

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Neutropenic enterocolitis is a fatal enterocolitis occurring in neutropenic patients with immunocompromised diseases, such as hematologic malignancies, history of solid organ or hematopoietic stem cell transplantation, and acquired immunodeficiency syndrome [1]. It mainly involves the terminal ileum, cecum, and ascending colon. Various organisms including Gram-negative bacilli, Gram-positive cocci, anaerobes, and Candida species are often identified alone or in combination [23].
Mucormycosis is a rare, life-threatening, opportunistic fungal infection caused by fungi in the order Mucorales. Mucormycosis occurs mainly in people with hematologic malignancies, diabetic ketoacidosis, renal or heart failure, history of solid organ or hematopoietic stem cell transplantation receiving immunosuppressive agents, and deferoxamine therapy, and in those who are malnourished [4567]. The mortality rate of mucormycosis approaches 70% [8]. The most common site of mucormycosis is rhinocerebral involvement following pulmonary, cutaneous, gastrointestinal (GI) involvement, and disseminated disease [47]. GI mucormycosis accounts for only 2% to 11% of all mucormycosis involvement, but the mortality rate is about 85% to 95% [910]. Mucormycosis is more common in patients with acute leukemia than other hematologic malignancies, such as myelodysplastic syndrome (MDS) and lymphoma [8].
We report a case of neutropenic enterocolitis due to mucormycosis in a patient with MDS who was successfully treated with surgery and liposomal amphotericin B.
Case Report
A 33-year-old man received first decitabine chemotherapy for MDS, refractory anemia with excess blast type 1. He had received itraconazole (100 mg twice a day) for prophylaxis. Two weeks later, he visited the emergency room because of fever. On examination, vital signs were blood pressure 100/60 mmHg, temperature 36.9°C, heart rate 144/min, and respiratory rate 16/min. White blood cell (WBC) count was 1,030/mm3 with 31% neutrophils, hemoglobin 7.0 g/dL, platelet count 3,000/mm3, total bilirubin 2.11 mg/dL, and C-reactive protein level 3.33 mg/dL. Serum galactomannan antigen was negative. An abdominal radiograph showed mild non-specific paralytic ileus, but there was no pain and tenderness on any abdominal point. There were no abnormal findings on chest radiograph and urinalysis. He received granulocyte colony-stimulating factor (G-CSF), piperacillin/sulbactam (4.5 g four times a day), and amikacin (7.5 mg/kg twice a day) for febrile neutropenia (Fig. 1). On hospital day 9 (chemotherapy day 27), he complained of whole abdominal cramping pain. There was tenderness as well as rebound tenderness on the whole abdomen. On examination, vital signs were blood pressure 120/80 mmHg, temperature 37.8°C, heart rate 90/min, and respiratory rate 20/min. WBC count was 420/mm3 with 4.7% neutrophils. Computed tomography (CT) of the abdomen revealed abnormal wall thickening and decreased density of the ileocecal valve and terminal ileum, suggesting neutropenic enterocolitis (Fig. 2). Supportive treatment including nasogastric tube drainage, G-CSF, ceftazidime (2 g three times a day), and ciprofloxacin (400 mg twice a day) was started due to neutropenia (WBC count 420/mm3) and thrombocytopenia (platelet count 3,000/mm3) (Fig. 1). Patient was broadened the spectrum of antimicrobial agents to meropenem (1 g three times a day) and metronidazole (500 mg three times a day), and an antifungal agent (caspofungin, 50 mg once daily) (Fig. 1). Symptoms and signs including fever, abdominal pain, and tenderness on the whole abdomen did not improve. Another abdominal CT scan was done on hospital day 18, which revealed bowel perforation at ileocecal valve and terminal ileum with partial obstruction of bowel and peritonitis (Fig. 3). Emergent exploratory laparotomy was performed. Gross finding showed whole small bowel dilatation, ileocecal region perforation, and ascending colon inflammation. Small bowel resection at ileocecal lesion was performed. After surgery, the patient received G-CSF, meropenem, levofloxacin (750 mg once daily), and caspofungin until the biopsy was confirmed (Fig. 1). Microscopic finding showed hemorrhagic infarction associated with invasive fungal infection with right angle hyphae corresponding with mucormycosis (Fig. 4). After the histopathologic confirmation, caspofungin was switched to liposomal amphotericin B (5 mg/kg/day) (Fig. 1). On hospital day 21, he still complained of whole abdominal pain, although fever and the inflammation marker were resolved and neutrophil counts had recovered. A second follow-up abdominal CT scan performed on hospital day 21 showed bowel perforation, gangrenous change at ileocecal valve, terminal ileum, and multifocal complicated fluid collection in the peritoneum due to sealed-off perforation (Fig. 5). Galactomanan or 1,3-beta-D glucan level was not examined that day. On hospital day 26, exploratory laparotomy was performed again, which revealed perforation of the previous anastomosis site. Segmentectomy of the small bowel perforation, mobilization of ascending colon, and ascending colon transection were performed. Microscopic histopathologic findings showed hemorrhagic infarction and fungal hyphae at resected small bowel and resected ascending colon (Fig. 6). He received liposomal amphotericin B for 6 weeks and was finally discharged from hospital with full recovery of general condition. Another abdominal CT scan confirmed the absence of perforation.
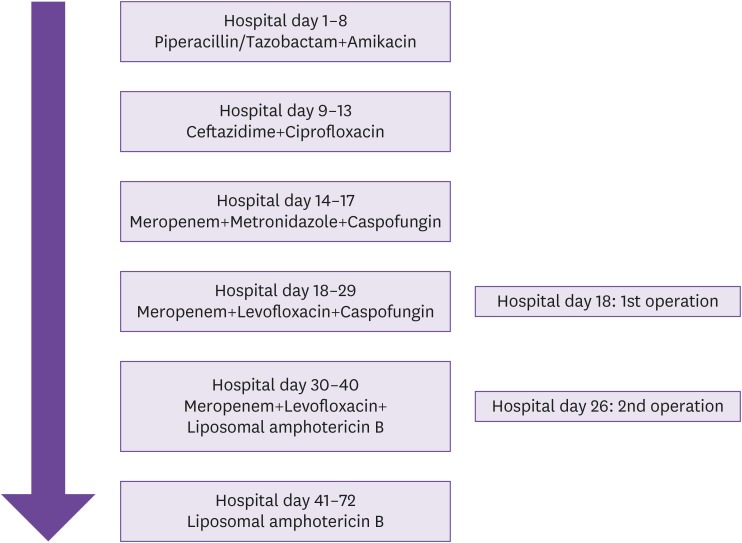
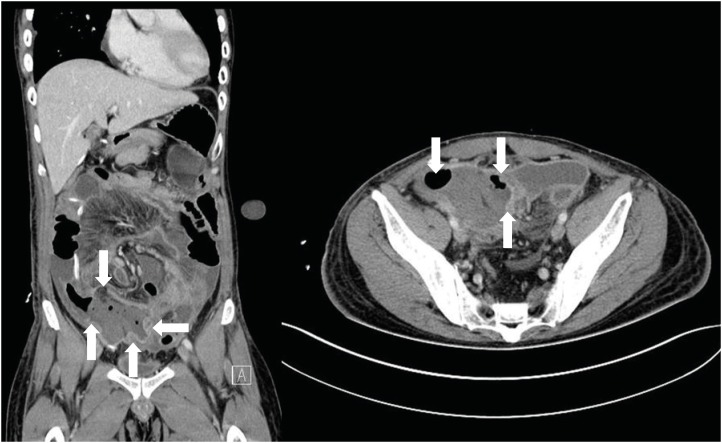
Figure 2
Abnormal wall thickening and decreased density of the ileocecal valve and terminal ileum, suggesting necrotizing enterocolitis (white arrows).
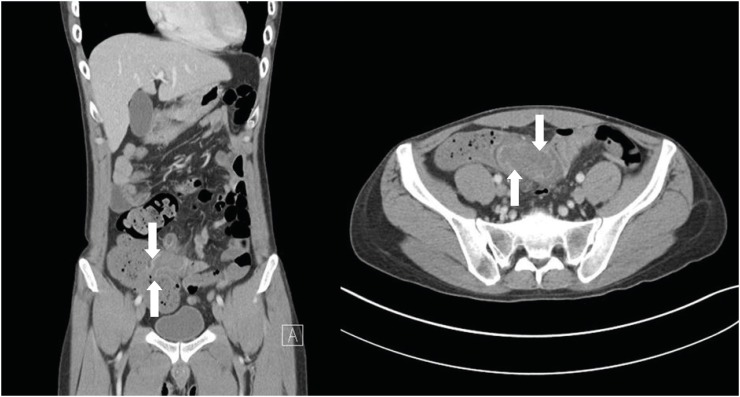
Figure 3
Perforation of the ileocecal valve (white arrows), terminal ileum with partial obstruction, and peritonitis.
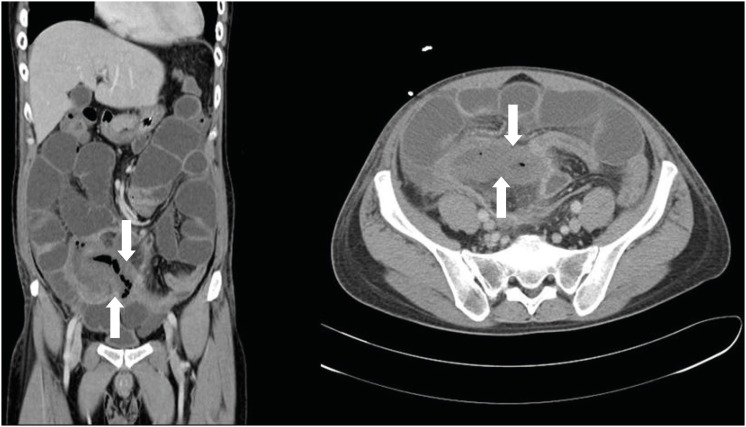
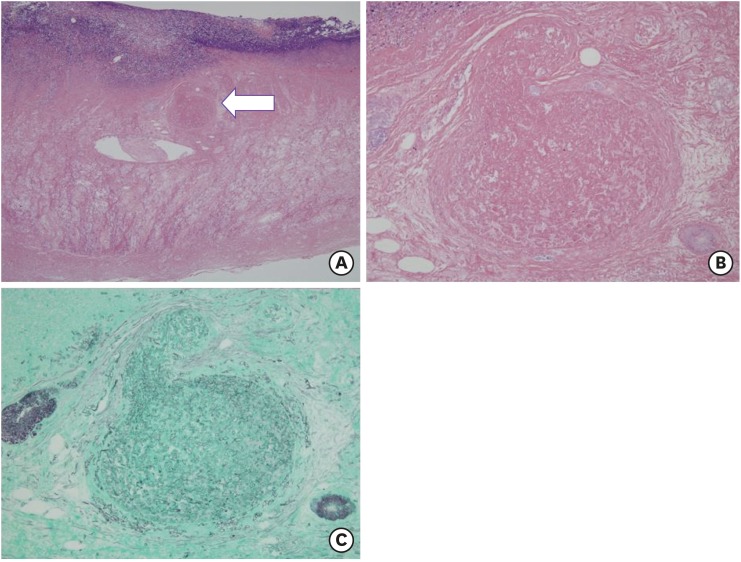
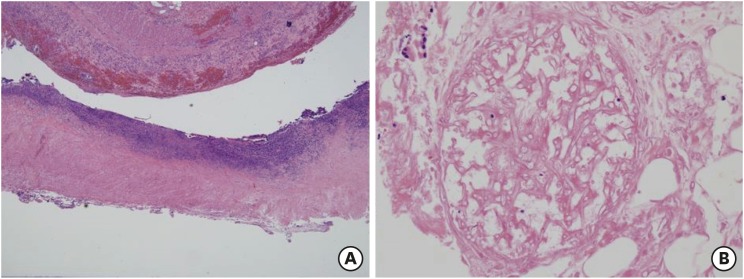
Figure 4
Histological observations. (A) Microscopically extensive coagulative infarction of intestine was noticed and angioinvasion (arrow head) in the muscularis propria was identified (H&E, ×40). (B) Fungal hyphae were admixed with fibrinous material in the vascular lumen occluding the vasculature, which is referred to angioinvasion (H&E, ×200). (C) GMS staining demonstrated non-septated broad hyphae with right-angled branching, suggestive of invasive mucormycosis (GMS, ×200).
H&E, hematoxylin and eosin; GMS, Gomori's methenamine silver.
Discussion
We report a case of GI mucormycosis manifesting as neutropenic enterocolitis in a patient with MDS. To our knowledge, this is the first case report of GI mucormycosis in a MDS patient. This case involved the ileocecal region and ascending colon. GI mucormycosis needed to be confirmed by pathologic examinations of surgical specimens, since the patient had symptoms and signs consistent with necrotizing (neutropenic) enterocolitis and there was no evidence supporting a suspicion of mucormycosis. A galactomannan assay was done on hospital day 1 and 13, and follow-up blood cultures were done many times, however, all were negative. Symptoms and signs of neutropenic enterocolitis include fever, abdominal distension, pain, tenderness, nausea, vomiting, watery or bloody diarrhea, and paralytic ileus. In patients with these symptoms, the many differential diagnoses include graft-versus-host disease, cytomegalovirus colitis, diverticulitis, appendicitis, inflammatory bowel disease, pseudomembranous colitis, ischemic colitis, Ogilvie's syndrome, cholangitis, and cholecystitis. In patients without complications (peritonitis, bleeding, or perforation), nonsurgical management with bowel rest, nasogastric decompression, hydration, nutritional support, correction of electrolyte imbalance, transfusion, broad spectrum antibiotics, empirical antifungal therapy, and G-CSF are optional. Although surgery is generally not recommended, it is indicated in patients with perforation, bleeding, or peritonitis [111].
GI mucormycosis is rare, even in patients with hematologic malignancies. The stomach is the most common organ of involvement followed by the colon. The small bowel is the least-involved organ in GI mucormycosis [46712]. The clinical symptoms of GI mucormycosis are varied and non-specific, and include abdominal pain and distension, fever, nausea and vomiting, diarrhea, hematemesis, and hematochezia. These non-specific symptoms can interfere with early diagnosis and treatment of mucormycosis. Galactomannan antigen test is not helpful for diagnosis of mucormycosis, one of the most common non-Aspergillus invasive fungal infections. On the other hand, imaging of GI mucormycosis is not specific for invasive fungal infection. Blood and urine cultures are also not helpful for diagnosis of GI mucormycosis. Therefore, it is almost impossible to discriminate mucormycosis from other bacterial or fungal infections without histopathological confirmation. Aspergillosis and mucormycosis can be confused based just on histopathological examination. Therefore, we should consider microbiologic culture in addition to histopathological confirmation. In this case, however, we did not culture surgical specimens for fungi. The characteristics of histopathologically identified fungal pathogens are wide, non-septate, irregularly branching hyphae with blood vessel invasion and tissue necrosis [1213141516171819]. Our findings indicate that clinicians should consider the possibility of GI mucormycosis in patients being treated for hematologic malignancy along with typhilitis or necrotizing enterocolitis. Our patient received two surgeries and liposomal amphotericin B simultaneously. The principles of treatment for mucormycosis are early detection, correction of predisposing factors, surgical debridement of infected tissues, and use of appropriate antifungal agents. Currently, amphotericin B and its liposomal preparation or lipid complex, which can reduce nephrotoxicity, are the recommended antifungal agents. Triazoles except for posaconazole and echinocandins are not effective against mucormycosis. However, recently triazoles and echinocandin have been preferred to amphotericin B for empirical treatment of neutropenic fever patients [6121314]. Therefore, clinicians should consider mucormycosis as one of possible diagnosis when a neutropenic patient does not respond to empirical antifungal treatment.
In summary, this case suggests that Gl mucormycosis can manifest as typhlitis or neutropenic enterocolitis, and emphasizes the importance of high suspicion, early diagnosis, and appropriate medical and surgical treatment for GI mucormycosis. It is difficult and dangerous to do invasive procedures for diagnosis, especially in patients with hematologic malignancies. For a neutropenic patient manifesting as typhlitis who does not respond to antibiotic treatment, GI mucormycosis can be considered, and an antifungal agent covering mucormycosis may be helpful.
 XML Download
XML Download