLD | 54.5 |
| Kim et al. (2014) [17] | In 4,437 Korean patients with T2DM | US | NAFLD | 72.7 |
| Targher et al. (2007) [18] | In 2,839 Italian patients with T2DM | US | NAFLD | 69.5 |
| Portillo-Sanchez et al. (2015) [11] | In 103 American patients with diabetes with normal plasma aminotransferases | 1H-MRS | NAFLD | 50 |
| Williams et al. (2011) [13] | In 54 biopsied patients with diabetes | Liver biopsy | NASH | 22 |
| Hyysalo et al. (2014) [12] | In 115 biopsied participants in in the Finnish population-based D2D-study | Liver biopsy | NASH | 17.6 |
| Kim et al. (2014) [15] | In 929 Korean patients with diabetes | US | NAFLD | 63.3 |
![]()
Half of patients with T2DM have NAFLD despite having normal alanine aminotransferase (ALT) levels [1112]. Population based studies have reported the prevalence of NASH to be 17.6% to 22%% in individuals with T2DM and 3.7% in nondiabetic individuals [13]. Furthermore, the prevalence of NASH among biopsied patients with diabetes can be as high as 64.0%, whereas the prevalence of advanced fibrosis (≥F3) in patients with T2DM is approximately 10.4% [14]. The NAFLD prevalence in Asians is not lower than that in Caucasians. In a study involving Korean patients with T2DM who were subjected to ultrasonography (US) examination in a university-based diabetes clinic, 63.3% of patients had NAFLD (Table 1) [11121315161718].
Furthermore, the risk of diabetes in subjects with NAFLD has been shown to be 2-fold higher than that in control subjects, even after adjustment for various risk factors [1920]. When obesity, insulin resistance, or hyperglycemia is combined with NAFLD, T2DM risk is dramatically increased [2]. In line with these studies, the resolution of steatosis in patients with NAFLD decreases T2DM risk by 39% to 82% [2122].
Go to :
THE PROGRESSION OF NAFLD AND DIABETES
Keynotes
-Patients with T2DM and NAFLD have an increased risk of NASH and fibrosis.
-Patients with both T2DM and NAFLD have a higher risk of CV diseases and diabetic complications compared to those without NAFLD.
Approximately 10% to 35% of subjects with normal liver histology progress to steatosis, 12% to 44% of those with hepatic steatosis progress to steatohepatitis, and up to 15% of patients with NASH are known to progress to cirrhosis [23]. In patients with NAFLD, the prevalence of NASH is approximately 60% in biopsy-indicated patients and 29.9% in patients without such an indication [8]. Studies have shown that increasing age, diabetes, and hypertension are predictive clinical parameters for fibrosis [2425].
NAFLD and NASH can progress to cirrhosis and liver failure in up to 15% of affected patients [26]. These patients are also at risk of developing hepatocellular carcinoma (HCC). Advanced age, high aspartate aminotransferase (AST) levels, thrombocytopenia (marker of progression of liver fibrosis), and diabetes were identified as risk factors for the development of HCC in Japanese patients with US-diagnosed NAFLD. Patients with NAFLD with advanced stages of fibrosis have a 7-fold higher risk of HCC compared to those without liver disease [27]. However, the cause of cirrhosis remains unclear in 30% of cases, and most of these cases are now considered NAFLD-related [28]. Cryptogenic cirrhosis was reported to be an underlying disease in approximately 7% of HCC cases in Korea and Japan compared with 13% in the United States [2829]. T2DM is also closely associated with progression to NASH, advanced fibrosis and the development of HCC [17].
NAFLD is a consequence but also a precursor of metabolic comorbidities, including diabetes, dyslipidemia, and hypertension, and thus, NAFLD increases CV events, and mortality even in the absence of these comorbidities [30]. Furthermore, hepatic fibrosis is a key predictor of liver-related outcomes and is also associated with all-cause and CV mortality as well as mortality due to cirrhosis, HCC, and infectious diseases in NAFLD patients [3132]. Diabetes is an important factor affecting all-cause and CV mortality in patients with NAFLD [31]. Thus, after the diagnosis of NAFLD, the stage of fibrosis needs to be assessed appropriately [31]. There is evidence that the presence of NAFLD in patients with T2DM is associated with increased risks of macrovascular and diabetic microvascular complications as well as chronic kidney disease [2].
Go to :
DIAGNOSIS OF NAFLD
Keynotes
- NAFLD can be diagnosed by a two-step process: (1) confirmation of he-patic steatosis, either by imaging modalities or histology and (2) exclu-sion of secondary causes of liver steatosis.
Routine screening for NAFLD in patients with T2DM is not currently recommended because of the unclear cost-effectiveness and uncertainties with diagnostic testing and treatments [33]. In individuals with and without diabetes, three important processes should be used to diagnose and assess NAFLD: (1) determine the existence of hepatic steatosis, either by imaging or histology; (2) exclude secondary causes of liver steatosis; and (3) assess NAFLD severity by establishing the presence of moderate-to-severe fibrosis (fibrosis stage of at least F2) [2]. Before making the diagnosis of NAFLD, secondary causes of hepatic fat accumulation and significant alcohol consumption (≥21 drinks/week for men and ≥14 drinks/week for women) need to be excluded [5]. Alcohol consumption over a 2-year time frame needs to be surveyed in detail using validated questionnaires [5]. However, it is noteworthy that there is also a synergy between alcohol intake and obesity or genetic risk factors of NAFLD progression for any given level of alcohol intake [6]. Even in patients whose alcohol consumption level is low, meeting the diagnostic criteria of NAFLD, small amounts of alcohol intake may affect outcomes in NAFLD, which warrants further study [534]. After performing a history and examination, the next investigations are to establish whether the patient has NAFLD or another liver condition.
A consensus regarding initial blood tests for NAFLD has not been reached among guidelines [33]. The decision on the extent of liver blood tests and interpretation of the results should be determined in a clinical context. In adults, initial screening tests may include abdominal US, hepatitis B surface antigen, hepatitis C antibody (with follow-on polymerase chain reaction if positive), anti-mitochondrial antibody, anti-smooth muscle antibody, antinuclear antibody, serum immunoglobulins, and simultaneous serum ferritin and transferrin saturation [33]. Although ALT levels have been shown to be the best single biochemical correlate of hepatic steatosis, liver enzyme levels can be normal, fluctuating, or elevated in patients with NAFLD [23]. There have been suggestions that the current reference intervals for ALT may be too high [3536], and a recent guidance recommending an ALT of >30 U/L as being significant in males and >25 U/L significant for females [37].
Noninvasive imaging studies to assess hepatic steatosis and hepatic fibrosis
Keynotes
- Despite its limited accuracy, US is a useful screening tool to detect hepatic steatosis with other possible structural abnormalities in patients who are suspected of having NAFLD.
- Vibration-controlled transient elastography (VCTE) with controlled at-tenuation parameter (CAP) is a simple quantitative index to detect ste-atosis in clinical practice, but CAP values should be carefully interpreted with patient factors such as obesity.
- As the MRI-PDFF is a highly reliable modality for detecting steatosis, comparable to liver biopsy, it is useful for sequent monitoring, such as in clinical trials.
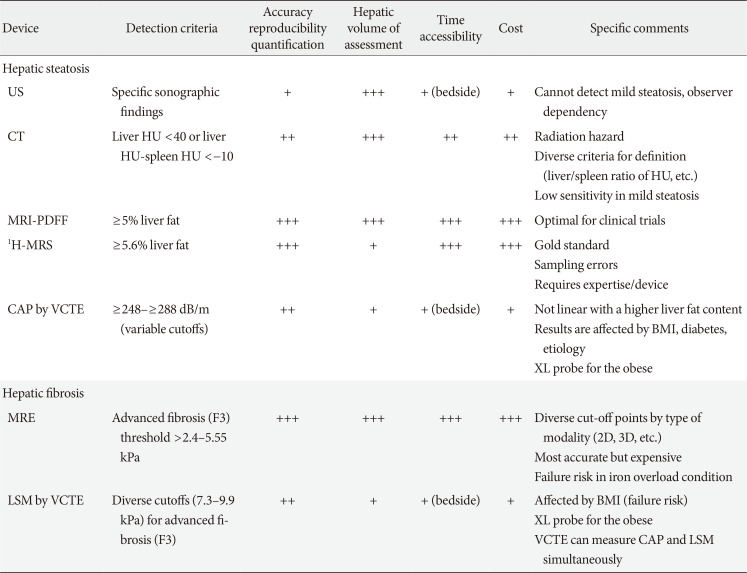
Currently, US, computed tomography (CT), MRI, 1H-MRS, and VCTE are available tools to measure NAFLD depending on the center or clinic (Table 2, Fig. 1).
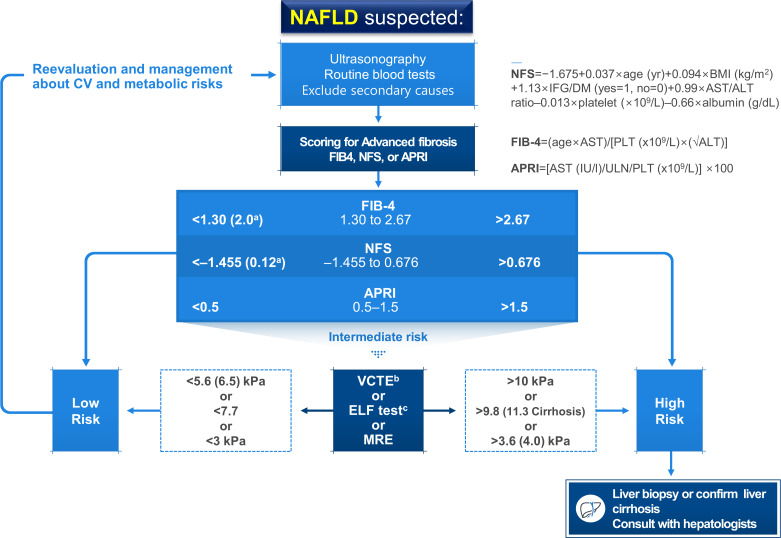 | Fig. 1Algorithm for non-alcoholic fatty liver disease (NAFLD) evaluation. CV, cardiovascular; NFS, NAFLD fibrosis score; BMI, body mass index; IFG, impaired fasting glucose; DM, diabetes mellitus; AST, aspartate aminotransferase; ALT, alanine aminotransferase; FIB-4, fibrosis-4; PLT, platelet; APRI, AST to platelet ratio index; ULN, upper limit of normal; VCTE, vibration-controlled transient elastography; ELF, enhanced liver fibrosis; MRE, magnetic resonance elastography. aHigher cutoffs for patients aged >65 years, bVariable cutoffs have been suggested. Measured values are affected by body factors, cFurther validation is required.
|
Table 2
Summary of the currently used imaging devices for the quantification of hepatic steatosis and fibrosis
US, ultrasonography; CT, computed tomography; MRI-PDFF, magnetic resonance imaging-proton density fat fraction; 1H-MRS, proton magnetic resonance spectroscopy; CAP, controlled attenuation parameter; VCTE, vibration-controlled transient elastography; BMI, body mass index; MRE, magnetic resonance elastography; LSM, liver stiffness measurement.
![]()
Ultrasonography and computed tomography
US is the recommended first line screening method for patients with T2DM by the European NAFLD guidelines [34]. US has interobserver variability and limited sensitivity to detect mild (<20%) steatosis [38], while optimum sensitivity for liver US was reported to be achieved at a liver fat content of ≥12.5% (sensitivity of approximately 80% to 85%) [3940].
Similar to US, CT has limited sensitivity to detect mild steatosis (<30% liver fat). Radiation exposure is an additional drawback. Thus, CT scans cannot be recommended for the diagnosis of hepatic steatosis [2].
Vibration-controlled transient elastography
VCTE measures the speed of a mechanically induced shear wave across the liver using pulse-echo ultrasonic acquisitions to obtain a liver stiffness measurement (LSM), as a marker of hepatic fibrosis, and ultrasonic attenuation through the liver to derive the CAP, as a marker of hepatic steatosis. VCTE is an easy-to-perform tool to obtain both LSM and CAP values using an M (3.5 MHz, at 2.5 to 6.5 cm-depth) or XL (2.5 MHz, at 3.5 to 7.5 cm-depth) ultrasound probe. Although LSM and CAP values are relatively reliable and well-validated, these parameters are affected by various patient factors, especially body mass index which may lead to an overestimation [4142]. With the availability of the XL probe, which has been proven for use in patients with morbid obesity, the failure rate of VCTE for obtaining the LSM and CAP values was reported to be less than 5%, while the significant disagreement between the first and second readings for LSM and CAP when obtained back to back was 18% and 11%, respectively [43].
Magnetic resonance imaging-based techniques
MRI-PDFF can provide fast, quantitative, accurate, and generalized hepatic fat measurements for the entire liver, thereby overcoming the heterogeneity of fat deposition [4445], while magnetic resonance elastography (MRE) is a useful diagnostic tool for the differentiation of histologically determined advanced liver fibrosis from non-advanced fibrosis [4647]. Additionally, LSM measured by MRE may reflect whole liver pathology rather than that of a very small area. MRI-PDFF is becoming the gold standard for hepatic steatosis quantification [48]. MRI-PDFF or 1H-MRS can measure liver fat more precisely than biopsy [4950]. In a secondary analysis of a clinical trial involving patients with biopsy-proven NASH, it was shown that histologic responders (≥2-point reduction in NAFLD activity score [NAS], without any worsening of fibrosis on liver biopsy) had a proportional reduction in the MRI-PDFF of 29.3% from baseline which was statistically significant when compared with histologic nonresponders [51]. However, at the present time, magnetic resonance techniques cannot be used for the assessment of NASH resolution or the exact assessment of fibrosis progression or improvement. Thus, these issues need to be addressed when designing future clinical trials.
Liver biopsy
Liver biopsy provides an accurate diagnosis in approximately 90% of patients with unexplained abnormalities revealed by liver function tests [52]. Noninvasive tools for fibrosis staging are not reliable for therapeutic or other decisions but may be helpful for excluding the probability of significant fibrosis and for predicting advanced fibrosis, thus guiding the decision to perform liver biopsy or not in a patient with NAFLD [53].
Further studies are required to determine whether an active NASH screening strategy in patients with T2DM and active therapy on the basis of the currently available evidence are cost-effective and beneficial for long-term CV and liver-related outcomes. Health care providers taking care of patients with diabetes are strongly encouraged to be vigilant for any signs and symptoms of chronic liver disease and, if indicated, further assessment of the stage of hepatic fibrosis should be conducted [5455].
Further assessment after the diagnosis of hepatic steatosis
Keynotes
- Staged approaches are recommended to determine the extent of liver fi-brosis in patients with NAFLD.
- To estimate hepatic fibrosis using nonimaging modalities, noninvasive biomarker models such as fibrosis-4 (FIB-4) or the NAFLD fibrosis score (NFS) are well-validated and widely used for screening high-risk patients.
- To assess liver fibrosis, VCTE is a point-of-care imaging device with moderate accuracy and high accessibility, while MRE has better accuracy performance, but it is not widely available.
The severity of hepatic fibrosis is the most powerful determinant of long-term outcomes, including mortality [31]; thus, the assessment of fibrosis is essential to manage patients with NAFLD. Although quantitative noninvasive imaging assessment of steatosis is feasible in the clinical setting, none of the current imaging technologies can reliably differentiate simple steatosis from NASH or detect its progression to early stage fibrosis [56]. Several prediction scores have been developed and validated to identify or exclude advanced fibrosis (≥F3). First-line testing should use either FIB-4 or the NFS. As an alternative, the AST to platelet ratio index [APRI] may also be used. Those patients with indeterminate FIB-4 (1.3 to 2.67) or NFS scores (−1.455 to 0.676) require a second-line test in a context dependent manner: VCTE, serum enhanced liver fibrosis (ELF) score, or MRE. The ELF score is a surrogate index based on extracellular matrix panel consisting of plasma concentrations of hyaluronic acid, tissue inhibitor of metalloproteinase 1, and procollagen type III amino-terminal peptide [57] However, the ELF test seems to need further validation, even though European guidelines recommend the test [34]. Patients with high FIB-4 (>2.67) or NFS (>0.676) values should be considered for referral to a specialist clinic irrespective of second-line tests (Fig. 1) [33]. Thus, the use of these scores in combination with imaging studies seems to be more reasonable. The cytokeratin 18 fragment test did not outperform AST measurement in discriminating NASH from simple steatosis [58].
By using VCTE, the threshold values of CAP (≥263 to 288 dB/m) for steatosis and the LSM (≥8.6 to 9.6 kPa) for advanced fibrosis have been variably reported [3948]. The very low values of the LSM (e.g., <5.6 or <6.5 kPa combined with a result from other noninvasive tests) suggest an exclusion of moderate fibrosis (Fig. 1) [59]. Although the threshold levels for the changes of MRI-PDFF to define improvement of steatosis seem to be 25% to 30%, the cutoff value for percent change in MRE to define the improvement of fibrosis needs further studies; it seems that more than a 20% difference is required to be confident [60].
Genetic variant study
Keynotes
- Genetic tests for the assessment of NAFLD are not officially recommend-ed, but identifying the carriers of high-risk genetic variants may be help-ful in some specific conditions.
Genetic factors are also important factors that determine susceptibility to the development and progression of NAFLD, considering that heritable factors account for approximately 50% of the interindividual differences in the prevalence of NASH with cirrhosis in a twin study [61]. Among several genetic risk factors, single-nucleotide polymorphisms (SNPs) in patatin-like phospholipase domain–containing 3 (PNPLA3) (rs738409 c.444 C>G, p.I148M), transmembrane 6 superfamily, member 2 (TM6SF2) (rs58542926 c.449 C>T, p.E167K), and membrane bound O-acyltransferase domain containing 7-transmembrane channel-like 4 (MBOAT7) (rs641738 C>T) have been relatively well validated to promote the development of NAFLD and its progression (i.e., cirrhosis, HCC, or both) [6263646566].
PNPLA3 encodes adiponutrin, a triglyceride (TG) lipase that regulates both TG and retinoid metabolism. The PNPLA3 I148M variant is resistant to proteasomal degradation by evading ubiquitylation and accumulates on lipid droplets, which interferes with lipolysis and causes a change in phospholipid remodeling [67]. The PNPLA3 SNP rs738409 is strongly associated with hepatic steatosis, steatohepatitis, fibrosis, and HCC [66].
TM6SF2 is involved in very low-density lipoprotein (VLDL) secretion from hepatocytes. The SNP rs58542926 C>T in TM6SF2 results in a loss-of-function, inducing a higher liver TG content and lower circulating lipoproteins. As with PNPLA3, the TM6SF2 minor (T) allele is associated with greater hepatic steatosis, more severe NASH and greater hepatic fibrosis/cirrhosis, but intriguingly, the more common major (C) allele is associated with the promotion of VLDL excretion, conferring an increased risk of dyslipidemia and cardiovascular disease (CAD) [6568]. In line with this, in a large exome-wide association study of plasma lipids in more than 300,000 individuals, the PNPLA3 I148M and TM6SF2 E167K variants were strongly associated with hepatic steatosis and progression to NASH, cirrhosis, and HCC, but also with increased risk of diabetes, lower blood TG, lower low-density lipoprotein cholesterol (LDL-C) concentrations, and protection from CAD [66].
The MBOAT7 rs641738 T allele is associated with reduced MBOAT7 protein expression and has been shown to be associated with an increase in the risk of steatosis and histologic liver damage in NAFLD (i.e., higher severity of necro-inflammation and fibrosis) independent of obesity [69]. The variant may also predispose patients to HCC in patients without cirrhosis [6570]. The MBOAT7 gene encodes lysophosphatidylinositol (LPI) acyltransferase 1, known as LPIAT1 or MBOAT7, which selectively uses LPI and arachidonoyl-CoA to form 2-arachidonoyl phosphatidylinositol (PI) [7172]. Consistent with this function, lipidome changes in the plasma and liver of patients with NAFLD have been reported: decreases in plasma levels of PI (36:4), PI (38:3), and PI (38:5) and decreases in hepatic concentrations of PI (36:4) and PI (38:3) in proportion to the number of MBOAT7 variant alleles [6973]. LPIAT1 contributes to the regulation of free arachidonic acid in the cell through the remodeling of phospholipids [74]. MBOAT7 deficiency is thus predicted to increase free polyunsaturated fatty acids and their pro-inflammatory eicosanoid lipids [7075].
Interestingly, in an Italian cohort study that evaluated the relationship between HCC risk and the total number of risk alleles including PNPLA3 I148M, TM6SF2 E167K, and MBOAT7 rs641738 T, there was a significant association between the number of risk alleles and HCC [70].
In addition, several protective variants have also been reported [76]. In particular, SNPs (rs72613567, rs62305723, and rs6834314) in HSD17B13, a gene that encodes the hepatic lipid droplet protein 17β-hydroxysteroid dehydrogenase type 13, were reported to be associated with decreased inflammation, ballooning, and liver enzyme levels in patients with NAFLD [7778]. Recently, HSD17B13 was identified as a lipid droplet enzyme retinol dehydrogenase, highlighting the importance of retinoid homeostasis in NAFLD and its progression [78]. The splice variant rs72613567 produces a truncated, nonfunctional protein that was associated with lower odds of various liver diseases and HCC [77]. It was also found that the isoform encoded by the protective allele is catalytically defective against estradiol [77].
Nutritional factors are very important even when considering genetic factors, as adiposity has been shown to amplify the effect of the NAFLD risk alleles in PNPLA3, TM6SF2, and glucokinase regulatory protein (GCKR) [7980]. Currently, genetic tests are not officially recommended, but identifying carriers of high risk genetic variants may be helpful in some specific conditions.
Go to :
TREATMENT OF NAFLD
Keynotes
- Management for patients with T2DM and NAFLD should be aimed at reducing the risk factors associated with their high CV risk as well as de-creasing hepatic fat accumulation and delaying the progression of inflam-mation and fibrosis.
- Lifestyle modification is the first step in the management for all patients with T2DM and NAFLD to improve NAFLD as well as hyperglycemia, dyslipidemia, and blood pressure levels.
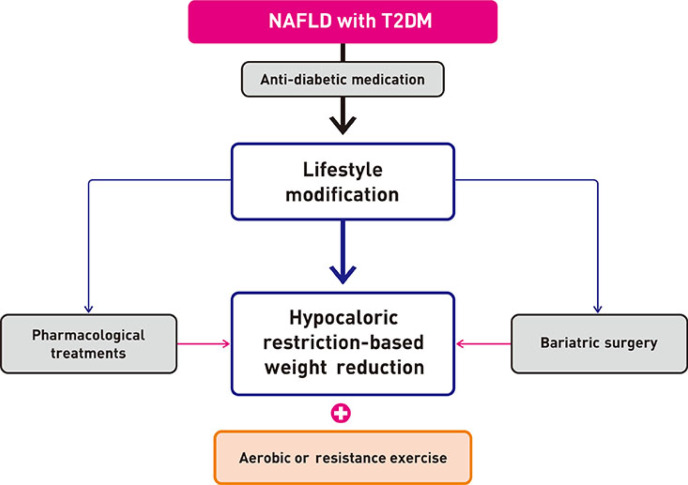
Epidemiological evidence suggests a strong bidirectional relationship between T2DM and NAFLD. Furthermore, NAFLD resolution attenuates T2DM risk, but when obesity, insulin resistance, or hyperglycemia is combined with NAFLD, the T2DM risk is significantly increased [4]. In a long-term follow-up study of patients with NAFLD, diabetes and smoking, along with fibrosis, age, and absence of statin use, contributed to mortality, underscoring the need for a comprehensive approach to patient management [32]. Additionally, spontaneous regression of NASH and even NASH-related fibrosis has been observed in clinical trials and may be related to lifestyle modifications and behavioral changes [81]. However, pharmacological treatment is more powerful than lifestyle modification for glucose control. Moreover, lifestyle modification plus anti-diabetic drugs are likely to have a synergistic effect on reducing the risk factors associated with CV risk and decreasing hepatic fat accumulation in these patients, thereby delaying the progression of inflammation and fibrosis. Therefore, all patients with T2DM and NAFLD should be strongly encouraged to adopt both lifestyle changes and anti-diabetic medication use (Fig. 2) [382].
Weight reduction
Keynotes
- Weight loss induced by either lifestyle modification or bariatric surgery improves glucometabolic profiles and reduces liver fat in subjects with T2DM.
- Regarding lifestyle modification, specific diets rather than calorie restric-tion or specific types of exercise protocols (aerobic or resistance) were not clearly defined for their efficacy at the present time.
It is well established that weight loss induced by either lifestyle modification or bariatric surgery in overweight or obese individuals with T2DM results in significant improvement or resolution of T2DM and its comorbidities such as hypertension, and hyperlipidemia [38384]. In addition, weight reduction has been associated with alleviated intrahepatic fat contents and aminotransferase levels [81]. Even relatively small amounts of weight loss can reduce liver fat and improve hepatic insulin resistance independent of any changes in insulin-stimulated peripheral glucose metabolism [85]. In adult populations with NAFLD, a systematic review that included a total of 23 studies evaluating the effect of lifestyle interventions, such as diet, physical activity, and/or exercise, on the hepatic indicators of steatosis, inflammation and fibrosis as well as glucose control/insulin sensitivity showed that the reductions in liver fat and/or liver aminotransferase concentrations were strongly correlated with weight loss [86]. However, it should be noted that sustainable maintenance of weight loss with lifestyle interventions for long-term periods was achievable in only 3% to 6% of the subjects [915].
The magnitude of weight reduction
Keynotes
- The improvement in histology is proportional to the magnitude of the weight loss, but this proportional trend might not be applicable to gluco-metabolic profiles.
- A magnitude of weight loss in the range of approximately 5% to 7% may clearly decrease steatosis but approximately 8% to 10% weight reduction is needed to reverse steatohepatitis.
In adult populations with NAFLD, a greater degree of weight loss, induced by either lifestyle modifications or bariatric surgical procedures, is associated with a greater improvement in histologic features [82]. Summarizing all current available reports, it appears that a magnitude of weight loss in the range of approximately 5% to 7% may clearly decrease steatosis and the associated metabolic parameters, but 8% to 10% weight reduction is needed to reverse steatohepatitis [38385868788]. Although a ≥7% weight loss also improved NAS, fibrosis was unchanged. Furthermore, the highest rates of NAS reduction, steatohepatitis resolution, and fibrosis regression occurred in patients with ≥10% weight loss [89]. The threshold of 7% weight loss was achieved by <50% of patients, even with intensive multidisciplinary lifestyle intervention.
Lifestyle modification
Keynotes
- The weight reduction achievable by dietary program remains the corner-stone of lifestyle modification for patients with T2DM and NAFLD.
- Caloric restriction, rather than dietary macronutrient composition, has a greater role in preventing the development and progression of T2DM, in reducing hepatic steatosis and in delaying inflammation and fibrosis.
- Exercise per se can reduce hepatic fat even in the absence of weight loss. Both aerobic and resistance exercise leading to a similar weight reduction are similarly effective in hepatic fat reduction in patients with T2DM.
- Individually tailored approaches combining a mainly hypocaloric diet in conjunction with a progressive increase in aerobic exercise/resistance training are associated with the magnitude of the weight reduction.
Of the ways to achieve weight reduction, lifestyle modification that includes a programmed diet and exercise is an effective and sound treatment for all patients with NAFLD and NASH [348290]. In addition, lifestyle modification improves hyperglycemia, atherogenic dyslipidemia, and blood pressure levels [919293]. Of the lifestyle programs, however, weight reduction achievable by dietary programs or interventions remains the cornerstone of lifestyle modification for all patients with T2DM and NAFLD [348290]. It seems that caloric restriction, rather than dietary macronutrient composition, has a greater role in reducing hepatic fat and delaying the progression of inflammation and fibrosis in patients with NAFLD [81838586949596]. Regarding the macronutrient composition, comparable effects have been observed with equally hypocaloric low-carbohydrate versus high-carbohydrate diets [97] and low-fat versus low-carbohydrate diets [98]. Exercise trials have reported an inconsistent amount of weight loss or changes in surrogate biomarkers achieved after exercise interventions, but the heterogeneities of the baseline characteristics of the study subjects and the exercise protocols must also be considered [399100]. Even with these findings, physical activity, either aerobic or resistance type, should be strongly promoted for the management of fatty liver in patients with T2DM because the benefits are not exclusively contingent upon weight loss [101]. It seems that, despite the unclear beneficial roles of exercise on weight loss and hepatic fat reduction, exercise itself has been shown to improve liver enzymes and insulin resistance in all patients with diabetes with NAFLD and NASH [102103]. A comprehensive approach with combined dietary and exercise interventions has shown significant benefit on NAFLD, especially for long-term intervention periods. However, whether a combined lifestyle intervention has synergistic effects compared to the separate approaches of diet and exercise is unclear. A meta-analysis by Keating et al. [102] showed that a combined dietary and exercise intervention had no significant pooled effects size (ES) when compared to diet alone (ES: −0.05; 95% confidence interval, −0.38 to 0.27; P=0.76). However, another systematic review that included eighteen studies to investigate whether a diet-plus-exercise intervention for a minimum of 6 months was more effective for weight loss than a diet-only intervention among obese or overweight adults showed that a combined diet-plus-exercise intervention provided greater long-term weight loss than a diet-only intervention [104]. Although the effects of lifestyle modification in the absence of weight loss on NAFLD and NASH might not be clear, it is clear that lifestyle changes with either or both a hypocaloric diet and exercise reduce the risk of CV disease and the onset and progression of T2DM [3482105].
Pharmacologic treatment
For patients with T2DM and NAFLD, however, pharmacological treatment is more powerful than lifestyle modification for glucose control. Moreover, lifestyle modification plus anti-diabetic drugs are likely to offer synergistic benefits for reducing the risk factors associated with their high CV risk [391] as well as decreasing hepatic fat accumulation and delaying the progression of inflammation and fibrosis. Therefore, especially in patients with T2DM, all patients should adopt both lifestyle changes and anti-diabetic medication use [82].
Anti-diabetic agents
Keynotes
- Patients with T2DM and NAFLD should adopt both lifestyle changes and anti-diabetic medication use.
- There are no definite pharmacologic treatments for NAFLD in patients with T2DM.
- Metformin is not recommended for treating NAFLD in patients with T2DM.
- Currently, pioglitazone could be a 1st-line option to improve NASH in patients with T2DM with some improvement in fibrosis.
- Evidence that sodium-glucose cotransporter 2 (SGLT2) inhibitors im-prove NAFLD/NASH with fibrosis in patients with T2DM is emerging. Although not generally recommended, these agents may be considered as an initial treatment option in specific conditions for the treatment of NAFLD in patients with T2DM.
- Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have some evi-dence of improving NAFLD/NASH with fibrosis, but these agents are not generally recommended for the treatment of NAFLD in patients with T2DM.
- Dipeptidyl peptidase-4 (DPP-4) inhibitors are not recommended for treating NAFLD in patients with T2DM.
1) Metformin
Studies on metformin use in NAFLD failed to show any improvement in liver histology in patients with NAFLD and NASH [106107]. Thus, metformin is not recommended for treating NAFLD in patients with T2DM. However, T2DM is now considered an independent risk factor for HCC and metformin may have a protective role in HCC occurrence [108].
2) Thiazolidinediones
Pioglitazone, one of the thiazolidinediones, is a peroxisome proliferator-activated receptor (PPAR)-γ agonist with insulin-sensitizing effects. An randomized controlled trial (RCT) evaluating the efficacy and safety of long-term pioglitazone (45 mg/day) treatment in patients with biopsy-proven NASH and prediabetes or T2DM showed that compared with the placebo group, only patients with T2DM showed a significant resolution of NASH (60% vs. 16%) and reduction in fibrosis from baseline [109]. Currently available data from previous studies suggest that, although it may reduce fibrosis, the clinical effect of pioglitazone may come from the suppression of rapid fibrosis progression rather than from fibrosis regression by turning off the metabolic drivers of liver fibrosis in T2DM [109110]. Pioglitazone could be a first-line therapy for patients with NASH and T2DM. However, pioglitazone should not be routinely used to treat NAFLD in patients with T2DM because of limited data and the common side effects of weight gain, fluid retention, and bone mass loss.
Lobeglitazone is currently being prescribed for T2DM in Korea. In a multicenter, prospective clinical trial, patients with T2DM and NAFLD treated with lobeglitazone (0.5 mg daily) for 24 weeks had improved liver enzymes and ameliorated hepatic fat contents assessed by VCTE-CAP [111].
3) Sodium-glucose cotransporter 2 inhibitors
SGLT2 inhibitors, including dapagliflozin, canagliflozin, empagliflozin, ipragliflozin, and luseogliflozin are being used increasingly in the treatment of T2DM; they promote weight loss which is an attractive property for the treatment of patients with NAFLD. Although SGLT2 inhibitors are not yet generally recommended for the treatment of NAFLD in patients with T2DM, emerging data suggest that SGLT2 inhibitors reduce the risk of progression of NAFLD [112], as the following results have been reported: a decrease in hepatic fat content [113114]; a decrease in AST and ALT [114115]; a decrease in the measures of fibrosis, such as the FIB-4 index [115116], the fibrosis index calculated from hyaluronic acid and type IV collagen 7S [116], and VCTE-measured LSM [117]; an improvement in hepatic insulin sensitivity [114]; and histology [118]. Well-designed RCTs are needed to elucidate whether SGLT2 inhibitors should be used as the first-line drug choice in patients with NAFLD/NASH with T2DM. In the meantime, these agents may be considered as an initial option to treat NAFLD in patients with T2DM and specific cardio-renal conditions [119].
4) Glucagon-like peptide-1 receptor agonists
GLP-1 RAs, including exenatide, lixisenatide and liraglutide, are promising candidates for the treatment of NAFLD and NASH because they can reduce weight and enhance insulin action. However, GLP-1 RAs are not generally recommended for the treatment of NAFLD in patients with T2DM because of the limited data to date [112]. In a well-performed clinical trial in patients with biopsy-proven NASH, liraglutide (1.8 mg daily) treatment for 48 weeks was associated with greater resolution of steatohepatitis and less progression of fibrosis [120].
5) Dipeptidyl peptidase-4 inhibitors
DPP-4 inhibitors including sitagliptin, vildagliptin, linagliptin, saxagliptin, gemigliptin, alogliptin, teneligliptin, and anagliptin are commonly used in patients with T2DM, but there are few studies about the efficacy of DPP-4 inhibitors in patients with T2DM and NAFLD; they are not yet believed to have a beneficial effect on NAFLD. Only vildagliptin showed a clinically significant decrease in hepatic TG levels measured by MRI-PDFF (27% with vildagliptin, from 7.3%±1.0% [baseline] to 5.3%±0.9% [endpoint]), unrelated to changes in body weight, during 6 months of therapy in patients with T2DM and NAFLD [121]. Mixed results have been reported for sitagliptin. A pilot clinical study demonstrated that sitagliptin could improve hepatocyte ballooning and liver enzymes in patients with T2DM and NASH after 1 year of treatment [122]. However, many other studies have failed to show an effect of sitagliptin treatment on liver fat content or liver stiffness [123124].
Non-antidiabetic agents
Keynotes
- Vitamin E is not recommended to treat NAFLD in patients with T2DM.
- Lipid-lowering agents such as statins, ezetimibe, fibrates, niacin, omega-3 polyunsaturated fatty acids, and colesevelam did not improve hepatic ste-atosis in patients with NAFLD.
- Ursodeoxycholic acid (UDCA) and pentoxifylline are not recommended for the treatment of NAFLD or NASH.
- Obeticholic acid may improve NASH without progression of fibrosis in patients with T2DM and NASH. Further studies are required to prove its efficacy and long-term effects as well as its adverse effects.
1) Vitamin E
Vitamin E is an antioxidant that prevents liver injury by blocking intrinsic apoptotic pathways and protecting against oxidative stress. Vitamin E improves liver histology in nondiabetic adults with biopsy-proven NASH [125], but is not recommended in patients with diabetes because of a lack of evidence [582]. In addition, there are some concerns that long-term use of vitamin E may be associated with increased all-cause mortality, an increased incidence of hemorrhagic stroke, and an increased risk of prostate cancer.
2) Lipid-lowering agents
Although statins are beneficial in the management of dyslipidemia and high CV risk as well as in reducing the risk of HCC and mortality, especially in patients with diabetes, lipid-lowering agents such as statins, ezetimibe, fibrates, niacin, omega-3 polyunsaturated fatty acids, and colesevelam did not improve hepatic steatosis in patients with NAFLD [582126]. There was also no evidence for the use of one of these agents for the treatment of NAFLD in patients with T2DM.
3) Ursodeoxycholic acid
UDCA, a naturally occurring bile acid, reduced oxidative stress and had antiapoptotic properties. Although several studies reported that UDCA improved liver enzymes and hepatic steatosis in patients with NAFLD [127128], both conventional (13 to 15 mg/kg daily) and high (23 to 28 mg/kg daily) doses of UDCA failed to induce histologic improvement in patients with NASH [129130].
4) Pentoxifylline
Pentoxifylline inhibits a number of proinflammatory cytokines including tumor necrosis factor-α. Although pentoxifylline (400 mg three times a day) improved the histological features of NASH in 55 adults with biopsy-confirmed NASH, only 9.1% of participants had T2DM [131]; another study reported no histological improvement in 30 patients, so larger studies are needed to establish the role of pentoxifylline in the management of patients with NASH and T2DM [132].
5) Obeticholic acid
Obeticholic acid is a natural agonist of the farnesoid X receptor and decreases insulin resistance and hepatic steatosis in animal models. Obeticholic acid (25 mg daily) treatment for 72 weeks, where 52.7% of patients had T2DM, improved liver histology in patients with NASH but increased LDL-C levels and caused pruritus [133]. Further studies are needed to clarify the long-term benefit and safety of obeticholic acid in patients with T2DM and NAFLD.
6) Carnitine
Carnitine is a modulator of mitochondrial free fatty acid transport and oxidation and has antioxidative activity in hepatocytes [98]. In patients with NASH, L-carnitine treatment (1 g daily) for 24 weeks improved liver enzymes and histological manifestations [134]. Treatment with the carnitine-orotate complex (824 mg, three times daily) for 12 weeks in patients with T2DM and NAFLD improved serum ALT and improved hepatic steatosis as assessed by CT in 78 patients [135].
7) Elafibranor
Elafibranor is a dual agonist of PPAR-α and PPAR-δ and improves insulin resistance in liver and peripheral tissue. In a phase 2b trial, elafibranor treatment (120 mg daily) for 52 weeks tended to induce resolution of NASH without fibrosis progression despite some methodological limitations. The predefined endpoint was not met in the intention to treat population and 39.1% of study participants had T2DM [136].
8) Cenicriviroc
Cenicriviroc, a dual antagonist of the C-C chemokine receptor types 2 and 5, has potent anti-inflammatory and antifibrotic activity in animal models. In a phase 2b study, in which half of subjects had T2DM and two-thirds had metabolic syndrome, cenicriviroc treatment (150 mg daily) for 1 year achieved improvement in fibrosis and no worsening of steatohepatitis compared with placebo [137].
9) Anti-obesity drugs
Because weight reduction is a key component for the treatment of NAFLD, anti-obesity drugs can be potential candidates. However, few studies have investigated the efficacy of anti-obesity drugs for the treatment of NAFLD. Orlistat (120 mg three times daily for 6 months), an inhibitor of fat absorption, showed improved steatosis assessed by US and confirmed by liver biopsy in patients with NAFLD [138]. Another study evaluated the effect of orlistat on NAFLD in patients who received a 1,400 kcal/day diet plus vitamin E (800 IU) daily. Orlistat (120 mg three times a day) did not enhance weight loss or improve liver enzymes and histopathology in fifty overweight subjects (10% of subjects had T2DM) [139].
Bariatric surgery
Keynotes
- In addition to its effects on body weight and metabolic profiles, bariatric surgery can decrease long-term mortality related to diabetes, CV diseas-es, and cancers.
- Bariatric surgery can be considered in obese patients with NAFLD and T2DM to resolve NASH and improve fibrosis.
Bariatric surgery has been accepted as a treatment option in obese patients with T2DM who do not achieve durable weight loss and improvement in comorbidities (including hyperglycemia) with nonsurgical methods [119]. A meta-analysis showed that the majority of patients undergoing bariatric surgery appear to improve or completely resolve the histopathological features of steatosis, inflammation, and ballooning. Fibrosis also improved by a weighted mean decrease of 11.9% in the incidence of fibrosis [140]. Another recent meta-analysis including 3,093 biopsies also reported the resolution of steatosis in 66% of patients, inflammation in 50%, ballooning degeneration in 76%, and fibrosis in 40% [141]. With regard to procedure selection, there is still a lack of data on which method, i.e., sleeve gastrectomy or Roux-en Y gastric bypass, is more effective. However, considering the safety of the surgery itself, sleeve gastrectomy is recommended in patients with NASH cirrhosis [82142143].
Go to :
 XML Download
XML Download