

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Streptococcus agalactiae, also known as Group B streptococcus (GBS), is part of the normal flora of the female urogenital tract and rectum. GBS are clinically important because they can be vertically transferred during the delivery of neonates, causing sepsis and meningitis in neonates and young infants and leading to other serious infections in women during the gestational and postpartum period [12].
Capsule production is an important virulence factor for GBS. Based on the recognized capsular polysaccharide (cps) antigens, GBS is classified into 10 serotypes, of which nine serotypes, i.e. Ia, Ib, and II-VIII, are considered as clinically important [23]. Previous reports worldwide have indicated that serotypes Ia, II, III, and V represent 80 – 90% of GBS isolates and are mainly involved in human diseases [23456].
In addition to its role in epidemiology and pathogenesis studies, capsular polysaccharide typing is important for surveillance programs and vaccine development [34567]. For example, serotype III is often involved in neonatal diseases followed, by types Ia, Ib, II, and V [23456]. Therefore, potential GBS vaccines must contain these capsular antigens [7].
GBS capsular typing is commonly performed by using immunoassays, particularly latex agglutination based on polyclonal antibodies specific for the recognized capsular polysaccharides [8]. However, immune-based serotyping has certain limitations, most importantly the difficult interpretation of some strains that either cross-react with multiple antisera or fail to react with any of the available antisera and remain untyped. Furthermore, these methods may not distinguish whether strains express capsular polysaccharide-related genes (non-encapsulated) or polysaccharide variants [9]. Capsular gene-based molecular typing (genotyping) is a suitable alternative method, and several methods for typing of S. agalactiae based on polymerase chain reaction (PCR) targeting cps operon have recently been published [101112].
This study was conducted to determine the colonization rate of GBS among pregnant women in Makkah, Saudi Arabia, focusing on the frequency of different serotypes among recovered clinical isolates and their antibiotic susceptibility patterns.
Materials and Methods
1. Study design
In this cross-sectional study, 400 Saudi pregnant women at ≥35 gestation weeks attending the antenatal clinic of Maternity and Children Hospital in Makkah were investigated over a period of 1 year (January 2018 to December 2018). Vagino-rectal swabs were collected from each subject in a sterile manner and transferred to the Microbiology Laboratory of Department of Laboratory Medicine, Faculty of Applied Medical Sciences, Umm Al Qura University, for further investigation.
2. Isolation and identification of GBS isolates
For GBS isolation, vagino-rectal swabs were first inoculated into Todd-Hewitt broth supplemented with gentamicin (8 μg/mL) and nalidixic acid (15 μg/mL) and incubated at 37°C for 36 h. The broth was then sub-cultured onto sheep blood agar and incubated in 5% CO2 for 18 – 24 h [1]. Isolates were identified using a Microscan WalkAway 40 Si Microbiology Analyzer (Siemens AG, Inc., Munich, Germany). The organisms were then confirmed as group B streptococcus by performing a latex slide agglutination test using a MASTASTREP kit (Mast House, Merseyside, UK).
3. Antibiotics susceptibility test of GBS isolates
Antimicrobial susceptibility testing of each GBS isolate was performed using the gram-positive susceptibility panel (PBC-28) of Microscan WalkAway 40 Si Microbiology Analyzer.
4. Detection of inducible clindamycin resistance
The inducible resistance of clindamycin was determined for isolates that showed resistance to erythromycin but susceptibility to clindamycin in the antibiotic susceptibility test. The D-zone test was performed using the disk diffusion method according to Clinical Laboratory Institute Standards guidelines [13].
5. Serotyping of GBS isolates by latex agglutination
After confirming the isolates as GBS, each isolate was subjected to serotyping using the ImmulexTM Strep-B latex kit (Staten's Serum Institute, Copenhagen, Denmark). Serotyping was performed according to the manufacturer's instructions.
6. Genotyping of GBS isolates by multiplex PCR
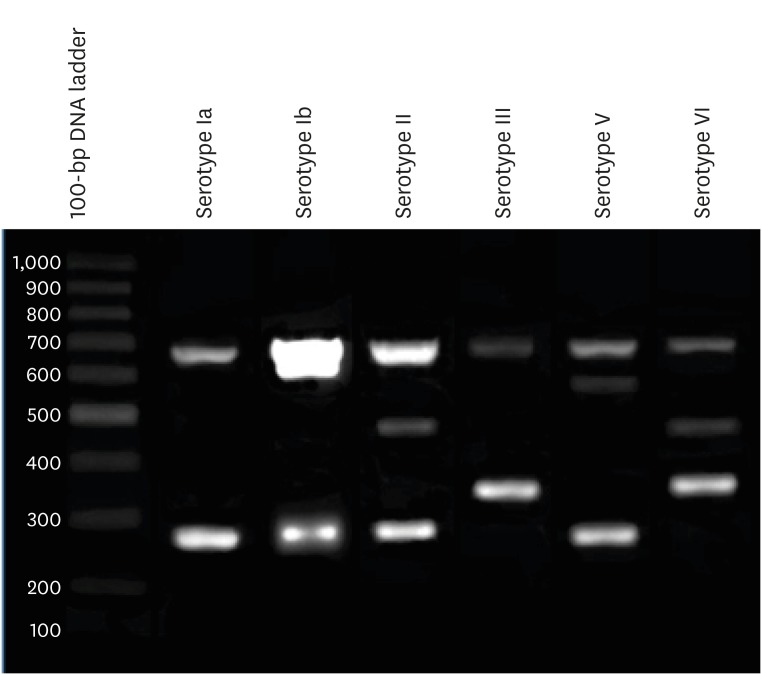
Genomic DNA was extracted from GBS isolates using a Gentra Puregene yeast/Bact. kit (Qiagen, Hilden, Germany) according to the manufacturer's instructions. Capsular gene-based genotyping of GBS isolates was carried out by multiplex PCR. Briefly, the multiplex PCR assay was performed to identify different GBS serotypes using 19 primers comprising both common and distinctive regions of GBS capsular genes as previously described [12]. The PCR product was electrophoresed in 1 μL Tris-Acetate-EDTA buffer through a 2% agarose gel containing ethidium bromide (0.5 μg/mL). Bands of the appropriate size were visualized using a Molecular Imager® Gel DocTM XR System (Bio-Rad Laboratories, Hercules, CA, USA) according to the manufacturer's instructions and identified by comparison with a 100-base pair (bp) DNA molecular weight marker (Promega, Madison, WI, USA).
7. Ethics statement
The medical ethics committee of Umm Al Qura University reviewed and approved the protocol of the current study, which was conducted in accordance with the Declaration of Helsinki (AMSEC 7/10-12-2017). All participating subjects provided written consent that they acknowledged the inclusion of their data anonymously in the study, and that they would not be identified in the publication.
RESULTS
1. Carriage rate and serotypes of GBS isolates among Saudi pregnant women
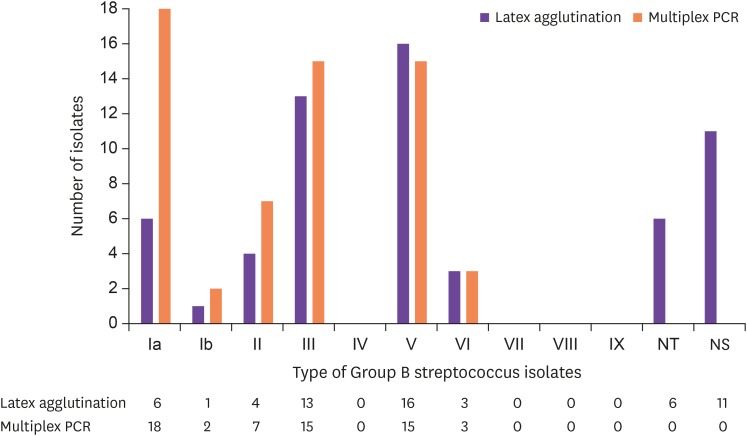
Sixty (15.0%) subjects among the investigated 400 Saudi pregnant women were colonized with GBS isolates. Of the recovered 60 GBS isolates, 43 (71.7%) were clearly assigned to a serotype by the latex agglutination test, whereas 11 (18.3%) showed non-specific (NS) agglutination with more than one antiserum, and 6 (10.0%) did not react with any antisera and were recorded as not-typable (NT). Latex agglutination-serotyped isolates included 6 as serotype Ia (10.0%), 1 as serotype Ib (1.7%), 4 as serotype II (6.7%), 13 as serotype III (21.7%), 16 as serotype V (26.7%), and 3 as serotype VI (5.0%) (Fig. 1). In contrast, multiplex PCR genotyping of GBS isolates revealed specific patterns for each isolate. All recovered patterns are shown in a representative gel in Fig. 2 and corresponded to the following types: 18 were serotype Ia (30.0%), 2 were serotype Ib (3.3%), 7 were serotype II (11.7%), 15 were serotypes III and V (25.0% each), and 3 were serotype VI (5.0%) (Fig. 1).
2. Concordance of GBS typing by latex agglutination and multiplex PCR genotyping
Of the typed 43 isolates by the latex agglutination test, only 34 isolates (79.1%) showed the same results as the molecular typing test, as indicated by bold numbers in Table 1. In contrast, 9 isolates (20.9%) showed discordant results by molecular typing. These included 4 isolates of serotype V and 2 isolates of serotype II in the latex agglutination test, which were typed as Ia by genotyping. Additionally, one isolate was typed VI by latex agglutination, whereas genotyping revealed this isolate as type III; finally, 2 isolates were typed as Ia by the latex agglutination test but typed as V and VI by genotyping (Table 1).
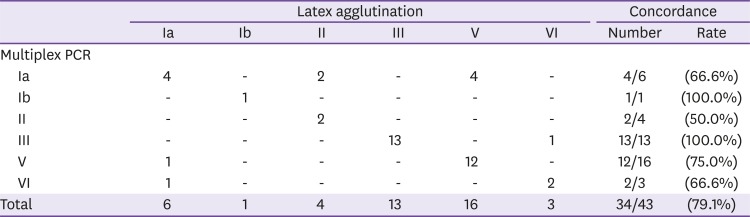
Table 1
Concordance by molecular typing and latex agglutination method
![]()
3. Molecular typing of latex agglutination-NT and NS typed isolates
Genotyping was able to type each isolate of both the NT- and NS-typed GBS isolates by latex agglutination. The 6 NT isolates were typed as II (3), Ia (2), and V (1) by multiplex PCR (Table 2). For the 11 NS-typed isolates, 6 were typed as Ia, 2 as type II, and 1 isolate each as Ib, III, and V (Table 2). Interestingly, all NS-typed isolates, except for 1 (isolate number 25), reacted equally with the antisera of multiple serotypes, of which 1 serotype was identical to the genotyping results. The exceptional isolate reacted positively with both serotype III and V reagents; however, multiplex PCR typed this isolate as Ia (Suppl Table 1).
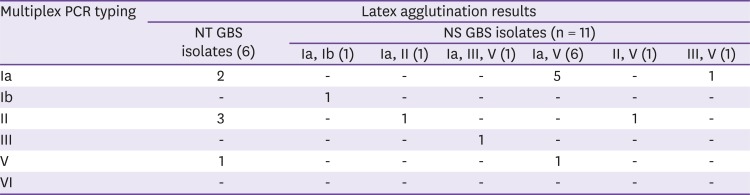
Table 2
Typing of latex agglutination not typable or non-specifically typed Group B streptococcus isolates by multiplex polymerase chain reaction
PCR, polymerase chain reaction; GBS, Group B streptococcus; NT, not-typable; NS, non-specifically typed.
![]()
4. Antibiotic susceptibility of recovered GBS isolates
All GBS isolates were 100% sensitive to penicillin G, ampicillin, linezolid, daptomycin, and vancomycin. The highest resistance was found to erythromycin (10, 16.7%) followed by clindamycin (9, 15.0%), and the lowest resistance was shown toward levofloxacin (2, 3.3%). In addition, 7 isolates were erythromycin-resistant and clindamycin-sensitive. D-Zone testing of these isolates revealed that only 1 isolate showed inducible clindamycin resistance. Thus, 10 isolates were clindamycin-resistant 10 (16.7%) isolates and 4 were resistant to both erythromycin and clindamycin (6.7%).
Analysis of antibiotic susceptibility in the recovered serotypes revealed that resistance to erythromycin and clindamycin was mainly restricted to the 3 predominant serotypes detected in the current study, i.e., Ia, III, and V. However, resistance to levofloxacin was detected only in types III and V (Table 3). The resistance profiles of all GBS isolates are shown in (Suppl Table 2).
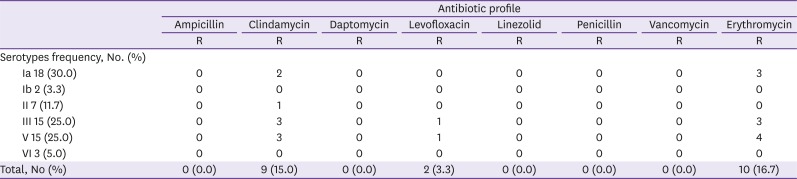
Table 3
Antibiotic susceptibility pattern of Group B streptococcus serotypes (n = 60)
![]()
DISCUSSION
Maternal GBS vagino-rectal colonization is an important risk factor for the development of invasive neonatal infections. A recent review documented worldwide variations in the GBS colonization rate, with values of 10 – 30% in the United States, 6.5 – 36% in Europe, 7.1–16% in Asia, 9.1 – 25.3% in the Middle East, and 11.9 – 31.6% in Africa [14]. The recorded rate of GBS colonization (15%) in the current study is generally within the range reported in other Middle East and Asian countries [1415].
In Saudi Arabia, the currently recorded frequency of GBS colonization is slightly higher than that previously reported from Makkah by the same group, with 13.4% of pregnant women colonized by GBS [16]. As both studies were carried out at the same hospital, these results indicate an increase in the GBS colonization rate among pregnant women in Makkah. Wide geographic variations in the rates of GBS maternal colonization were documented in Saudi Arabia, with higher GBS colonization rates ranging from 19% to 31.6% in Dammam, Taif, Riyadh, and Jeddah [1718192021].
In addition to variations in the GBS colonization rate, a distinct frequency in GBS serotypes has been documented worldwide, with serotypes Ia, II, III, and V as the most commonly encountered types; these types are also associated with human diseases [3456]. Worldwide differences in the distribution of GBS serotypes are generally attributed to geographical variations and differences between ethnic groups [215]. It is important to identify the local serotype distribution to enact appropriate control measures, including the development of specific vaccines against circulating serotypes [9]. Limited data are available regarding the distribution of GBS serotypes from Saudi Arabia and other countries in the region.
The most frequent method used for GBS typing is latex agglutination-based serotyping, whereas the Lancefield precipitation test is less frequently used [22]. Most previous studies serotyped more than 90% of investigated isolates by latex agglutination [2324]. Molecular genotyping was described as an alternative tool for GBS typing [1011]. The capsular gene-based multiplex PCR assay [12] was recently introduced and was used in the present study.
In this study, 28.3% of GBS isolates could not be satisfactorily typed by the latex agglutination test. In contrast, all isolates were successfully typed using the multiplex PCR assay. Our latex agglutination results are very similar to those obtained in a study conducted in Europe, in which 27% of GBS isolates could not be typed by latex agglutination [25]. This suggests that difficulties in serotyping by latex agglutination are quite common. However, a recent study revealed 100% matching between the latex agglutination and PCR methods for GBS typing, demonstrating the reliability of this approach [26]. However, the current study revealed that only 79.1% of latex agglutination-typed isolates showed the same results as multiplex PCR typing. An even lower percentage (71.1%) of agreement between these two methods was reported in a recent study from Norway [27]. Multiple limitations to latex agglutination-based serotyping have been documented, of which immunological cross-reaction is the most common [22232425]. Therefore, the unsatisfactory agreement between serotyping and genotyping may be attributed in part to the cross-reaction with a serotype V latex reagent, which was repeatedly encountered in the current study (Staten's Serum Institute) (Table 2). Similar issues were encountered in a previous study using serotype V and IX latex reagents from the same manufacturer [25]. Another limitation of latex agglutination-based serotyping is the lack of sensitivity with a subsequent failure to identify certain serotypes. In the current study, a significant proportion of isolates (10%) remained as NT. Similar findings were also reported by other researchers who used latex agglutination for GBS serotyping [222527]. The precise reason for this is not known, but it may be related to improper expression of the capsule under laboratory conditions. In contrast, the genotyping method identified all investigated GBS isolates in the current study, including the NT or NS types determined by latex agglutination. These findings agree with those of previous studies showing that all GBS isolates could be typed using molecular methods [10111227]. Thus, we used the genotyping results to determine the frequency of different GBS serotypes in Saudi pregnant women in Makkah.
This is the second study in Saudi Arabia to report the serotype distribution of GBS isolates colonizing the pregnant women in Saudi Arabia. A previous study performed in Riyadh reported serotype II as the most predominant type (42%), followed by serotype IV (16%) and serotype Ia (12%) using the latex agglutination method [19]. The present study is the first study in Saudi Arabia to use molecular genotyping to describe the GBS serotype distribution. In contrast to the former Saudi study, serotype Ia was the most predominant (30%) serotype in the current study, followed by types III and V (25% each), whereas serotype IV, the second most prevalent serotype in the former study, was not detected. Similarly, different serotype distributions were reported in two different localities in Iran, with serotypes V, II, and IV as the most predominant (19.6%, 12.5%, and 12.5%, respectively) in the northwest region of the country [28], whereas in the central region, serotypes III, Ib, and II were the most predominant serotypes (41.8%, 24.45%, and 14.54%, respectively) [29]. Moreover, differences in the serotype distribution were reported in neighboring countries, such as Kuwait and Egypt. In these studies, serotype V was the most prevalent, both in Kuwait (38.5%) and Egypt (33%), whereas serotype Ia showed lower rates (7.7% and 14%, respectively) [3031]. These differences could be simply attributed to the different methods used for typing of recovered GBS isolates, as was encountered in the current study. However, the variation of GBS serotypes distribution could also be linked to regional differences in the demographic makeup of the countries with subsequent variation of its distribution in the region or even within the country as reported earlier [2242829]. This may also explain the recorded variation in the GBS serotype distribution between the former Riyadh (central region) and current Makkah (western region) studies.
Moreover, GBS has been established as a leading cause of neonatal invasive infections globally (1, 3, 6), including in Saudi Arabia, where a recent study reported an overall incidence of GBS cases to be 0.51/1,000 live births; 69.1% had early onset disease and 30.9% had late onset disease [32]. Among them, urinary tract infection was the most common (47.3%), followed by sepsis (43.6%), meningitis (5.5%), and pneumonia (1.8%) with a mortality rate of 3.6%. In contrast, an earlier study from Saudi Arabia reported that the prevalence of early onset GBS disease was 0.52/1,000 live births, and respiratory complications (37.0%) were found to be the most common with a mortality rate of 9.0% [33]. This suggests that studies of the antibiotic resistance of different serotypes are essential for increasing our understanding of effective antimicrobial therapies. Penicillin and ampicillin have been universally established as first-line intrapartum prophylaxis to prevent early-onset neonatal GBS infection [2434]. In the current study, all GBS isolates were 100% sensitive to penicillin, ampicillin, linezolid, daptomycin, and vancomycin, which agrees with the results of previous studies in Saudi Arabia [1619] and other countries [33035] and confirm the expected empiric susceptibility to penicillin. In contrast, clindamycin is recommended as a second-line antimicrobial agent for intrapartum prophylaxis for GBS infections in women who are allergic to penicillin [136]. Resistance to clindamycin and/or erythromycin in GBS strains has been reported in many countries, ranging from 6.4% to 85.7% for erythromycin and 4.2% to 73.2% for clindamycin [2435373839]. The highest rate of resistance for both erythromycin (85.7%) and clindamycin resistance (73.2%) in GBS strains has been reported in China [39]. In the current study, the highest resistance was encountered for both erythromycin and clindamycin (16.7% each). This rate of resistance is slightly higher than that in our previously reported study performed in Makkah (15.7% and 5.1%, respectively) [16]. However, in the previous study, the results could not be directly compared, as serotyping was not carried out. Furthermore, the current study revealed a slight increase in the resistance to erythromycin and a 3-fold increase in the resistance to clindamycin. As in our previous study, a study from Riyadh, Saudi Arabia showed a 10% resistance rate to erythromycin and 6% to clindamycin among GBS isolates [19]. Similarly, during the same period in Kuwait, resistance to erythromycin and clindamycin was (12.6%) and (7.0%), respectively [30]. Even significantly lower resistance (0.18%) to clindamycin with no resistance to erythromycin was reported in a previous study performed in Taif, Saudi Arabia [18]. These findings indicate an increase in the resistance both to erythromycin and clindamycin, which is likely related to antibiotic administration according to individual institutional policies rather than to an adopted national policy. The currently recorded high rate of erythromycin and clindamycin resistance supports current Centre for Disease Control recommendations for the necessity of performing antibiotic susceptibility testing if erythromycin or clindamycin therapy is needed for intrapartum prophylaxis, particularly for mothers allergic to penicillin, to prevent neonatal GBS infection [1].
In a trial to correlate antibiotic resistance patterns with different GBS serotypes colonizing pregnant women, resistance to erythromycin and clindamycin was mainly restricted to the most frequently isolated serotypes (Ia, III, and V), as revealed in this study (Table 3). Similar findings were reported in a study from Korea in which resistance to erythromycin and clindamycin was observed in the most predominant serotypes detected, i.e., type III and V [40]. In addition, a study from Malaysia reported that the rate of resistance to erythromycin (38.0%) was the same in the most predominant serotypes (Ia and III), while resistance to clindamycin was more frequent in serotype III (57.0%) followed by serotype Ia (14.0%) [35]. However, different patterns were observed in a Canadian study in which serotypes III and V were the most predominant but resistance both to erythromycin and clindamycin was prevalent in serotype IV, which was among the least predominant serotypes detected in the study [5]. Similar to the Canadian study, a study in Iran revealed high resistance to clindamycin in the least prevalent serotype III compared to the most prevalent serotype V [28]. In fact, this resistance pattern is difficult to explain; however, the findings of these studies suggest that the resistance to erythromycin and clindamycin is commonly observed in serotype III, regardless of whether this serotype was the least or most prevalent among the population studied. The reported resistance pattern to these antibiotics suggests the requirement for an ongoing monitoring system to determine the trends in antimicrobial resistance for GBS colonizing pregnant women.
In the comparison of the two typing methods, i.e. latex agglutination and multiplex PCR, to designate the specific serotype of each GBS isolate, not all strains could be typed by latex agglutination, as some strains were either non-typable or non-specifically typed. Cross-reactions are often observed with serotype V latex reagent. In contrast, multiplex PCR assigned a specific serotype to each isolate. However, we observed faint but visible bands for serotypes V (582 bp) and VI (470 bp). One of our non-specifically typed isolates, which reacted positively with both serotype III and V latex reagents, was typed as Ia by multiplex PCR. The non-consistent results of this isolate can be confirmed by sequencing, which was beyond the scope of this study.
In conclusion, the current study demonstrated that GBS colonization was prevalent among pregnant women and resistance to erythromycin and clindamycin, with serotypes Ia, III, and V as the predominant types. This is the first study to report the distribution of GBS serotypes in the studied group from Makkah and the first study in Saudi Arabia to use molecular genotyping to identify GBS serotypes. Molecular genotyping using capsular gene-based multiplex PCR provided reliable typing of investigated GBS isolates in terms of sensitivity and specificity as compared to conventional serotyping using latex agglutination. Serotypes Ia followed by types III and V were most predominant among all colonizing GBS isolates. All isolates were 100% sensitive to penicillin, ampicillin, linezolid, daptomycin, and vancomycin; resistance to erythromycin and clindamycin was restricted to the predominant serotypes (Ia, III, and V). These findings regarding the serotype distribution and antibiotic susceptibility patterns among the Saudi pregnant women within the Makkah population represent a valuable contribution to the epidemiological characteristics of GBS in this region and highlight the need to adopt national antenatal policies for GBS followed by intrapartum antibiotic prophylaxis. Further studies are needed to consider active surveillance for invasive diseases associated with GBS colonization.
 XML Download
XML Download