

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Severe trauma causes tissue damage, collapse of the skin barrier, and alterations in the immune system. As a result, patients with severe trauma are vulnerable to bacterial invasion and infection [12]. In particular, methicillin-resistant Staphylococcus aureus is a major pathogen in intensive care units (ICUs) and patients with severe trauma can easily contract S. aureus infection [3].
Vancomycin is the first-line antibiotic used in the treatment of methicillin-resistant S. aureus (MRSA) infection [4]. Vancomycin is an area under the concentration curve-dependent antibiotic, and suboptimal serum concentrations of this drug lead to treatment failure and the development of resistance [56]. Thus, serum vancomycin concentrations must be measured in patients with severe trauma by therapeutic drug monitoring (TDM) [7]. In a 1,084-bed tertiary hospital which this study had done with a trauma ICU (TICU), suboptimal serum vancomycin concentrations were more frequently observed in severe trauma patients than medical intensive care unit (MICU) patients.
Vancomycin clearance (CLvan) is influenced by many factors. A patient's renal function and use of continuous renal replacement therapy (CRRT) have a decisive effect on CLvan. Capillary fluid leakage leads to changes in the volume of distribution (Vd) and CLvan [8]. Intensive fluid therapy for critically ill patients causes pharmacokinetic alterations due to the hydrophilicity of vancomycin [5]. The simultaneous use of other drugs influencing renal function and the use of vasoactive drugs affect CLvan [59].
In this study, the factors affecting vancomycin levels between multiple trauma patients in the TICU and MICU stratified by use of CRRT were compared. Furthermore, the influence of these factors on CLvan was statistically analyzed.
Go to : 
Materials and Methods
1. Study population
The data from the TDM database at the pharmacy of one tertiary care hospital was retrieved for the retrospective selection of appropriative cases. The TDM database includes information on patient's characteristics and the pharmacokinetic parameters of vancomycin. Patient's information (age, height, actual body weight, sex, serum creatinine rate, and trough level of vancomycin) are entered into the TDM software, which then calculates the pharmacokinetic parameters (half-life, Vd, optimal dose of vancomycin, and CLvan). Patients aged >18 years who were admitted to the TICU or MICU from January 2015 to December 2015 were selected. All patients received vancomycin intravenously by intermittent infusion. The vancomycin dose, calculated by the ideal body weight (IBW), was 1 g every 12 hours averagely in the non-dialyzed patients. In the case of patients undergoing CRRT, the vancomycin dose was 1 g/day averagely. Patients received vancomycin infusions at least thrice consecutively, then the serum vancomycin levels were measured just prior to the next dose at steady-state conditions according to TDM timing recommendation [7]. TDM was analyzed as vancomycin doses are adjusted by clinicians, as a result of TDM for the achievement of the target vancomycin level (15 – 20 μg/mL) in the second trough. In cases in which vancomycin administration was stopped for >7 days and restarted, the second TDM and trough level were analyzed again as a new case. As a result, some patients were considered as representing more than one case. Exclusion criteria were children aged ≤ 18 years old, those with an end-stage renal disorder on intermittent hemodialysis or continuous ambulatory peritoneal dialysis, and women who were pregnant. This study was approved by the Ajou University Hospital Institutional Review Board (AJIRB-MED-MDB-17-161).
2. Data collection
We reviewed patients' medical histories, laboratory results, use of vancomycin and other drugs, as well as clinical findings. Among the patient characteristics, weight was specifically recorded as actual body weight, IBW, overweight (kg; weight - IBW), overweight rate (percent; (overweight/IBW) × 100), and body mass index (BMI; kg/m2). Fluid input and output were specifically analyzed as total fluid input/output (L; total fluid input – total fluid output), one-day fluid output per weight, and one-day urine output per weight. The insensible loss of fluid was calculated as 500 ml/day. The rate of creatinine clearance was calculated by the Cockroft-Gault formula [10]. Augmented renal clearance (ARC) was defined as an increased creatinine clearance of greater than 130 ml/min/1.73 m2 [11]. The use of vancomycin in the culture of MRSA was identified as therapeutic use of vancomycin (versus empiric use). Sub-therapeutic level of vancomycin was defined as a trough level of vancomycin of lesser than 15 mg/L. The use of drugs that affected renal function (vasoactive agents, angiotensin receptor blockers, non-steroidal anti-inflammatory drugs, mannitol, aminoglycoside, and furosemide), a number of simultaneously used antibiotics (beta-lactams, macrolide, colistin, aminoglycoside, tetracycline analogues, metronidazole, quinolone, antifungal agents, and antiviral agents), and furosemide dosage were also analyzed. The type of CRRT used was continuous venovenous hemodiafiltration. The velocity of CRRT was calculated as the intensity of CRRT ([dialysate fluid flow + replacement fluid flow + ultrafiltration flow]/hour/weight of patient; mL/hour/kg) [12]. The clinical severity of patients was evaluated using the Injury Severity Score [13] in the TICU and the Simplified Acute Physiology Score 3 [14] in the MICU.
3. Vancomycin concentration assay and pharmacokinetic parameters
We identified that the sampling for the measurement of serum vancomycin trough levels was performed one hour before the next dose. The samples were analyzed by fluorescence polarization immunoassay (Cobas Integra 800, Roche Diagnostics, Mannheim, Germany).
Based on the measured concentrations, we estimated the pharmacokinetic parameters (Vd, half-life [T1/2]). The pharmacokinetic parameters were estimated by a Bayesian (non-linear) method using CAPCIL® software (SIMKIN Inc., Gainesville, FL, USA) [15]. We used K12 = 1.12 (hr -1: the central to peripheral transfer rate constant), K21 = 0.48 (hr -1: the peripheral to central transfer rate constant) for the pharmacokinetic parameter analysis with a 2-compartment model. In this method, pharmacokinetic parameters (elimination rate constant (Ke) and Vd) that reduce the difference between the actual and predicted concentrations are sought. The T1/2 value was calculated automatically using the equation T1/2 = 0.693/Ke. CLvan was calculated using the equation CLvan = Ke × Vd. Optimal vancomycin doses were also calculated by this software.
4. Statistical analysis
Continuous variables were expressed as mean ± standard deviation, and categorical variables were presented as frequencies and percentages. Group comparisons were analyzed independently by a Student's t-test for continuous variables and chi-square test for categorical variables. Pearson's correlation analysis and Spearman correlation analysis were performed to evaluate the correlations between the continuous variables and CLvan. Furthermore, Student's t-test and Mann-Whitney U-test were performed to evaluate the correlations between the categorical variables and CLvan. The interrelationships of each variable were analyzed by multiple linear regression. A two-tailed P-value <0.05 was considered statistically significant. All statistical analyses were performed with IBM SPSS Statistics (version 21.0; IBM Corp., Armonk, NY, USA).
Go to :
Results
1. Characteristics of the study population
We identified 202 cases (175 patients) with TDM in two ICUs during the study period, comprising 87 TICU cases (67 patients) and 115 MICU cases (108 patients). Thirty cases in which the inclusion criteria were not met were excluded. Seventy-six TICU cases and 96 MICU cases were included in the final analysis (Fig. 1).
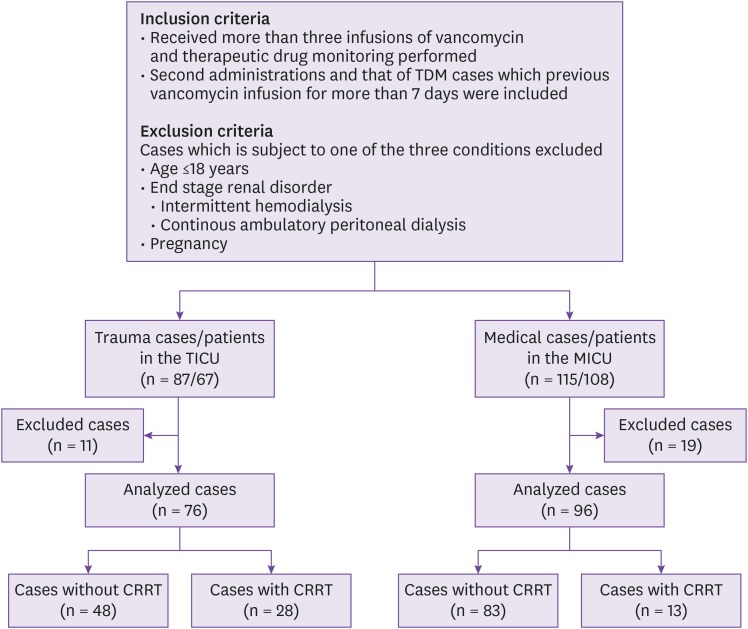
Table 1 shows the clinical characteristics and laboratory findings of the TICU and MICU non-dialyzed groups. A total of 48 TICU cases and 83 MICU cases were enrolled. The mean age of the patients in the TICU (50.17 ± 19.1 years) was significantly lower than that of those in the MICU (67.41 ± 14.35 years; P < 0.001). However, the height (168.91 ± 8.14 cm vs. 164.05 ± 8.43 cm; P = 0.002) and actual body weight (71.93 ± 14.78 kg vs. 58.36 ± 19.88 kg; P < 0.001) of the TICU patients were significantly higher than those of the MICU patients. The mean IBW (64.28 ± 8.34 kg vs. 59.35 ± 9.02 kg; P = 0.002), overweight (7.65 ± 14.57 kg vs. 7.65 ± 14.57 kg; P = 0.002), BMI (25.20 ± 5.02 kg/m2
vs. 21.49 ± 5.79 kg/m2; P < 0.001) and body surface area (BSA) (1.82 ± 0.20 cm0.725 × kg0.425 × 0.007184 vs. 1.61 ± 0.25 cm0.725 × kg0.425 × 0.007184; P < 0.001) were higher in the TICU patients than the MICU patients. No significant differences were observed in terms of sex, or the prevalence of diabetes mellitus or chronic kidney disease between the two groups.
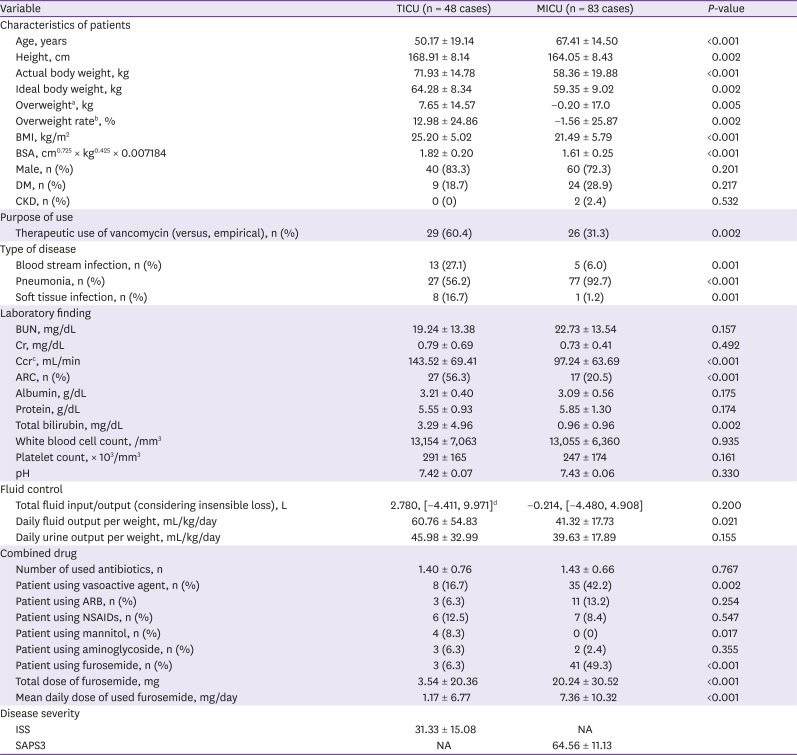
Table 1
Clinical characteristics of non-dialyzed patients in the TICU and MICU
aOverweight = weight - ideal body weight.
bOverweight rate = {(weight - ideal body weight)/ideal body weight} × 100.
cCcr = [{(140 - age) × weight}/(72 × Cr)], if female × 0.85.
d[ ], interquartile range.
TICU, trauma intensive care unit; MICU, medical intensive care unit; BMI, body mass index; BSA, body surface area; DM, diabetes mellitus; CKD, chronic kidney disease; BUN, blood urea nitrogen; Cr, creatinine; Ccr, creatinine clearance; ARC, augmented renal clearance; pH, potential of hydrogen; ARB, angiotensin receptor blocker; NSAIDs, nonsteroidal anti-inflammatory drugs; ISS, Injury Severity Score; NA, not assessed; SAPS3, Simplified Acute Physiology Score 3.
![]()
The rate of therapeutic use (versus empiric use) of vancomycin was significantly higher in the TICU patients (60.4%) than in the MICU (31.3%; P = 0.002). The rate of bloodstream infections was higher in the TICU patients (27.1%) than the MICU patients (6.0%; P = 0.001). The pneumonia prevalence rate was lower among the TICU patients (56.2%) than the MICU patients (92.7%; P < 0.001). The rate of soft-tissue infection in the TICU patients (16.7%) was higher than that in the MICU patients (1.2%; P = 0.001).
The rate of creatinine clearance (Ccr; 143.52 ± 69.41 mL/min vs. 97.24 ± 63.69 mL/min; P < 0.001) and level of total bilirubin (3.29 ± 4.96 mg/dL vs. 0.96 ± 0.96 mg/dL; P = 0.002) and rate of ARC (56.3% vs. 20.5%; P < 0.001) were significantly higher in the TICU patients than MICU patients. However, the serum blood urea nitrogen, creatinine, albumin and total protein levels, white blood cell count, platelet count, and potential of hydrogen were not different between the two groups.
The total fluid input/output (considering insensible loss) from the time of ICU hospitalization to the measurement of serum vancomycin concentrations was not different between the TICU and MICU patients (2.780 ± 14.382 L vs. -0.214 ± 9.389 L; P = 0.200). The one-day fluid output per weight of the TICU patients (60.76 ± 54.83 mL/kg/day) was higher than that in the MICU patients (41.32 ± 17.73 mL/kg/day; P = 0.021). No difference in the one-day urine output per weight was observed between the TICU and MICU patients (45.98 ± 32.99 mL/kg/day vs. 39.63 ± 17.89 mL/kg/day; P = 0.155).
The rate of use of vasoactive agents among patients in the TICU (16.7%) was lower than that among those in the MICU (42.2%; P = 0.002), and the use of mannitol in the TICU (8.3%) was higher than in the MICU (0.0%; P = 0.017). The rate of use of furosemide in the TICU (6.3%) was lower than in the MICU (49.3%; P < .001). The total volume (3.54 ± 20.36 mg vs. 20.24 ± 30.52 mg; P < 0.001) and one-day mean volume (1.17 ± 6.77 mg/day vs. 7.36 ± 10.32 mg/day; P < 0.001) of furosemide in the TICU during the vancomycin administration period was significantly lower than in the MICU (Table 1).
2. Pharmacokinetics of vancomycin
No significant difference in the total vancomycin dose (dose of vancomycin before TDM) was observed among the non-dialyzed patients between the two ICU groups (5.19 ± 1.81 g vs. 4.90 ± 1.60 g; P = 0.347). The one-day mean vancomycin dose was not different between the two groups (1.96 ± 0.45 g/day vs. 1.91 ± 0.36 g/day; P = 0.477). However, the one-day mean vancomycin dose per weight (actual body weight) was significantly lower in the TICU patients than the MICU patients (27.85 ± 5.88 mg/kg/day vs. 34.71 ± 9.24 mg/kg/day; P < 0.001). The serum vancomycin trough levels were lower in the TICU patients than the MICU patients (trough level, 10.42 ± 8.13 μg/mL vs. 14.63 ± 8.47 μg/mL; P = 0.006). Among the TICU patients, the sub-therapeutic trough level of vancomycin was observed in 84.6% of blood stream infection, 70.4% of pneumonia and 75% of soft tissue infection cases. And that was higher than that of MICU patients (40%, 70.4%, and 0%). The Vd of vancomycin was higher among the TICU patients than the MICU patients (51.12 ± 7.92 L vs. 45.82 ± 8.70 L; P = 0.001). The optimal vancomycin dose was calculated through the initial dosage and serum vancomycin trough level, and the optimal vancomycin dose was higher in the TICU patients than the MICU patients (3.25 ± 1.64 g vs. 2.09 ± 1.10 g; P <0.001). The CLvan rate was significantly higher among the TICU patients than the MICU patients (74.25 ± 27.99 mL/min vs. 53.74 ± 23.91 mL/min; P <0.001).
No significant differences in the total vancomycin dose, one-day vancomycin dose per weight, serum vancomycin peak level, serum vancomycin trough level, T1/2 of vancomycin, optimal vancomycin dose, or CLvan were observed between the two ICU groups in patients undergoing CRRT (Table 2).
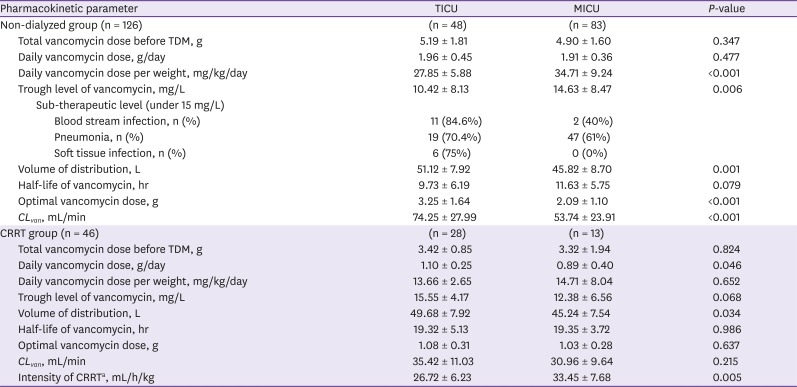
Table 2
Pharmacokinetics of vancomycin in the TICU and MICU patients
aIntensity of CRRT = (dialysate fluid flow + replacement fluid flow + ultrafiltration flow)/hour/weight of patient.
TICU, trauma intensive care unit; MICU, medical intensive care unit; TDM, therapeutic drug monitoring; CLvan, vancomycin clearance; CRRT, continuous renal replacement therapy.
![]()
3. Factors associated with vancomycin clearance
The factors associated with CLvan were evaluated by the Pearson's correlation analysis test, Student's t-test, and multiple linear regression continually. In the case of non-dialyzed patients, variables that significantly differed between the two ICU groups in terms of clinical characteristics and laboratory findings were selected. Then we identified correlations between selected variables and CLvan of patients in the TICU. The results of the Pearson's correlation analysis and Student's t-test showed that age, height, IBW, BSA, Ccr, serum total bilirubin, furosemide use, and mean daily dose of furosemide were associated with CLvan in the TICU group. Considering the variation inflation factor in the multiple linear regression, height and IBW values were excluded. In the multiple linear regression, the only factor associated with CLvan in the non-dialyzed group was serum Ccr (R2 = 0.559, P < 0.001; coefficient = 0.156, P = 0.017) (Table 3).
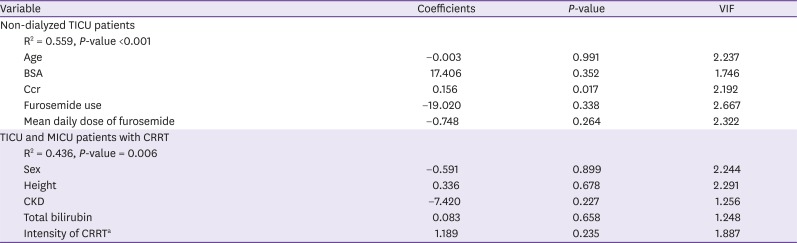
Table 3
Multiple linear regression of the factors associated with vancomycin clearance in non-dialyzed TICU patients and patients with CRRT in the TICU and MICU
aIntensity of CRRT = (dialysate fluid flow + replacement fluid flow + ultrafiltration flow)/hour/weight of patient.
TICU, trauma intensive care unit; CRRT, continuous renal replacement therapy; MICU, medical intensive care unit; VIF, variation inflation factor; BSA, body surface area; Ccr, creatinine clearance; CKD, chronic kidney disease.
![]()
In the case of patients undergoing CRRT, the CLvan rate was not significantly different between the two ICU groups. So, we investigated the factors associated with CLvan in all the ICU groups. The results of the Pearson's correlation analysis and variation inflation factor of the multiple linear regression showed that sex, height, underlying chronic kidney disease, serum total bilirubin and intensity of CRRT were associated with CLvan. However, in the multiple linear regression analysis, none of the factors was associated with CLvan (R2 = 0.436, P = 0.006) (Table 3).
Go to :
Discussion
In this study, multiple trauma patients in the TICU were compared to patients in the MICU for the identification of the factors associated with CLvan. The patients' factors that significantly differed between the TICU and MICU patients were age, height, actual body weight, IBW, overweight, BMI, BSA, therapeutic use of vancomycin (vs. empiric use), site of infection, serum Ccr, rate of ARC, serum total bilirubin, one-day fluid output per weight, use of vasoactive agents, use of mannitol, use of furosemide, and furosemide dose.
Multiple trauma patients develop immune system alterations through tissue damage, resulting in capillary leakage and peripheral fluid retention [1]. Such patients should undergo intensive fluid therapy for hemodynamic stabilization. These processes affect drug pharmacokinetics, augment renal drug elimination, increase the Vd, and decrease serum drug concentrations [8916]. Weight gain occurs because of traumatic damage and massive fluid therapy, thus reflecting the degree of damage and treatment intensity. It is expected that drug clearance increases with weight gain.
In this study, the largest differences between the two ICU patient groups were observed in the weight indices. The patients in the TICU were heavier and taller and had a higher IBW and rate of overweight than those in the MICU. The overweight rate was found to be 12.98 ± 24.8% in patients in the TICU undergoing high-intensity therapy and with a high degree of tissue damage. The actual body weight of the MICU patients was lower than their IBW; this may be a result of the long-term strict management of pulmonary edema which required negative fluid balance.
Serum Ccr is measured using the Cockcroft-Gault equation, which includes serum creatinine, age, and actual body weight. The serum Ccr values in this study were markedly different between the TICU and MICU patients (143.52 ± 69.41 mL/min vs. 97.24 ± 63.69 mL/min; P < 0.001), the rate of ARC was higher in TICU patients than MICU patients (56.3% vs. 20.5%; P < 0.001); however, the serum creatinine level did not differ (0.79 ± 0.69 mg/dL vs. 0.73 ± 0.41 mg/dL; P = 0.492). It is thought that ARC originate from age and the actual body weight of patients.
Table 2 shows the pharmacokinetics of vancomycin in the two groups according to the use of CRRT. The one-day vancomycin dose in the non-dialyzed group was not different between the two ICU group patients, and the actual body weight was higher in the TICU patients. As a result, the one-day vancomycin dose per weight is expected to be lower in TICU patients than MICU patients. The vancomycin dose was nearly 2 g/day in both ICUs, resulting from the consideration of IBW. Heavier TICU patients are administered a relatively lower dose, while the CLvan is higher in TICU patients; therefore, the serum vancomycin peak and trough levels are lower in TICU patients than MICU patients. The CLvan in the CRRT group was not different between the patients in the two ICUs. In the CRRT group, hemodiafiltration is the only method used for vancomycin elimination, so CLvan is not affected by other patients' variables. Thus, CLvan should not be considered in the determination of the vancomycin dose for patients in either ICU type.
Table 3 shows the results of the multiple linear regression, in which correlations were observed between patient factors and CLvan. In the non-dialyzed TICU group, the only factor showing a significant correlation was serum Ccr. The correlation between CLvan and serum Ccr, as observed in our study, has been confirmed by studies including non-severe trauma patients and neurosurgical ICU patients [1718].
As mentioned above, serum Ccr includes patient age, actual body weight, and serum creatinine concentrations. In our study, these three factors did not affect CLvan individually, but they were correlated with CLvan when considered simultaneously. Actual body weight showed the largest number of differences of the aforementioned three factors between the TICU and MICU patients. Thus, the actual body weight of patients should be considered in the determination of vancomycin dose.
In studies about ARC, the ARC associated with younger age, male gender, trauma, lower critical illness severity scores [11]. In those studies, body weight was not so related with ARC. The reason is that there is no significant difference in weight from the control, thus weight indicators were not importantly analyzed [192021]. In our study, the weight gain was important feature of TICU patients. Severe trauma patients required massive fluid therapy, thus patients with ARC should be taken care of weight.
Medellin-Garibay et al reported that the use of furosemide in trauma patients affects the pharmacokinetics of vancomycin, but our study showed no significant correlation with the use of furosemide [18]. That study, however, included all types of trauma patients. However, in our study, we included severe trauma patients, who were hospitalized in the TICU; therefore, the number of patients using furosemide was small (n = 3, 6.3%) as was the furosemide dose (1.17 ± 6.77 mg/day). Further studies need to be conducted to clarify this point.
CRRT use may affect drug clearance. Drugs with a high molecular weight, such as vancomycin, are influenced more by CRRT intensity than the CRRT method [2223]. In our study, many factors were analyzed for the determination of their association with CLvan in the CRRT group, but none of the factors showed correlations, including the CRRT intensity (Table 3). Previous studies differ from our study in that our participants included trauma patients. Patients in the TICU differ from those in the MICU based on the volume of fluid therapy and actual body weight, which affect drug pharmacokinetics; this may be the reason for the observed differences between our study and previous studies.
No difference in terms of CLvan in the CRRT group was observed between the patients in the two ICUs (Table 2), and there were no factors that affected CLvan in both sets of patients (Table 3). Therefore, vancomycin dosing can be performed using a fixed dose in patients undergoing CRRT.
This study has several limitations that should be mentioned. First, the clinical characteristics including age and ideal body weight were different between two groups, so the control group may not be appropriate. Second, the sample size was relatively small for the identification of differences between the two groups. Third, this study was conducted at a single referral center in Far East Asia, so the results may not be applicable to other regions. Fourth, the number of patients using furosemide was small. Furosemide is an important drug affecting drug clearance. In this study, the influence of furosemide could not be determined.
The actual body weight of TICU patients with multiple trauma easily changes compared to other patients in the ICU because of intensive fluid therapy administration. And actual body weight would be an important factor of ARC. Therefore, the vancomycin dose should be controlled in non-dialyzed TICU patients, depending on the actual body weight changes. Further, therapeutic vancomycin levels should be monitored for the maintenance of optimal therapeutic levels of vancomycin. In the case of dialyzed patients in both ICUs, vancomycin can be infused with fixed doses regardless of patients' characteristics.
Go to :
 XML Download
XML Download