

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Myocardial perfusion positron emission tomography (PET) has the advantages of absolute quantification of myocardial blood flow (MBF) and flow reserve (MFR). It can measure volumetric flow normalized by a specific mass of myocardium without an invasive procedure. PET-measured MBF and MFR add diagnostic value to relative perfusion defect assessments1)2) and facilitate the detection of multivessel disease causing balanced ischemia.3) The prognostic value of PET-measured MFR for other traditional cardiovascular risk factors has been repeatedly demonstrated.4)5)6)
Although the clinical values of MBF quantification using PET are evident, the lack of lesion-specificity limits its integration into the clinical management of coronary artery disease (CAD). PET-measured MBF does not always correlate well to a specific epicardial coronary stenosis due to the anatomical variability of the coronary trees.7) Therefore, it is difficult to establish a normal MBF or MFR threshold or to determine revascularization based solely on MBF or MFR values.
Hybrid imaging of PET and coronary computed tomography (CT) has recently been suggested as an excellent candidate for the evaluation of CAD. The additional anatomical information provided by coronary CT enables correlation of perfusion abnormality with a specific epicardial coronary lesion8) and a comprehensive interpretation of the relationship between CAD phenotypes and the changes of MBF.9)10) Additional coronary CT images may help delineate the myocardium affected by a specific epicardial coronary lesion and evaluate the perfusion decrease in a lesion-specific manner. However, recent studies have failed to improve the diagnostic accuracy of PET-measured MBF parameters using hybrid PET/CT images.8)11) They reassigned vascular territories in > 50% of the analyzed cases, but the reassignment did not lead to better diagnostic accuracy of hyperemic MBF. This might be attributed to the MBF quantification method used (vessel-specific MBF), which measures the MBF in a certain vascular territory as a whole, regardless of the lesion location.
Therefore, the present study assessed whether a more specific correlation of lesion location (proximal, mid, distal, or other small branches) using hybrid PET/CT imaging could improve the diagnostic accuracy of MBF parameters regarding anatomically significant left anterior descending artery (LAD) stenosis.
Go to : 
METHODS
Study population
Consecutive patients with stable angina referred to invasive coronary angiography (CAG) prospectively underwent N-13 ammonia PET and coronary CT before CAG for study purposes, all of which were performed within two weeks. The exclusion criteria included acute coronary syndrome, previous revascularization or myocardial infarction, overt heart failure with a decreased left ventricular ejection fraction (< 40%), changes in the clinical presentation between any two of the studies, a coronary anomaly, other structural heart diseases, or allergies to the contrast medium. Patients with a left main branch stenoses and those with data errors in the image fusion processes were also excluded. Forty-three patients were finally included and their baseline characteristics are listed in Table 1. The recruitment of the patients, acquisition and analysis of the imaging studies, and clinical data collection were approved by the Institutional Review Board (IRB) of Chonnam National University Hospital [IRB No. CNUH-2016-195].
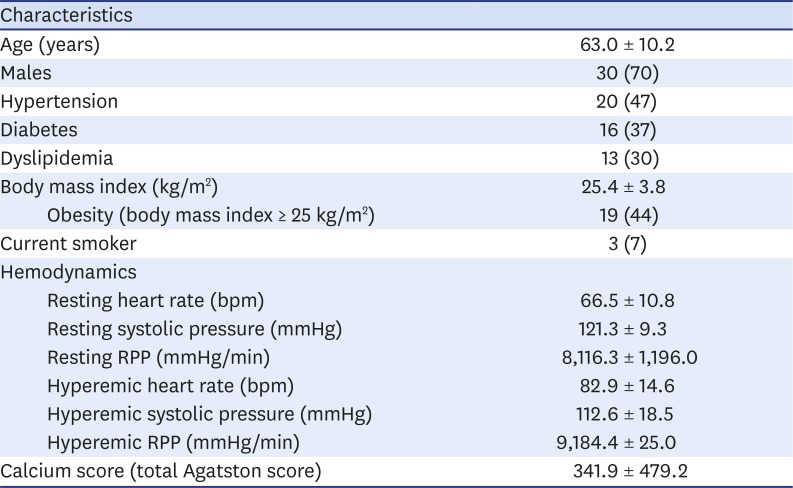
Table 1
Baseline characteristics of the study population
Data are the mean ± SD or n followed by percentage in parentheses.
CAD: coronary artery disease, RPP: rate-pressure product (systolic blood pressure × heart rate).
![]()
N-13 ammonia PET
The N-13 ammonia PET was performed in accordance with the current guidelines for myocardial perfusion PET.12) The patients fasted for ≥ 4 hours and nitrate, beta blockers, calcium channel blockers, methylxanthine derivatives, and caffeine were not consumed ≥ 24 hours before PET acquisition.
Patients were positioned on the scanner with their arms raised. Intravenous lines were placed in the patient's radial veins for N-13 ammonia injection and adenosine infusion. First, a low-dose CT scan (120 kV, 30 mA) for attenuation correction was performed. A bolus (11 MBq/kg [0.3 mCi/kg]) of N-13 ammonia was injected and the dynamic image acquisition was started simultaneously and lasted for six minutes. Immediately following the dynamic image acquisition, electrocardiogram (ECG)-gated static image acquisition was initiated and lasted 13 minutes. The infusion of adenosine was performed at a rate of 0.14 mg/kg/min for six minutes, one hour after the resting image acquisition was completed. N-13 ammonia was injected after three minutes during the peak hyperemia. Stress image acquisition was started simultaneously with the N-13 ammonia injection using the same time frames as the resting images. Image acquisition was performed using a dedicated PET scanner (Discovery ST, GE Healthcare, Chicago, IL, USA). The images were reconstructed using ordered subset expectation maximization with two iterations.
Coronary CT
One to two hours prior to the coronary CT scan, patients with a heart rate over 65 were administered p.o. beta blocker medication (propranolol 40 mg, maximum 120 mg).
A 2nd-generation dual-source CT scanner (SOMATOM Definition Flash; Siemens Medical Solution, Munich, Germany) was used while applying the previously described protocol.10) The section thickness was 0.75 mm, the gantry rotation time was 0.33 s, the tube current was 600 mAs at 120 kVp, and the pitch was 0.2 (conventional mode) or 3.4 (high-pitch mode). ECG gating was performed either retrospectively (conventional mode) or prospectively (high-pitch or step-and-shoot mode), according to the patient's heart rate variability.
The CT scan range included the entire heart. A non-ionic contrast medium (Ultravist 370; Bayer Schering Pharma, Berlin, Germany) was injected as a bolus, followed by a 60 mL saline flush at a speed of 4 mL/s for clearance of the contrast medium. The axial images were reconstructed at multiple phases covering the cardiac cycle in increments of 10% of the RR interval between 5% and 95%. Short-axis slices were reconstructed from the base to the apex using the Argus software tool (Siemens Medical Solution).
Hybrid imaging of N-13 ammonia PET and coronary CT
The PET and CT images were fused using a commercially available software tool (CardIQ Fusion, GE Healthcare). The images were appropriately co-registered in the transaxial, coronal, and sagittal planes according to anatomical landmarks, such as the interventricular septum, cardiac apex, and papillary muscles. The epicardial surface was automatically extracted and manually modified using a seed and extend algorithm. The non-gated perfusion images were projected onto the myocardial surface using a rainbow color scale. The coronary trees were traced using the same algorithm as that used in the myocardial extraction. The perfusion-rendered myocardium and the extracted coronary trees were fused with the same axis orientation. The image fusion was performed using the Advantage Workstation 4.6 (GE Healthcare).
Conventional and lesion-specific MBF measurement
The analyses were performed only for the LAD as its path was invariably located along the anterior aspect of the interventricular septum with the least ‘floating segments’ among the three major coronary branches.
Conventional MBF measurements were performed using the PMOD (PMOD Technologies, Zurich, Switzerland) software package, as previously described.10) The hyperemic and resting MBF was calculated for the standard 17 myocardial segments. The territory of the LAD included the apical, apical septal, apical anterior, mid-anterior, mid-anteroseptal, basal anterior, and basal anteroseptal segments.13) The MFR was calculated by dividing the hyperemic MBF with the correlating resting MBF.
Two cardiac imaging experts analyzed the coronary CT images to assess the presence and location of LAD stenosis. Any stenosis (≥ 30%)14) on the CT images was considered eligible for lesion-specific MBF measurement and its location was classified as proximal, mid-, distal LAD, and diagonal branches, as previously suggested.15) The hybrid PET/CT images were aligned to the same axis as that of the polar plot MBF maps from the PMOD software. According to the vascular path and the location of a certain stenosis, the downstream myocardial segments were isolated by the consensus of two observers. The lesion-specific MBF was defined as the average MBF value calculated within the isolated myocardial segments (Figure 1).
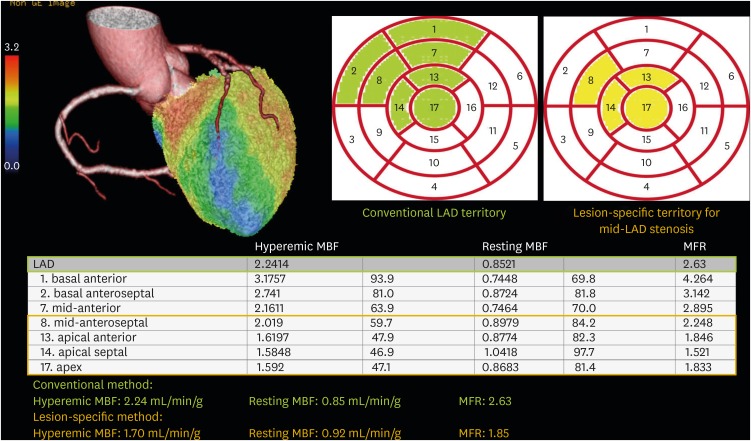 | Figure 1Conventional and lesion-specific measurements of the MBF and MFR in a patient with a significant mid-LAD stenosis (89% reference diameter). For a lesion-specific MBF measurement, the segments downstream of the mid-LAD stenosis (segments 8, 13, 14, and 17) were isolated and their average MBF values were obtained. LAD: left anterior descending artery, MBF: myocardial blood flow, MFR: myocardial flow reserve.
|
Radiation exposure from hybrid PET/CT imaging
The total radiation exposure of a patient undergoing hybrid PET/CT imaging was calculated by summing the effective doses from the N-13 ammonia PET and coronary CT studies, respectively. The effective dose from N-13 ammonia PET was calculated by multiplying the estimated effective dose (0.002 mSv/MBq) suggested by the International Commission on Radiological Protection Publication 8016) with the actual administered dose (produced N-13 activity – post-injection activity in the syringe). The effective doses from rest and stress studies were summed to obtain the total radiation exposure from N-13 ammonia PET. For calculating the effective dose from coronary CT, the dose-length product was obtained from the CT dose report and multiplied by a conversion coefficient value of 0.014 mSv·mGy−1cm−1.17) The effective dose from the low-dose attenuation correction CT was calculated using the same method as that of cardiac CT with a conversion coefficient value of 0.014 mSv·mGy−1cm−1.18) This value was regarded to be a part of the effective dose from N-13 ammonia PET.
Statistical analyses
The hyperemic MBF, resting MBF, and MFR values were compared between the LADs with and without significant stenosis (≥ 70% reference diameter on CAG)19) using the student's t-test. To evaluate the changes of the MBF values by applying the lesion-specific method, the MBF values measured by the two different methods were compared using the paired t-test.
The diagnostic performances were compared between conventional and lesion-specific measurements. The sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), and accuracy with 95% confidence intervals were calculated for the two methods, based on the binary discrimination of either the presence or absence of significant stenosis. Receiver operating characteristics (ROC) curve analysis was performed to obtain the optimal cutoff values for the calculation of diagnostic performances. The areas under the ROC curves (accuracy) were compared using the methodology suggested by DeLong et al.20) Pearson's correlation analysis was applied to elucidate the relationships between the MBF values measured by the two different methods and anatomical stenosis severity.
The statistical analyses were performed using IBM SPSS Statistics for Windows, ver. 23.0 (IBM Corp., Armonk, NY, USA) and MedCalc ver. 11.6.1.0 (MedCalc Software bvba, USA). A p-value < 0.05 was considered as statistically significant.
Go to :
RESULTS
Twenty-eight patients (64%) were eligible for lesion-specific MBF measurement and the measurements were successfully performed for all of them. Nineteen (44%) had significant LAD stenoses. The significant stenoses were located in the proximal LAD (n = 5), mid-LAD (n = 10), proximal-to-mid-LAD (n = 3), and the diagonal branch (n = 1). No patients had significant stenosis in the distal LAD. The myocardial segments downstream of the proximal lesion were included for lesion-specific MBF measurement in those with proximal to mid-LAD stenoses.
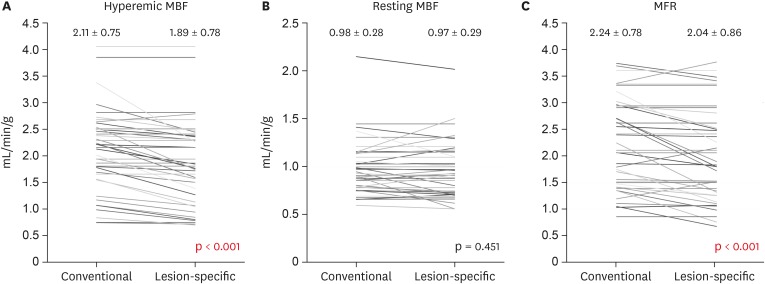
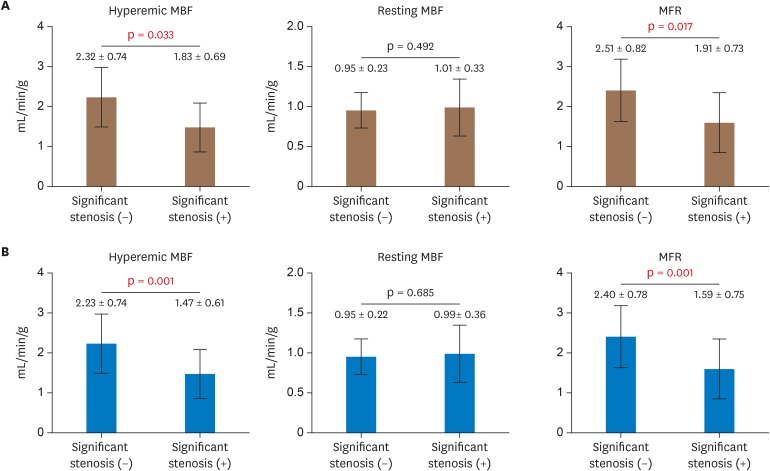
The hyperemic MBF and MFR measured using the lesion-specific method were significantly lower than those measured using the conventional method while the resting MBF was similar between the two methods (Figure 2). The hyperemic MBF and MFR were significantly lower in the LADs with significant stenosis for both the conventional and lesion-specific measurements, while no difference of the resting MBF was found (Figure 3).
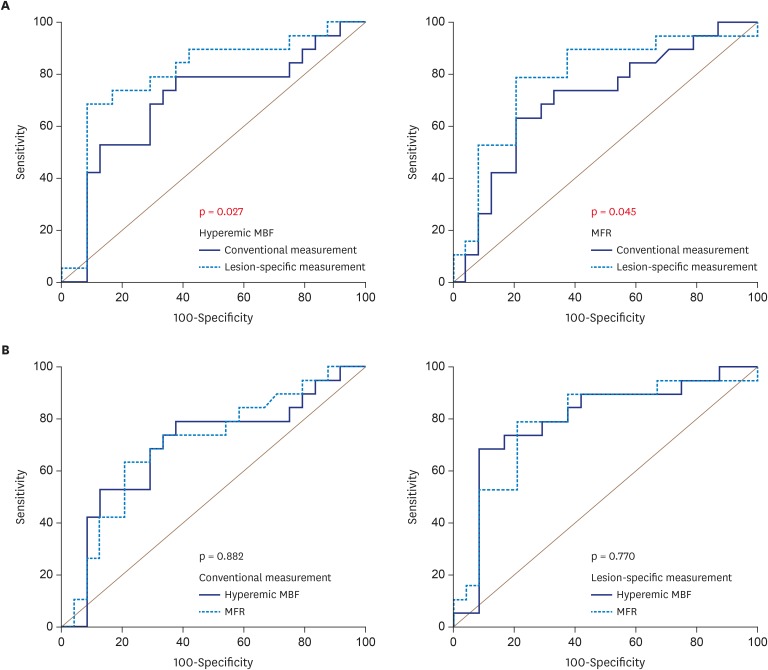
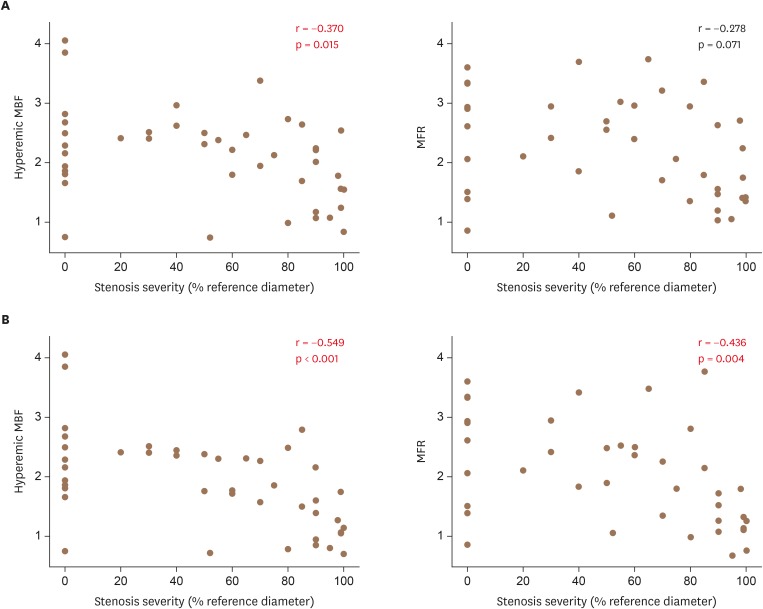
For the conventional method, the sensitivity, specificity, NPV, PPV, and accuracy were 71%, 68%, 74%, 65%, and 70% for the hyperemic MBF (optimal cutoff = 2.15 mL/min/g) and 79%, 63%, 74%, 65%, and 70% for the MFR (optimal cutoff = 1.82), respectively. For the lesion-specific method, the sensitivity, specificity, NPV, PPV, and accuracy were 83%, 74%, 80%, 78%, and 80% for the hyperemic MBF (optimal cutoff = 1.75 mL/min/g) and 79%, 79%, 83%, 75%, and 79% for the MFR (optimal cutoff = 1.86), respectively. The overall diagnostic accuracy was significantly higher with the lesion-specific method for both the hyperemic MBF and MFR. However, no statistical differences were found between the diagnostic accuracy of the hyperemic MBF and MFR when the same method was applied (Figure 4). The resting MBF could not effectively detect significant LAD stenosis using either of the two methods. The hyperemic MBF and MFR measured by the lesion-specific method correlated better with anatomical stenosis severity than those measured by the conventional method (Figure 5).
The mean effective dose from hybrid PET/CT imaging was 9.15 ± 5.48 mSv. The mean effective dose from N-13 ammonia PET was 1.94 ± 0.12 mSv while that from cardiac CT was 7.21 ± 5.45 mSv. However, the highest effective dose reached 20.9 mSv in a patient imaged in the conventional mode.
Go to :
DISCUSSION
The present study assessed MBF measurements using hybrid PET/CT imaging. The lesion-specific method significantly improved the diagnostic accuracy of PET-measured MBF parameters compared to the conventional method. The lesion-specific hyperemic MBF and MFR were better correlated with the anatomical severity of LAD stenosis than conventional methods.
The anatomy of the coronary trees varied among individuals and the 17 segment model has substantial discrepancies with actual coronary territories.21) These facts seriously limit the clinical relevance of MBF parameters derived from myocardial perfusion PET. Two recent studies attempted to solve these problems by reassigning vascular territories using hybrid PET/CT.8)11) However, although 50% of the standard myocardial segments were reassigned to new territories, they failed to improve the diagnostic accuracy of the hyperemic MBF regarding anatomically and functionally significant stenoses. In those studies, the hyperemic MBF values were averaged throughout the whole territory, regardless of the lesion locations so that only small changes were observed after territory reassignment. In contrast, the hyperemic MBF and MFR values could significantly decrease if the lesion locations were taken into account, as shown in the present study. It can be assumed that a whole territory-based, ‘per-vessel’ approach may dilute the significance of coronary stenosis. Some normally perfused segments, which are not subtended to the stenosis, might falsely increase the hyperemic MBF and lower its diagnostic performance. The MBF parameters calculated only within the downstream segments could more directly reflect the severity of myocardial ischemia.
There have been several attempts to measure MBF in a lesion-specific manner using hybrid PET/CT imaging. Kim et al.22) traced the MBF change by manually drawing ellipsoidal regions of interest along the interventricular septum on PET images. The results showed that the MBF gradient reflected the location (proximal vs. mid-to-distal) of the LAD stenosis. Piccinelli et al.23) introduced a more advanced technique of tracking the vascular path and its MBF changes along the coronary arteries. They established normal ranges for vessel-specific MBF values from subjects without angiographic stenoses. Without additional anatomical information from CT, Lee et al.2) analyzed only the segments with visually appreciable perfusion defects to enhance the lesion specificity of the MBF parameters. The main limitation of such a method is that visual estimation of the extent of perfusion defects can be influenced by threshold and image contrasts. Notably, recent coronary CT studies have suggested automated delineation of individualized coronary territories named fractional myocardial mass (FMM), which is completely independent of the standardized 17 myocardial segment model.24)25) A larger FMM relative to the coronary luminal area was associated with lower fractional flow reserve (FFR) values,26) which is plausible since FFR reflects not only the severity of epicardial coronary stenosis but also the myocardial mass subtended to a specific coronary segment. Taking advantage of hybrid PET/CT imaging, the amount of actual flow normalized to the subtended myocardium (‘FMM-specific MBF’) may be available, providing comprehensive insight into the coronary physiology among the pressure, flow, and myocardial mass.
There are concerns that hybrid PET/CT imaging may be redundant in the non-invasive assessment of CAD and that coronary CT itself may be sufficient. As FFR measured by CT has become clinically available, coronary CT has gained relevance in both the anatomical and functional assessments of epicardial CAD.27) However, a patient's prognosis depends not only on the severity of epicardial stenosis, but also on hemodynamic impairments caused by diffuse atherosclerosis or microvascular disease. FFR may overlook significant epicardial stenosis in the presence of microvascular dysfunction, which blunts the vasodilatory response to pharmacologic stress.28) Therefore, there is still a great need for measuring flow that can be obtained by PET. Myocardial perfusion PET and coronary CT can play complementary roles through their respective genuine abilities, leading to synergistic and comprehensive evaluations of various aspects of CAD.
There are several limitations of the present study. First, the sample size was small and the physiological stenosis severity (such as FFR) was not assessed. Second, actual clinical application of the lesion-specific MBF measurement may be limited in the case of the left main stem, left circumflex, or right coronary artery stenoses because they have substantial floating segments, which do not directly correlate with certain myocardial areas. Third, we did not optimize the coronary CT protocol in order to reduce radiation exposure in this hybrid imaging study. Although the mean total effective dose was under 10 mSv, which is comparable to recent data29) and similar to or lower than that from SPECT using Tc-99m-labeled agents and conventional cameras,30) the highest value obtained was > 20 mSv. This implies that the coronary CT protocol should be optimized for the balance between the diagnostic gain from hybrid imaging and radiation risk. Lastly, albeit significantly improved, the diagnostic accuracy of lesion-specific hyperemic MBF and MFR was slightly lower than that of the vessel-specific hyperemic MBF assessed in recent studies.8)11) Regarding the fact that the prevalence of diabetes was more than double in our study (37% vs. 16%), underlying microvascular disease might have negatively influenced the diagnostic accuracy regarding epicardial stenosis. Additionally, the calcium scores were substantially high in our study population, which might have decreased the MFR even in the absence of significant epicardial stenosis.10)
Conclusions
Lesion-specific measurement using hybrid imaging of myocardial perfusion PET and coronary CT improved the diagnostic accuracy of PET-measured hyperemic MBF and MFR. This technique may overcome the shortcomings of the current MBF measurement by PET and help to diagnose and manage CAD in the clinical field.
Go to :
 XML Download
XML Download