

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Domestic Incidence and Epidemic
Dysentery epidemics have been common in Korea for a long time, particularly in the summer [1]. The first historical mention of the dysentery in Korea dates back to September of the sixth year of King Shinjong's reign in Korea dynasty (1202) in a book named 前王患痢疾(Jeonwanghwan dysentery). A prescription for diarrhea can also be found in Donguibogam (Principles and Practice of Eastern Medicine). However, Donguibogam did not distinguish between communicable and non-communicable diarrhea [1]. During the Japanese colonial period, 佐藤 (Jwadeung) [2] stated that the reason there was such a high incidence of dysentery in Korea was that the concept of hygiene was not properly established. In addition, the management system for drinking water was also in a poor condition [1]. Considering the national circumstances in that period, both reasons are reflective of the overall state of Korea at that time. As can be seen from the above examples, dysentery has been a major cause of domestic food poisoning for a long time and national epidemics have still occurred until recently. In this chapter, we aim to describe the characteristics of the domestic incidence of dysentery after the colonial period and the characteristics of the disease, with a main focus on bacillary dysentery. Domestic epidemiological research on dysentery outbreaks, as is the case for other infectious diseases, has limited amount of data, making it difficult to give a full account of the facts. After the national liberation, the UN allied forces began to study the domestic dysentery outbreaks during the Korean War [34]. After the war, the disease began to be monitored by the Korean National Institute of Health [4]. Table 1 shows the number of dysentery cases in Korea from 1954 to 2013, published by the Centers for Disease Control and Prevention [5]. Along with typhoid, dysentery has been the most common disease among domestic food-borne legal communicable diseases. Regarding typhoid, its incidence peaked in the 1960s and it has shown a steady decrease since then, whereas dysentery showed a low incidence during the period of 1980s and up to the mid-1990s but the epidemic broke out again and showed rapid increase by period. Figure 1 shows the number of annual domestic cases of dysentery for the period from 1991 to 2017 [6].

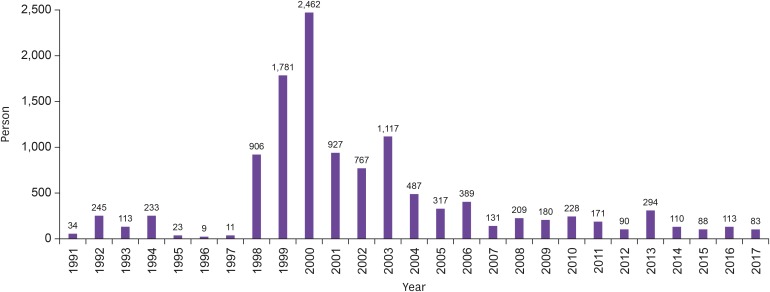 | Figure 1Number of annual domestic outbreak cases of dysentery for the period between 1991 to August, 2017.
|
Table 1
Number of reports on foodborne legal communicable diseases in Korea, 1954-2013 [5]
![]()
As shown in Figure 1, dysentery was epidemic between 1998 and 2003, but since 2004 it has declined every year, showing a low incidence rate in recent years. The epidemiological status of dysentery in Korea however shows a different time-dependent pattern, and therefore, the epidemiological characteristics of each period will be described below by dividing into several periods covering the period from the time after the national liberation to the present.
1. Korean War Period
As is the case in other wars, epidemics such as typhus fever, relapsing fever, typhoid fever, and smallpox broke out during the Korean War. Bacillary dysentery was prevalent among North Korean military prisoners in 1950-1951 [4]. Approximately two thirds of patients complaining of fever and diarrhea in early 1950 had bacillary dysentery, and Shigella flexneri was the causative pathogen in more than 95% of the cases [34]. In 1952-1953, S. flexneri was the most common strain accounting for 90.9% of the 3,732 Shigella isolates obtained from soldiers, refugees and prisoners while there were relatively fewer cases of isolation of Shigella dysenteriae (6.3%), Shigella sonnei (2.3%) and Shigella boydii (0.5%) [78].
2. 1960s - 1970s
Although the reported number of dysentery cases may not represent the definitive actual situation in Korea in this period, it can be seen that the incidence of domestic dysentery decreased in the 1970s compared to the 1960s. Table 2 shows the collection and reorganization of the data on the serotype analysis of domestic dysentery after the Korean War [7]. Shigella serotypes in Daegu and Gyeongbuk regions in the 1960s showed a similar distribution to that of the 1950s [91011]. The serotype distribution of Shigella in the 1970s is similar to that in the 1960s, but S. sonnei shows an increase. In addition, the use of antibiotics in the 1970s increased the drug resistance of Shigella [12]. In addition to chloramphenicol, tetracycline, streptomycin, and sulfonamide resistance, the resistance of Shigella to cotrimoxazole and ampicillin also increased, resulting in an increase in multidrug-resistant Shigella from 50% in 1973 to 95% or higher since 1977.

Table 2
Dysentery Incidence in Korea for the past 50 years [7]
![]()
3. 1980s - 1997
From the 1980s to 1997, the incidence of dysentery in Korea remained consistently low. The most common serotype in the 1980s was S. flexneri, but S. sonnei showed a steady increase (Table 2). During this period, Korea's socio-economic development triggered an improvement in overall hygiene habits in the country. In addition, the national health insurance system, which began in 1977, expanded to regional medical insurance in 1989, stabilizing the health insurance system and public health system at a national level. Meanwhile, the government also made efforts to eliminate enteric infectious diseases such as salmonella, dysentery, and cholera. The 1990s was the period with the lowest incidence of dysentery in Korea. In 1996 and 1997, there were only 9 and 11 cases of dysentery, respectively, nationwide (Fig. 1). The most common serotype in this period was S. sonnei. From the 54 Shigella strains isolated in 1991, S. sonnei accounted for 79.6%, followed by S. flexneri at 18.5%. This was the first time that S. sonnei was present in a higher proportion than S. flexneri in Korea [7]. Since then, S. sonnei has been the most common serotype in the country. Further analysis on the biotype or genotype analysis of S. sonnei showed that new clones were introduced in the 1990s that were different from those from the 1980s, replacing the existing clones [1314]. In this period, Shigella mostly showed resistance to sulfamethoxazole, tetracycline, and trimethoprim, but was susceptible to cefotaxime, ciprofloxacin, and norfloxacin. However, nalidixic acid resistance increased from 7.7% to 100% in the 1980s [15].
4. National epidemic during the Period 1998 - 2004
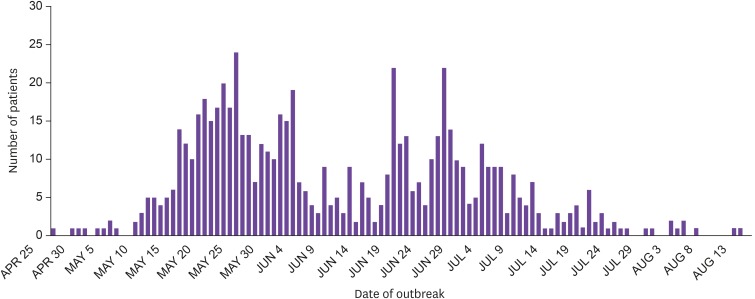
In 1998, dysentery, which had shown a rare incidence in Korea for some time, showed a sudden and rapid increase. There were 906 cases in 1998 alone, peaking at 2,462 cases in 2,000 (Fig. 1). Most cases were related to the S. sonnei strain, but the S. flexneri epidemic also occurred almost every year, and the proportion of S. flexneri changed according to the scale of the epidemic [7]. S. sonnei epidemic strains in this period had a similar genotype to that of the strain which was introduced in the 1990s and showed sporadic outbreaks [7]. We will look into several major epidemic cases to better understand the situation in each case. The nationwide elementary school meal provision began in 1998, and since the fall of 1999 the high school meal provision also started; the dysentery outbreaks in 1998 and 1999 were associated with these school meals. For example, all the five outbreaks in 1999 in Gyeonggi, Chungnam, Busan, and Gyeongnam occurred in kindergarten, elementary school, and high school settings and they were large-scale, ranging from tens to hundreds of patients [16]. From 1998 to 2000, the period when dysentery was highly epidemic, the average incidence by region was 6.0 cases or more per 100,000 people in Gangwon, Jeonnam, Gyeongnam, and Jeju, indicating that these regions were the most affected. For Seoul, Incheon, Daejeon, and Jeonbuk regions, the incidence was less than 1.0 case [1617]. In Jeju, in particular, incidences of 0 and 2.62 per 100,000 people in 1998 and 1999, respectively, rose to 306.8 in 2000, which is an explosive increase (Fig. 2) [18]. A total of 29% and 45% patients with dysentery fell within the 10 years age group in 1999 and 2000, respectively, and 44% and 20% patients were between 10-19 years old, for 1999 and 2000, respectively. This indicates that the outbreak occurred mainly among the school-aged population. The major pathways of transmission for the domestic dysentery epidemic in 1999 and 2000 were food, water, and contact, which were estimated at 50%, 38.5%, and 11.5%, respectively. Overall, this indicates that food was the key source of infection, while water supply also acted as a major source. Infection from contact occurred primarily among infants and preschoolers. When food was the common source of infection, the school meal was found to be the major source together with other meal-providing sources such as the catering service in the local community and mall food services. In November 2004, a dysentery epidemic occurred at an elementary school in Chungju [19]. The outbreak started with 248 cases at the elementary school and then another 17 cases occurred in a neighboring daycare center, showing the extensive scale of the epidemic. The pathogen in question was also a multidrug-resistant (ampicillin, tetracycline, trimethoprim-sulfamethoxazole and 3rd-generation cephalosporin resistant) bacterium producing CTX-M-14 ESBL (extended-spectrum beta-lactamase). At the time, there was much debate around whether fluoroquinolone could be used as a treatment, given that dysentery outbreak occurred mainly in an elementary school among young children. Fortunately, since 2004, the incidence of domestic dysentery has decreased.
5. Since 2005
After the period between 1998 and 2004, the period of the nationwide dysentery epidemic, the incidence of domestic dysentery has remained relatively stable until now. However, as overseas travel has increased, the number of cases of imported dysentery have also increased, with this trend being especially clear since 2007 [20]. In 2010 and 2011, 212 (53.1%) of the 399 dysentery cases were imported cases. There were many cases of contraction of dysentery after traveling to Southeast Asia with the order of visited countries being India (21.7%), Cambodia (19.8%), Philippines (17.9%), and Vietnam (9.0%), with S. sonnei (65.6%) and S. flexneri (20.3%) being the most common strain types. In terms of timing, incidence was the highest in July and August, and in terms of age group, incidence was the highest among people in their twenties. With the increase of imported dysentery, more cases of multidrug-resistant dysentery are being reported. Shigella producing CTX-M-55 ESBL was imported from China [21] and Shigella resistant to fluoroquinolone, one of the major treatments, was imported from Vietnam and India [2223]. The Vietnam-imported dysentery showed a small-scale outbreak through the spread between families and through a daycare center. This outbreak was especially problematic because the Shigella was resistant to ciprofloxacin and the strain produced ESBL. Dysentery imported from overseas is expected to become more common in the future; thus, it requires continuous monitoring and control.
Now, we have examined the status of dysentery outbreaks in Korea from the period after the Korean War until the present. In summary, there was a nationwide dysentery epidemic between 1998 and 2004, and since then, the incidence has been stably low. Regarding the latest trends, more than half of the Shigella cases have been imported cases.
Go to : 
Characteristics of Dysentery in Korea
1. Epidemiological characteristics
Dysentery has a typical fecal-oral transmission [24]. The dysentery patient, a reservoir, excretes Shigella through feces for several weeks. Ingestion of only 10 - 100 Shigella can cause lead to the development of the disease in humans, which indicates that the person can be infected by contact. In Korea, food is the most common pathway for the spread of the disease and infections by contact have been reported in kindergartens, while dysentery outbreaks by water pollution, such as contaminated water in a communal well, also occur in developing countries.
2. Antimicrobial resistance of Shigella in Korea
Table 3 shows the antimicrobial resistance rate of Shigella isolated in Korea from 1998 to 2004 [19]. The resistance rate varies depending on the year and epidemic pattern, but they are mostly resistant to ampicillin, nalidixic acid, and trimethoprim/sulfamethoxazole, making it difficult to use those drugs as treatment.
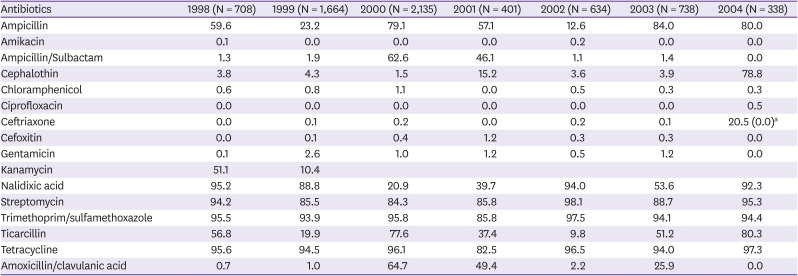
Table 3
The antibiotics resistance rate of Shigella isolated in the period 1998 - 2004 in Korea (%)
aIn 2004, there were no ceftriaxone resistant strains except for 78 strains that were subject to antibiotic susceptibility tests among 267 strains from the group outbreak cases included in this study.
Source: Centers for Disease Control and Prevention, Department of Enterobacteria.
![]()
3. Symptoms
The incubation period for dysentery ranges from 12 to 96 hours [1724]. In some cases, symptoms can be mild or the patient may even be asymptomatic. Main symptoms include high fever and nausea, occasional vomiting, cramping, abdominal pain, and diarrhea with tenesmus. In typical cases, the feces contain blood or pus. Rarely, infants experience central nervous system manifestations such as convulsions. S. dysenteriae leads to the most severe symptoms, followed by S. flexneri and S. sonnei in terms of the severity of clinical symptoms [25]. Shigella does not cause bacteremia in most cases, even in severe infections, as it causes inflammation of the mucous membranes. It can be asymptomatic or pass with mild symptoms and is usually treated in 4-7 days.
4. Diagnosis
Patients with diarrhea and systemic symptoms, such as fever, should be screened to check for bacillary dysentery [172425]. In diarrhea patients, wet specimens of feces may help to diagnose inflammatory bowel disease (IBD). In particular, if diarrhea lasts more than 48 hours and spreads within the family, occurring at intervals of 1 - 3 days, the likelihood of dysentery is high. Feces should be smeared on slides and stained with methylene blue. A high count of white blood cells may typically be observed under the microscope. A definite diagnosis can be given when Shigella is isolated from the feces. Shigella is vulnerable to acid; therefore, if transportation is lengthy, then the sample should be refrigerated for storage or inoculated into a carrier medium.
5. Treatment
To treat dehydration from diarrhea and vomiting, water and electrolytes are administered orally [25]. Patients with severe vomiting or sickness are administered water and electrolytes intravenously. Most cases of dysentery self-resolve over time and do not require antibiotics, but severe cases of dysentery may require antibiotics. Antibiotics can be used to shorten the duration of Shigella excretion, that is, to reduce the spread of the bacterium. Since 2000, the rates of antimicrobial resistance of S. sonnei isolated in Korea have been high, with rates reaching 91% for ampicillin, 41% for ampicillin/sulbactam, 9% for kanamycin, and 82% for trimethoprim/sulfamethoxazole. Many ESBL-producing strains have been reported [252627]. Therefore, the antibiotic therapy recommended by The Korean Society of Infectious Diseases/Korean Society for Antimicrobial Therapy is 750 mg of ciprofloxacin once daily for 3 days or 500 mg of azithromycin once daily for 3 days [25].
Go to :
Prevention and Control
After the establishment of the Government of the Korea, the Prevention of Contagious Diseases Act was promulgated as Law No. 308 in 1954. The Act, enacted after the Korean War, was mostly based on the “Decree on Infectious Diseases Prevention” during the Japanese colonial period. The legal communicable disease was divided into levels 1, 2, and 3, with dysentery being categorized into level 1. Level 1 has 12 diseases, including cholera, plague, typhoid fever, and typhus fever. The main content of the Act was the stipulation that level 1 and level 2 diseases should be reported immediately while level 3 diseases should be reported once a month. The Act also included inoculation of some of the diseases. During the Japanese colonial period, public hygiene was managed by the police and patients or suspected patients were forced into quarantine in a government-designated hospital. In an expert meeting before the 2nd amendment of the Prevention of Contagious Diseases Act in 1976, it was requested that instead of placing all the patients with infectious diseases under government control, they could instead be hospitalized in private general hospitals with wards for infectious diseases. From this we can infer that, in those days, it was possible to treat such patients in private hospitals without reporting them and instead of sending them to government-designated accommodation facilities. Since then, there have been multiple amendments to the Act, although they were only minor revisions. The Prevention of Contagious Diseases Act, which properly accommodates for domestic situations was promulgated in January 2000 [28]. Dysentery was categorized as a level 1 infectious disease, which are those that require immediate measures such as quarantine. In the present, the law stipulates that medical doctors, oriental medicine doctors, and directors of medical institutions who encounter patients with dysentery should immediately report back to the local healthcare center in writing, by fax or through the website communicable disease web report system(http://is.cdc.go.kr) [29]. Doctors, oriental medicine doctors, army surgeons, and medical institution directors who are found to act in a negligent way or give false reports or notifications will be fined up to two million won. Cases reported to the local healthcare center are integrated in the Centers for Disease Control and Prevention through a public health policy division in the relevant city of province. Public healthcare centers have to conduct a full epidemiological survey upon receiving the report of dysentery cases in order to identify the source of infection, to establish whether it is a case of a group outbreak, and to block transmission to other people through an appropriate control and management of patients, people in contact and the environment. Of particular importance is the need to determine whether it is a group outbreak in waterborne/foodborne diseases, such as dysentery. The epidemic determination criterion is when two or more communicable disease patients (including suspected cases) are epidemiologically related. If a group outbreak of dysentery is suspected, an epidemiological survey is conducted by forming a city/county/district, city/province or central epidemiological survey team depending on the scale of the outbreak. Patients with dysentery need to be isolated to prevent secondary transmission because Shigella can be isolated from the feces for a long time. The quarantine period set by the nation is up to the time when the result of 2nd feces culture test is negative upon the test in 24 hours interval after 48 hours have passed under antibiotics treatment. With economic development, overall hygiene habits have improved and so dysentery outbreaks are no longer a major problem. However, due to the nature of waterborne and foodborne infections, the possibility of a group outbreak is always present. In addition, the recent increase in imported multidrug-resistant Shigella requires continued monitoring and control of dysentery.
Go to :
 XML Download
XML Download