

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Staphylococcus aureus is one of the most common causes of bacteremia both in the community and hospitals. S. aureus bacteremia (SAB) can spread to any body site and result in serious complications such as endocarditis, osteomyelitis, pneumonia, and meningitis with 20 – 50% mortality [123].
Patients with chronic kidney disease (CKD) are vulnerable to SAB because of the repeated hospital exposure, the use of intravascular catheters, fluid overload, and the negative impact of the uremic state on the immune function [45]. Where there are many studies reported on the outcomes of SAB in patients with end stage renal disease undergoing hemodialysis, there are few studies on the outcome of SAB in patients with non-dialysis dependent CKD (ND-CKD) [678]. Therefore, we aimed to define the clinical characteristics of SAB, estimate the all-cause mortality following SAB, and identify risk factors for mortality in patients with CKD stratified by dialysis.
Materials and Methods
1. Patients and clinical data
We performed a retrospective study among patients who were hospitalized in Chungnam National University Hospital and developed SAB in the period of March 2014 to December 2018. All patients with signs and symptoms of bacteremia with positive blood cultures for S. aureus were included in this study. Only the first clinically significant episode of infection with SAB for each patient was included in the analysis. Cases of suspected contamination and polymicrobial bacteremia were excluded. The VITEK II automated system (bioMérieux Inc., Marcy L'Etoile, France) was used to identify bacterial organisms and to detect vancomycin minimum inhibitory concentration (MIC). In the VITEK II, system bacterial organisms are identified with standard identification cards.
Patients with SAB were identified from microbiology laboratory records. All detailed clinical data including baseline characteristics, Charlson's Comorbidity Index (CCI) score, severity of acute infection as measured by Pitt bacteremia score (PBS) and Sequential Organ Failure Assessment (SOFA) score, community or nosocomial acquisition of bacteremia, antimicrobial therapy, methicillin resistance of S. aureus isolates, and all-cause mortalities were collected from reviewing the electronic medical records.
The study protocol was reviewed and approved by an institutional review board (IRB) of the Chungnam National University Hospital (IRB registration no. 2019-10-026).
2. Definitions
Bacteremia was defined as the presence of ≥1 positive blood culture for S. aureus in a patient who had signs and symptoms consistent with Systemic Inflammatory Response Syndrome (SIRS). The diagnosis of SIRS was made according to the criteria of the Surviving sepsis campaign [9].
SAB was classified as community-acquired if S. aureus was isolated from blood cultures drawn within 48 h of hospital admission and was classified as healthcare associated if the patients had (1) a history of hospitalization or surgery in the previous year, (2) a history of residence in a long-term care facility in the past year, (3) a history of hemodialysis or peritoneal dialysis in the previous year, and (4) the presence of a permanent indwelling catheter or percutaneous medical device at the time of culture [10111213].
We defined patients with CKD as patients who had a GFR <60 mL/min/1.73 m2 for >3 months [14]. Patients who were at least 18 years of age and had no prior SAB episode at the time of CKD diagnosis were grouped as patients with CKD in the present study.
The infections were classified based on the primary site of infection as catheter-related bloodstream infection (CRBSI), heart and large vessel infection (including endocarditis, infected vascular thrombi, and infection of implanted vascular devices), bone and joint (including osteomyelitis and arthritis) infection, lung infection, skin and soft tissue infection, surgical site infection (SSI), central nervous system (CNS) infection, and unknown primary focus. CRBSI was considered to be the source of bacteremia, modified from the previous study. [15] Skin and soft tissue infection was considered to be the source of SAB when patients had a pure culture of S. aureus from a tissue or a drainage specimen from the affected site and had signs of infection [15]. SSI was defined according to the definitions of the Centers for Disease Control and Prevention [16]. If a primary focus of infection could not be determined, it was considered to be unknown.
The CCI is considered a reliable method for measuring comorbidity in clinical research. We collected comorbidities at diagnosis by review of the medical record within 12 months of diagnosis using methods previously described [17]. Severity of SAB was assessed using PBS and SOFA scores according to the methods previously described [1819].
We defined it appropriate if the at least 1 antibiotic to which the isolate showed in vitro susceptibility that was initiated within 2 days after the onset of SAB. Source control means removal of the intravascular catheter for CRBSI, percutaneous drainage or surgical removal of abscess if it presents, surgical removal of infected prosthetic device if it presents.
3. Statistical analyses
Bivariate analyses for categorical variables were performed using Pearson Chi square or Fisher's exact tests and one-way ANOVA test was performed to compare continuous variables. Kaplan-Meier estimates were plotted for patients with ND-CKD, dialysis, and non-CKD, and they were examined for differences by log-rank test. To investigate predictors of mortality following SAB, we used Cox proportional hazards regression models. SPSS software (version 22.0, SPSS, Inc., an IBM Company, Chicago, IL, USA) and Prism software (version 8, Graphpad, San Diego, CA, USA) were used for statistical analyses.
Results
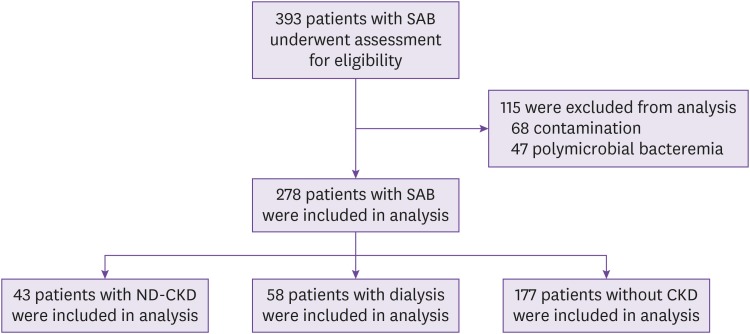
As a total, 278 SAB of 43 patients (31 males) with ND-CKD, 58 patients (39 males) with dialysis, and 177 patients (112 males) without CKD were analyzed after excluding 68 cases of suspected contamination and 47 of polymicrobial bacteremia in the period of March 2014 to December 2018 (Fig. 1).
Figure 1
Enrollment of patients with Staphylococcus aureus bacteremia (SAB).
ND-CKD, non-dialysis dependent chronic kidney disease; CKD, chronic kidney disease.
1. Clinical characteristics of the study population
The median (interquartile ranges) age of patients with SAB was 72 years (36 − 89) in ND-CKD, 65.5 years (34 − 90) in dialysis, and 68 (18 - 101) in non-CKD patients. Main demographic findings of the 278 patients are given in Table 1. Diabetes mellitus was most common among all patient groups. CCI was higher among dialysis (4.19 ± 1.95) and ND-CKD (4.14 ± 3.12), compared to non-CKD patients (3.01 ± 3.45, P = 0.013). All patients with dialysis in the present study were receiving hemodialysis.
Table 1
Baseline demographic and clinical characteristics of Staphylococcus aureus bacteremia (SAB)
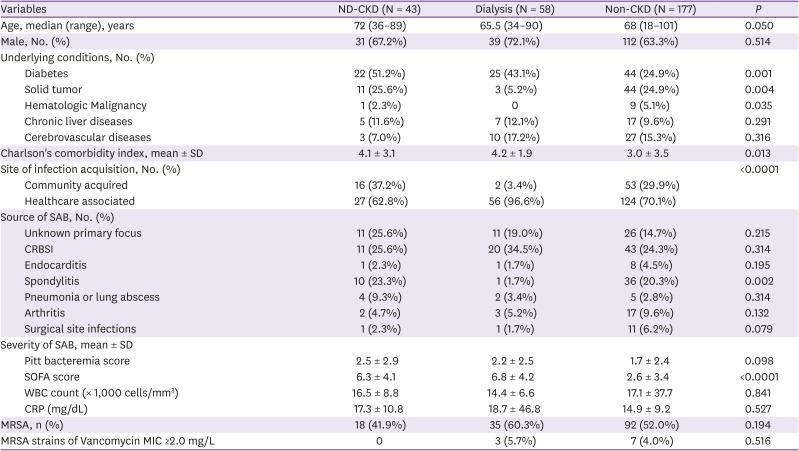
We found that SAB is healthcare-associated for 62.8% in ND-CKD, 96.6% in dialysis, and 70.1% in non-CKD group (P <0.0001). CRBSI was the most common source of SAB in all patient groups and especially comprises 34.5% among dialysis group. Unknown primary focus was more frequent in ND-CKD than in other groups, without statistical significance. ND-CKD and non-CKD had SAB originated from spondylitis and SSIs more frequently than dialysis patients did, which had no statistical significance.
PBS was increased in ND-CKD (2.51 ± 2.91) and dialysis (2.24 ± 2.47), compared to non-CKD (1.71 ± 2.35, P = 0.098) patients. SOFA score was significantly elevated in ND-CKD (6.26 ± 4.13) and dialysis (6.78 ± 4.21), compared to non-CKD (2.55 ± 3.44, P <0.0001) group.
The proportion of methicillin-resistant S. aureus (MRSA) was more than 50% in dialysis and non-CKD groups, and related with healthcare-associated SAB. In contrast, methicillin-susceptible S. aureus (MSSA) comprised 58% of SAB in ND-CKD patients. More than 90% of MRSA isolates in our study had vancomycin MIC ≤1.0 mg/L.
2. Appropriateness of treatment and outcome of SAB
For MSSA bacteremia (MSSAB), more than 90% of patients of all groups received antibiotics with anti-MSSA activity within 48 h after the onset of bacteremia (Table 2). However, the proportion of patients with MRSA bacteremia (MRSAB) who were given anti-MRSA antibiotics <48 h decreased to 38.3% of ND-CKD, 48.6% of dialysis, and 44.6% of non-CKD patients. Among 145 patients with MRSAB, 125 cases were initially treated with vancomycin and 14 cases didn't receive any anti-MRSA antibiotics because they died before the report of initial blood culture. The source of infection was controlled for 15 cases (34.9%) of ND-CKD, 30 cases (51.7%) of dialysis, and 79 cases (44.6%) of non-CKD patients.
Table 2
Treatment and outcome of Staphylococcus aureus bacteremia

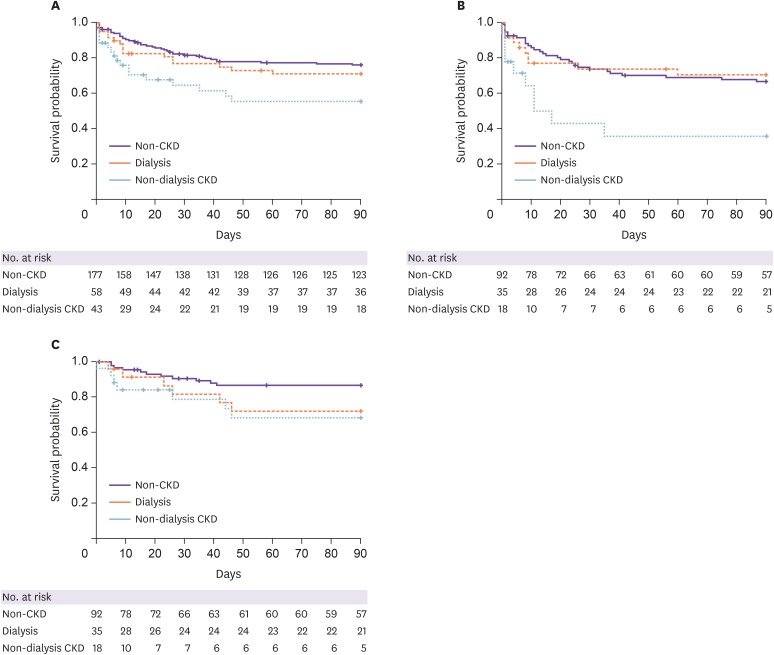
The 7-day all-cause mortality rate after a diagnosis of SAB was 25.6% among ND-CKD, 12.1% of dialysis, and 7.9% of non-CKD patients (P = 0.007). The 30-day mortality rate among ND-CKD was 39.5%, compared to 27.6% of dialysis and 20.9% of non-CKD patients (P = 0.037). The 90-day mortality was 46.5%, 32.8%, and 25.9% among ND-CKD, dialysis, and non-CKD patients, respectively (P = 0.065).
Kaplan-Meier survival estimates of the probability of survival from SAB plotted for ND-CKD, dialysis, and non-CKD patients are shown in Figure 2. ND-CKD showed higher risk for mortality (HR, 2.335; 95% confidence interval, 1.203 – 4.531; P = 0.003) compared to non-CKD patients in Log-rank test. The hazard ratio of all-cause mortality following SAB in ND-CKD compared to dialysis patients was 1.707 (95% CI, 0.895 – 3.258; P = 0.086). When the survival analyses were performed for patients stratified by methicillin resistance, the hazard ratio of mortality following MRSAB compared to MSSAB was 1.868 ((95% CI, 1.209 – 2.888; P = 0.0057) and the risk for all-cause mortality from MRSAB in ND-CKD significantly exceed that of dialysis (HR, 2.628; 95% CI, 1.074 – 6.435; P = 0.011) and that of non-CKD (HR, 3.001; 95% CI, 1.172 – 7.685; P = 0.0005) patients. The Kaplan-Meier survival estimates of survival probability following MSSAB was not different between ND-CKD and dialysis patients.
3. Risk factors associated with mortality
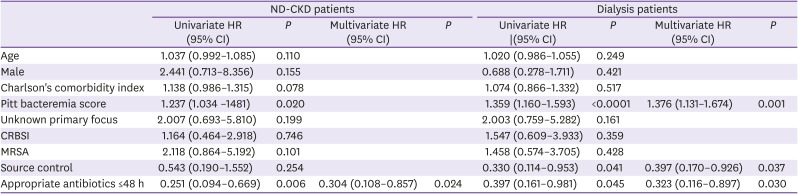
In a multivariate Cox regression model, appropriate antibiotics <48 h (adjusted HR, 0.304; 95% CI, 0.108 − 0.857; P = 0.024) was the only independent risk factor of mortality following SAB among patients with ND-CKD (Table 3). For dialysis patients, PBS (adjusted HR, 1.376; 95% CI, 1.131 − 1.674; P = 0.001), source control (adjusted HR, 0. 352; 95% CI, 0.126 − 0.985; P = 0.047), and appropriate antibiotics within 48 h (adjusted HR, 0. 323; 95% CI, 0.116 − 0.897; P = 0.030) were significantly associated with mortality following SAB.
Table 3
Hazard ratios for mortality of SAB in patients with non-dialysis dependent chronic kidney disease (ND-CKD) versus dialysisa
Discussion
This is the first study to estimate the all-cause mortality following SAB in CKD patients stratified by dialysis and its predictors in Korea. We found all-cause mortality, especially 7-day and 30-day mortalities, associated with SAB was significantly increased among ND-CKD patients. Administration of appropriate antibiotics <48 h could reduce the risk for mortality following SAB among CKD patients regardless of dialysis. The risk for mortality following MRSAB was significantly higher in ND-CKD, compared to dialysis or non-CKD patients.
SAB is a common, life-threatening infection with significant morbidity and mortality with 20 – 50% according to previous studies. [123] A recently performed prospective study in 11 Korean hospitals for 8 years showed 30-day case fatalities of 21.2 – 21.9% [20]. In the present study, overall 30-day mortality rate following SAB was 25.2% and Kaplan-Meier estimates showed that ND-CKD patients had increased risk for all-cause mortality compared to non-CKD patients. The 7-day all-cause mortality rate after a diagnosis of SAB was 26.8% among ND-CKD, which was significantly higher than that of dialysis patients (12.3%) or non-CKD patients (7.9%, P = 0.020). This higher early mortality with high PBS suggested that SAB among ND-CKD patients presented more severe manifestations at the onset that they died rapidly before the results of initial blood cultures were reported.
When the analyses were stratified by methicillin resistance, the all-cause mortality following MRSAB was significantly higher than that of MSSAB in our study. However, methicillin resistance was not a significant factor predicting mortality following SAB among CKD patients in a multivariate Cox proportional hazards regression. Many studies demonstrated conflicting results about the impact of methicillin resistance on the mortality of SAB [21222324]. A meta-analysis by Cosgrove et al. showed significantly higher mortality rates for MRSAB (OR, 1.93; 95% CI, 1.54 – 2.42; P <0.001) compared to that of MSSAB [24]. On the contrary, a prospective cohort study performed in Taiwan showed that patients with MRSAB did not have higher mortality than did patients with MSSAB, although most of the patients with MRSAB did not receive empirical glycopeptide therapy [23]. There have been no evidence to suggest that MRSA strains are more virulent than MSSA strains, however, failure in timely administration of appropriate empirical antibiotics, uncontrolled infection source, and inferior anti-staphylococcal activity of vancomycin could contribute to increased mortality following MRSAB.
Our study showed that receipt of appropriate antibiotics <48 h was significantly associated with reducing risk for mortality following SAB in ND-CKD and dialysis patients. Administration of inappropriate antibiotics was identified as an independent predictor for mortality in many studies, which also have conflicting data [2526]. In a retrospective cohort study performed in Israel, mortality was significantly higher among patients receiving inappropriate antibiotics than those receiving appropriate ones [25]. In contrast, inadequate empirical antimicrobial therapy for SAB was not associated with increased 30-day mortality rates in a study performed in 9 Western European countries [26]. Controversial results of the appropriateness of antibiotic treatment on the mortality of S. aureus infections may result from differences in methods and populations of studies. The proportion of methicillin resistance is different depending on the study sites and many studies evaluated outcomes in patients with staphylococcal infections from various sites with different severity including central venous catheter, skin and soft tissue, lungs, and bloodstream. This could result in significant clinical heterogeneity because mortality outcomes vary greatly between sites such as skin and soft tissue and pneumonia. Our study included only patients with SAB, which improved clinical homogeneity and made analysis more comparable. When the analysis of our study was stratified by methicillin resistance, appropriate antibiotics <48 h was associated with reducing mortality only in patients with MRSAB, not in those with MSSAB (data not shown). Since empirical treatment with glycopeptide has been largely restricted in our hospitals, inadequate antimicrobial treatment was strongly associated with MRSAB. Actually, the proportion of patients treated with appropriate antibiotics was significantly lower in patients with MRSAB (33.3 – 48.6%) than those with MSSAB (91.8 – 95.7%). Dialysis patients are more likely to be treated with vancomycin at the onset of fever before the report of microbiological results and to get easy approval for vancomycin use. This could explain why dialysis patients had better outcome following MRSAB, compared to ND-CKD patients in our study.
Source control have been reported to affect the outcomes of patients with SAB and this may be more important in determining mortality than the appropriateness of antibiotics. In a multicenter, prospective, observational study of 884 patients with SAB bacteremia duration was not affected by the choice of antibiotic therapy but by the time to source control procedure (P <0.0001), and delay in source control was significantly associated with increased 30-day mortality [27]. In addition, a retrospective cohort study demonstrated that failure of source control was an independent predictor of mortality, and in patients with eradicable foci, there were no significant differences in the mortality rate between appropriate and inappropriate empirical therapy [28]. Our study demonstrated that source control was related with reducing risk for mortality in dialysis patients. A randomized clinical trial could answer which of appropriate antibiotic treatment or source control is more important in determining the outcome of SAB, although this would be difficult to perform due to ethical issues.
We hypothesized dialysis could adversely affect the outcomes associated with SAB due to more deteriorated immune dysfunction; therefore, dialysis patients would have higher mortality than ND-CKD patients. However, the risk for mortality following SAB of dialysis patients was reduced compared to that of ND-CKD patients despite statistical insignificance, and their risk for mortality following MRSAB was significantly lower than that of ND-CKD patients. The reasons for improved survival in dialysis patients could be early diagnosis of SAB among these patients who visit the dialysis clinics regularly, easy access to vancomycin use, and the fact that dialysis catheter-related infections are the cause of SAB, which have a better prognosis due to immediate catheter removal.
There are several potential limitations of the present study that should be mentioned. First, the study was retrospective, a design which can make identifying the source of SAB difficult. In our study, the proportion of patients with unidentified primary focus was higher in ND-CKD (25.6%) patients despite no statistical significance. Since echocardiography was performed in only 1 case of unknown primary focus among ND-CKD patients, the incidence of endocarditis could be underestimated in this group. Second, vancomycin MICs vary depending on the testing methods.[29] Since we adopted the vancomycin MICs detected by VITEK II, the proportion of MRSA isolates with high vancomycin MIC (≥2.0 mg/L) could be underestimated. Therefore, we were not able to assess the impact of high vancomycin MIC on the mortality of our patients. Third, with the small number of cases with MRSAB in CKD patients, it was difficult to assess predictors for mortality using multivariate Cox-regression analysis in this group. A prospective study including increased number of cases with MRSAB needs to be performed to identify the risk factors for mortality in patients with CKD.
In conclusion, the risk for all-cause mortality following SAB was higher among ND-CKD, compared to non-CKD patients. Appropriate antibiotics <48 h was associated with reducing the risk for all-cause mortality following SAB among CKD patients, regardless of dialysis. For MRSAB, the risk for mortality among ND-CKD was significantly higher than that of dialysis or non-CKD patients.
 XML Download
XML Download