

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Gram-negative bacilli have become important pathogens in cancer patients [1], and Klebsiella pneumoniae (KP) is the second most common pathogen among Gram-negative bacteria [2]. A previous study revealed KP bacteremia tends to occur more frequently in cancer patients, and higher mortality was predicted in this population [3]. In addition, extended-spectrum beta-lactamase (ESBL) producers have increased and been considerable threat to clinicians, since they are often multidrug-resistant and may lead to poorer treatment outcome [4].
Given the pathogenic significance of ESBL-producing K. pneumoniae (ESBL-KP), knowing its characteristics and possible risk factors associated with worse clinical outcome may be helpful when treating cancer patients with Gram-negative bacteremia. Therefore, this study was performed to assess possible difference in characteristics and clinical outcome between ESBL-producing strains with non-ESBL-producers in adult patients with cancer.
Go to : 
Materials and methods
1. Study design
A retrospective cohort study was performed by reviewing the electronic medical record database at Samsung Medical Centre, a 1,960-bed tertiary care hospital with a comprehensive cancer center in Seoul, Korea. This study was approved by the Institutional Review Board of Samsung Medical Center (SMC 2011-10-095). Patients above the age of eighteen with cancer who had an episode of KP bacteremia between 2010 and 2012 were included in this study. Demographic information, medical history and laboratory data were collected by reviewing medical records. The study population was divided into two groups, based on whether or not the isolated strain produced ESBL. Clinical outcomes were measured by 14-day mortality, 30-day mortality, need for intensive care unit (ICU) care, occurrence of organ failure such as acute kidney injury, length of hospital stay and time to death.
2. Definition
Neutropenia was defined as an absolute neutrophil count of less than 500/mm3. Use of steroid was defined as exposure to doses greater than the equivalent of prednisolone 10 mg per day for more than three weeks within the previous one month [56]. Prior antibiotics exposure was defined as exposure to certain antibiotics within the 90 days prior to the onset of bacteremia. The definition of community-acquired and hospital-acquired (nosocomial) bacteremia followed previous definition [7]. The Pitt bacteremia score and Charlson score were used as defined previously [89]. The definition of acute kidney injury followed the Kidney Disease Improving Global Outcomes (KDIGO) guideline published in 2012 [10].
Pneumonia was defined as having respiratory symptoms, productive coughs for example, with new infiltrate on chest x-ray and with isolation of KP from lower respiratory tract specimens without another identifiable source. Pancreatobiliary infections were identified by symptoms, laboratory findings, or imaging studies. Patients with an intraabdominal focus other than pancreatobiliary tracts were classified as having intraabdominal infection. Patients without any identifiable source of infection were classified as primary bacteremia. The definition of catheter-related infection followed that of Infectious Diseases Society of America (IDSA) [11].
Empirical antimicrobial therapy was defined as the initial therapy before obtaining the results of blood cultures and definitive antimicrobial therapy was defined as therapy that might have been tailored according to the results of antibiotic susceptibility tests. Antibiotics therapy was considered appropriate if the treatment regimen included one or more antibiotic shown to be active in vitro in appropriate doses for the indicated use. Treatment failure was defined as persistence of fever or bacteremia, clinical deterioration, or death. The third-generation cephalosporins in the current study were exclusively ceftriaxone or cefotaxime.
3. Statistical analysis
Possible risk factors were first evaluated by Student's t-test or Mann-Whitney U test when comparing continuous variables, or by Fisher's exact test or chi-squared test for categorical variables. Associations that were found to be significant enough i.e. P <0.10 in univariate analysis were further analyzed by multivariate logistic regression with stepwise backward selection to identify independent risk factors. All P-values were 2-tailed, and P <0.05 was considered statistically significant. SPSS statistics, version 18.0 (IBM, Armonk, NY, USA) was used for analyses.
Go to :
Results
1. Baseline characteristics
A total of 278 cases of K. pneumoniae bacteremia in patients with cancer were identified during the study period. The mean age of the study population was 57.3 and patients with male gender comprised 59.7% of cases. Those with hematologic malignancy comprised 47.5% of cases. Of the study population, 28.4% had rapidly fatal disease by McCabe classification. In the 90 days prior to the onset of bacteremia, 219 patients (78.8% of cases) were exposed to certain antibiotics. ESBL-KP bacteremia was identified in 50 patients (18% of cases). Appropriate empirical antibiotics therapy was done in 88.5% of cases.
2. Clinical characteristics and outcome of ESBL-KP bacteremia compared to non-ESBL-KP
Differences in clinical characteristics and outcome between ESBL-KP and non-ESBL-KP bacteremia are presented in Table 1. Presence of a percutaneous drainage catheter [odds ratio (OR) 4.99, P <0.001], presence of a nasogastric tube (OR 5.05, P = 0.01), and surgery within 90 days (OR 2.78, P = 0.02) were more frequent in the ESBL group than in the non-ESBL group. Antibiotics such as third-generation cephalosporin (OR 2.14, P = 0.03), glycopeptide (OR 2.02, P = 0.04), metronidazole (OR 2.58, P = 0.005) were used more frequently in ESBL-producer group in the 90 days prior to the onset of bacteremia.
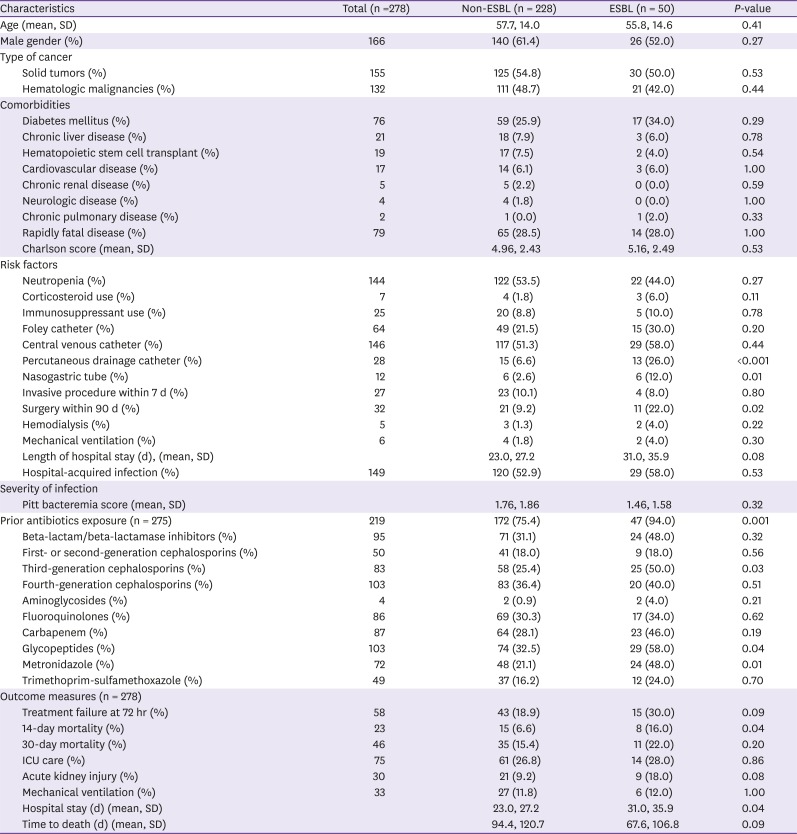
Table 1
Comparison of clinical characteristics and outcome of ESBL-producing and non-ESBL-producing Klebsiella pneumoniae bacteremia (n = 278)
![]()
Treatment failure during the initial 72 hours was more commonly seen in ESBL producer group, though not significantly (OR 1.84, P = 0.09). Although 14-day mortality was significantly higher with ESBL-KP bacteremia (OR 2.76, P = 0.04), there was no significant difference in 30-day mortality between non-ESBL producer group and ESBL producer group (OR 1.67, P = 0.20). Hospital stay was significantly longer in ESBL-KP bacteremia group (23.0 days in the non-ESBL group vs. 31.0 days in the ESBL group, P = 0.04), but no other measures of clinical outcome was significantly different between the two groups.
When adjusted for confounders by a multivariable regression model, the presence of percutaneous drainage catheter (OR 5.14, P = 0.001), prior exposure to a third generation cephalosporin (OR 2.22, P = 0.03) and prior exposure to a glycopeptide (OR 2.40, P = 0.02) were found more frequently in those with ESBL-KP bacteremia.
3. Risk factors for mortality and possible impact of ESBL on mortality
Possible risk factors for 30-day mortality and 14-day mortality are presented in Table 2 and Table 3. There was no significant difference according to age, gender, type of malignancy or type of underlying diseases. Among the risk factors examined previously, presence of a nasogastric tube (OR 3.73, P = 0.04), occurrence of organ failure severe enough to require mechanical ventilation (OR 10.43, P = 0.01) and hemodialysis (OR 7.64, P = 0.04) at the onset of bacteremia were found to be more frequent in the 30-day mortality group. Catheter-related infection was more frequently observed in mortality group (OR 3.67, P = 0.01). After adjusting for confounders, presence of a nasogastric tube and catheter-related infection were no longer significant. Goodness of fit measured by P-value of Hosmer-Lemeshow test was 0.553.
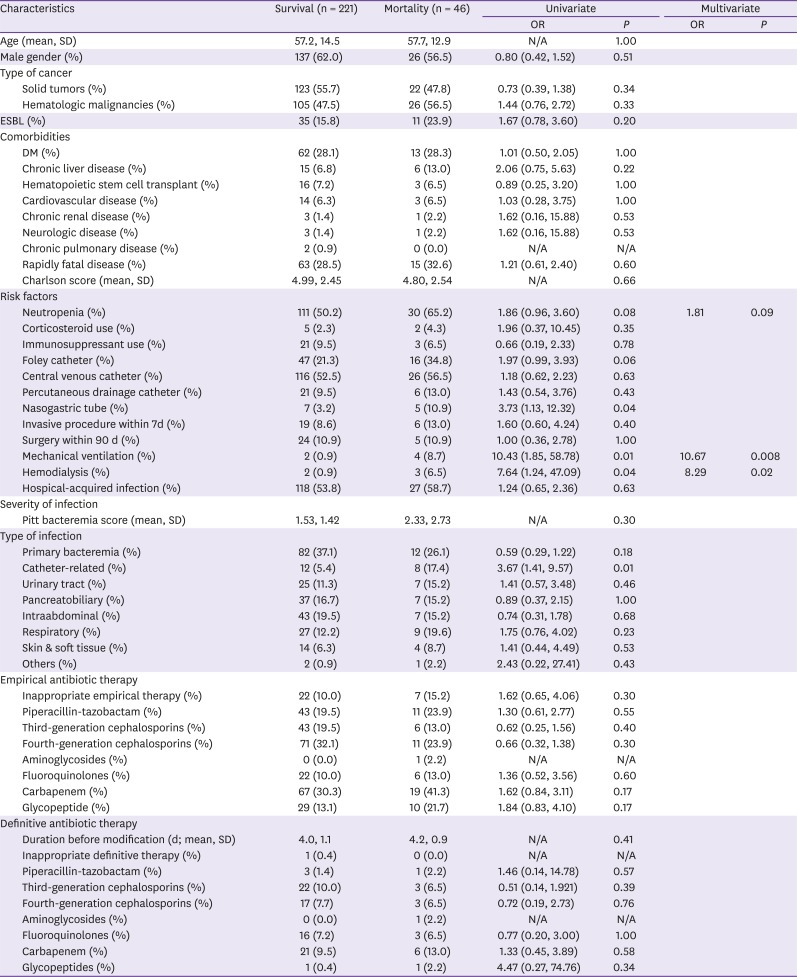
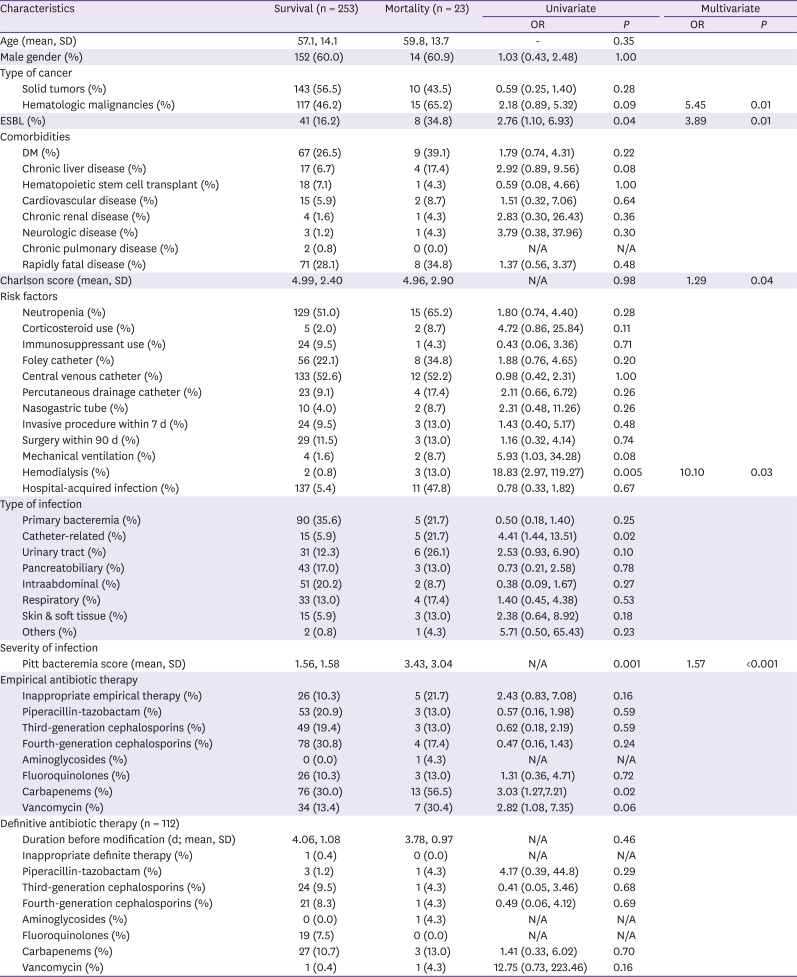
Table 2
Risk factors for 30-day mortality (n = 267)
OR, odds ratio; SD, standard deviation; N/A, not applicable; ESBL, extended-spectrum beta-lactamase; DM, diabetes mellitus; d, days.
![]()
Table 3
Risk factors for 14-day mortality (n = 276)
OR, odds ratio; SD, standard deviation; N/A, not applicable; ESBL, extended-spectrum beta-lactamase; DM, diabetes mellitus; d, days.
![]()
When the study population was divided based on mortality by the 14th day from the onset of bacteremia, baseline characteristics were similar between two groups. A higher Pitt bacteremia score (mean: 1.56 in survival group vs. 3.43 in mortality group, P = 0.001), acute kidney injury that necessitated hemodialysis at the onset of bacteremia (OR 18.83, P = 0.005) were more frequent in the mortality group and remained significant after adjusting for confounders. Variables related to underlying diseases, such as hematologic malignancy and Charlson score gained statistical significance after multivariable regression, whereas catheter-related infection (OR 4.41, P = 0.02) lost its significance. Unlike in the 30-day mortality analysis, ESBL-KP bacteremia was significantly and independently associated with higher 14-day mortality (OR 2.76, P = 0.04). Goodness of fit measured by P-value of Hosmer-Lemeshow test was 0.632.
Only 48.0% of people with ESBL-KP infection received appropriate empirical antibiotics therapy, compared to 97.4% of those with non-ESBL-KP infection given appropriate empirical antibiotics. However, an inappropriate empirical antibiotic therapy was not related to higher mortality (OR 2.43, P = 0.16). Moreover, those who were empirically treated with carbapenem showed higher 14-day mortality (OR 3.03, P = 0.02). Higher Pitt bacteremia score and Charlson score were observed in those empirically treated with carbapenem in the present study. Among patients who died within 14 days after the onset of bacteremia (n = 23), those empirically treated with meropenem (n = 13) had a mean Pitt score of 4.46, a mean Charlson score of 5.90. For 30-day mortality cases (n = 44), those empirically treated with meropenem (n = 18) had a mean Pitt score of 3.94, a mean Charlson score of 5.50. The overall mean Pitt score was 1.67, and mean Charlson score was 4.99. A definitive antibiotic therapy did not have a significant association with mortality.
4. Molecular analysis of ESBL-KP isolates
Forty-nine out of 50 ESBL-KP isolates underwent molecular analysis including multilocus sequence typing. Thirty-four (69.4%) produced CTX-M-type and 32 (65.4%) produced CTX-M-14 and/or CTX-M-15 (Table 4). Fourteen sequence types (STs) were identified among CTX-M-14- and CTX-M-15-producing KP isolates, among which ST711 was the most common (18.8%) (Table 5).
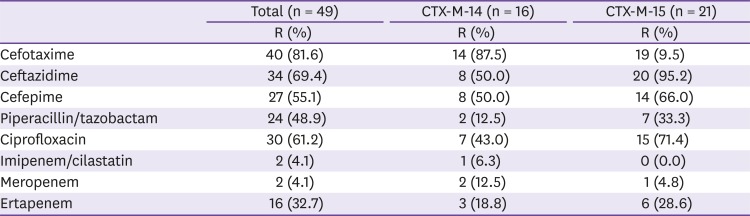
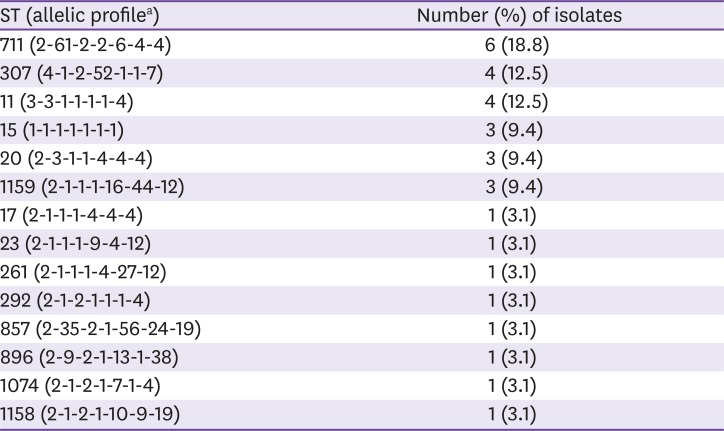
Table 4
Antibiotics susceptibility of ESBL-producing Klebsiella pneumoniae
Five isolates produced both CTX-M-14 and CTX-M-15 enzymes.
ESBL, extended-spectrum beta-lactamase; R, resistant.
![]()
Table 5
Distribution of sequence types among CTX-M-14 or CTX-M-15-producing Klebsiella pneumoniae isolates (N = 32)
![]()
Go to :
Discussion
We demonstrated differences between ESBL-KP and non-ESBL-KP bloodstream infection in adult cancer patients. In addition, we analyzed possible risk factors of mortality of cancer patients with KP bacteremia. Overall, our findings were similar to previous reports in which study populations were not limited to oncology patients [121314151617]. Our finding that exposure to a third-generation cephalosporin was more frequently found in those with ESBL-KP bacteremia was consistent with previous reports [151819]. However, it should be pointed out that by comparing ESBL-producer to non-ESBL-producer, this study might have exaggerated the role of a third-generation cephalosporin in the development of resistance [2021]. Exposure to metronidazole or vancomycin was another risk factor and the latter remained significant after adjustment. A study in 2011 also revealed that those who had ESBL-producing Escherichia coli or ESBL-KP bacteremia had greater exposure to extended-spectrum cephalosporins, fluoroquinolones, aminoglycosides, trimethoprim/sulfamethoxazole, vancomycin, and metronidazole than those who did not [22]. However, independent influence of vancomycin exposure to ESBL-KP infection lacks biological plausibility and no previous study supports this finding. A possible explanation for this is that the impact of use of parenteral antibiotics such as vancomycin could have been overestimated by inclusion of those who might have acquired the pathogen before admission [23]. Although all but four of study population were suspected to have obtained the index infection after admission, the exact length of hospital stay before the index infection was not adjusted in this study, leaving a possibility of certain irrelevant nosocomial environmental factor being falsely attributed.
Not only were the risk of treatment failure during initial 72 hours and death within 14 days after the onset of bacteremia higher in ESBL-KP bacteremia group, but ESBL-KP bacteremia had an independent association with 14-day mortality. At present, more studies support that ESBL production itself does not independently affect mortality. According to a Mexican study [16], even though the study population was not limited to cancer patients, neither mortality nor length of hospital stay had a significant association with ESBL production. Another study that included Taiwanese cancer patients found that ESBL production was not related to increased risk of death. They suggested that septic shock was the only risk factor of mortality [24]. In 2006, Cosgrove et al. [25] analyzed how drug resistance could contribute to adverse clinical outcomes. They pointed out that inadequate or delayed antimicrobial therapy or severe underlying disease might lead to higher risk of death and did not attribute drug resistance itself to adverse outcomes. There is even a study that suggested multidrug resistant E. coli might have a lower virulence than drug-sensitive E. coli [26]. In contrast, there are some studies that suggest a possible relationship between ESBL production and mortality. When initially treated appropriately, those with ESBL-KP bacteremia experienced a higher 15-day mortality than those infected with non-ESBL-KP. When studies concerning ESBL-producing E. coli bacteremia were included, there was even more evidence for this result [192227]. However, although our study support this possible association, we acknowledge that this lacks a clear explanation so far. There has been no report supporting an association between ESBL production and increased virulence, thus highlighting a potential area for further investigation.
Even though ESBL-producing strains seemed to be associated with higher mortality, there was no significant association between appropriateness of empirical therapy and mortality. This may be explained by the fact that the severity of sepsis was an independent risk factor for mortality. At our institution, we generally do not begin with carbapenem unless the patient is critically-ill or is expected to be at an increased risk of multidrug-resistant bacterial infection. In other words, increased mortality in those empirically treated with carbapenem may be due to more severe infection itself, considering a positive association between higher Pitt bacteremia score and mortality. This result is in accordance with other studies which were based on population not restricted to cancer patients. A report in 2006 claimed that inappropriate empirical therapy showed no statistically significant difference in relation to death regardless of ESBL production [28]. In another study with 19 cases of ESBL-KP bacteremia, no significant difference in mortality was observed between patients who received appropriate empirical antibiotic therapy and those who did not [29]. On the contrary, Hyle et al. observed that inadequate empirical antimicrobial therapy was an independent risk factor for mortality in ESBL-KP bacteremia [30]. A study in which ESBL-producing Enterobacteriaceae bacteremia cases were included, Tumbarello et al. reported that inadequately treated patients had a three-fold increase in 21-day mortality compared to the adequately treated patients [31].
There are several limitations in this study. First, because all cases were from a single tertiary-care center, the results may be not generalizable. Second, being retrospective, there might have been some variables that could not be taken into consideration. Finally, the number of patients who started mechanical ventilation or renal replacement therapy at the onset of bacteremia was small, which might make the association between these variables and mortality less reliable.
In conclusion, there were several differences in clinical characteristics between ESBL-KP and non-ESBL-KP bacteremia in cancer patients, similar to previous reports including non-cancer patients. ESBL production was associated with 14-day mortality, but not with 30-day mortality, and mortality was affected by severity of sepsis and occurrence of organ failure such as acute kidney injury.
Go to :
 XML Download
XML Download