

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
For most high-risk hematologic malignancies, hematopoietic cell transplantation (HCT) has been the only curative method of treatment. The outcome of HCT is known to be best with matched related donors (MRDs), as the degree of human leukocyte antigen (HLA) match between the donor and the recipient correlates with the transplant outcome [12]. However, MRDs are available only for a proportion of HCT candidates [13]. For patients without a suitable MRD, the next preferred option is to use matched unrelated donors (MUDs), followed by partially-matched unrelated donors (PUDs), haploidentical familial donors (HIDs), or cord blood units (CB). One may naturally wonder how the transplant outcomes from these alternative donors compare across the different donor types.
Although HIDs have the advantage of almost universal and immediate donor availability [4], the early experience of HCTs from HIDs was complicated by the manifestation of a strong bidirectional alloreactivity, e.g., graft failure and graft-vs.-host disease (GVHD) [56]. These days, however, haploidentical HCTs have become increasingly popular with decades of efforts on better understanding of the immunologic mechanisms of HCT and developing measures to overcome the complications related to these [47]. Indeed, T-cell-replete HCTs from HIDs using anti-thymocyte globulin (ATG) have demonstrated similar survival and acceptable risk of other morbidities compared to those of matched donors [8].
The overall picture is positive for HIDs, but most of the previous studies have compared different donor types adopting different graft sources, intensity of conditioning, and GVHD prophylaxis platforms. In other words, the influence of these factors on transplant outcomes cannot be excluded when interpreting their results.
Thus, the aim of this study was to compare T-cell-replete HCT outcomes from HIDs with those from PUDs and MUDs in a homogenous population with acute leukemia or myelodysplastic syndrome (MDS) who used the same graft source of peripheral blood and a reduced intensity conditioning (RIC) regimen of busulfan, fludarabine, and ATG.
MATERIALS AND METHODS
Patient selection and treatment
We retrospectively identified and collected clinical data from 153 adult patients with a diagnosis of acute leukemia or MDS who had undergone their first HCT from an unrelated or haploidentical donor with a specified ATG-containing RIC regimen between February 2008 and March 2017, at Seoul National University Hospital (SNUH) and Seoul National University Bundang Hospital (SNUBH). The donors included 10/10 allele MUDs, 7/10 or 8–9/10 PUDs, or 3–4/6 or 3–7/8 or 6/10 allele HIDs. Peripheral blood stem cells were used as the graft source for all cases. Patients who received HCT from CB or bone marrow as the stem cell source were excluded for their infrequency at these institutions during the study period. Conditioning consisted of intravenous busulfan at a dose of 3.2 mg/kg on D-7 and D-6, fludarabine at 30 mg/m2 from D-7 to D-2, and rabbit ATG (thymoglobulin) at 3.0 mg/kg from D-3 to D-1. Cyclosporin A or tacrolimus, with or without methotrexate, was used in all patients to prevent GVHD. The type and dose of immunosuppressant, dose of ATG, and the choice to switch to another calcineurin inhibitor were at the discretion of the treating physician. Methotrexate was used at a dose of 15 mg/m2 for 2/3 d or at 15 mg/m2 2 or 3 days the first day followed by 10 mg/m2 for the next 2 d. The study protocol was reviewed and approved by the Institutional Review Board of SNUH and SNUBH, respectively.
Definition
Acute GVHD was diagnosed and graded clinically according to Glucksberg's criteria [9], and chronic GVHD according to the National Institutes of Health consensus criteria [10]. Relapse was defined by any evidence of the disease after HCT, and non-relapse mortality (NRM) was defined as death from any cause except relapse. The HCT comorbidity index (HCT-CI) was applied according to the previous study by Sorror et al. [11]. The disease risk index (DRI) consisted of disease and stage risk, each of which was derived from a diagnosis with the cytogenetics data and remission status at the time of HCT, respectively, and has been shown to successfully risk stratify heterogenous allogeneic transplant recipients [12]. For the present study, the DRI was collapsed to a 2-group system of low/intermediate and high/very high risk, as proposed by the original study [12].
Statistical endpoints included GVHD-free, relapse-free survival (GRFS), disease-free survival (DFS), and overall survival (OS). GRFS is a composite endpoint encompassing ongoing morbidity from GVHD in addition to relapse and death [1314]. GRFS events were defined grade III–IV acute GVHD chronic GVHD requiring systemic immunosuppressive treatment, relapse, or death. DFS was calculated as the time from HCT to relapse or death, and OS was defined as the time from HCT to death.
Statistical methods
Patient and treatment characteristics were compared with the chi-square test for categorical variables and one-way ANOVA for continuous variables. Survival curves were plotted using the Kaplan-Meier method and compared using the log-rank test. Cumulative incidence was estimated for individual failure events and compared using Gray's test, with death without GVHD being a competing risk for GVHD, relapse for NRM, and NRM for relapse. The Cox proportional hazards model was applied to identify risk factors significantly related to survival, in which variables with statistical significance from univariable analyses were subsequently used to construct multivariable analyses, along with the donor types. All P-values were two-sided and values of <0.05 were considered statistically significant. Statistical analyses were performed using two statistical software packages: SPSS version 23.0 (IBM Corp, Armonk, NY, USA) and R 3.5.1.
RESULTS
Baseline characteristics
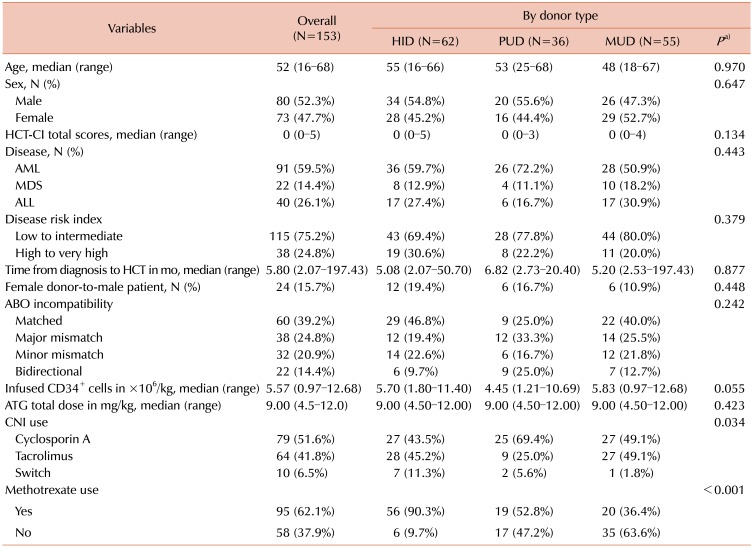
The characteristics of the included 153 patients are shown in Table 1. Overall, the median age of the recipients was 52 yr (range, 16–68) and 52.3% of the patients were males. Median HCT-CI scores were 0 in both overall and each of the three donor groups. The most common diagnosis was acute myeloid leukemia (AML, 59.5%), followed by acute lymphoblastic leukemia (ALL, 26.1%), and MDS (14.4%). DRI was low/intermediate in 75.2% and high/very high in 24.8% of the patients. Patients received HCT after a median of 5.80 months (range, 2.07–197.43 mo) from their diagnosis of hematologic malignancy, and approximately 15.7% of the cases consisted of a male recipient and a female donor. CD34+ cells were infused at a median dose of 5.57×106/kg (range, 0.97–12.68×106/kg), and the median total ATG dose was 9.00 mg/kg (range, 4.5–12.0 mg/kg). Although these characteristics were comparable among groups with different donor types, cyclosporin A was more frequently used, compared to tacrolimus, in the PUD group than in the HID and MUD groups, at 69.4% vs. 43.5% and 49.1%, respectively (P=0.034). Additionally, the proportion of patients who used methotrexate was higher in the HID group than in the PUD and MUD group, at 90.3% vs. 52.8% and 36.4%, respectively (P<0.001).
Estimate of survival
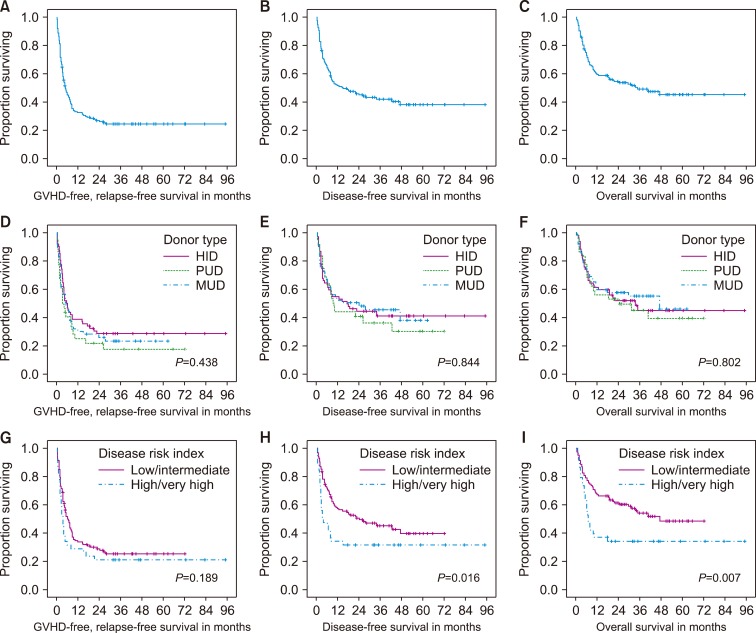
In the total population, the 3-yr GRFS, DFS, and OS rates were 24.3% [95% confidence interval (CI), 20.7–27.9%], 42.0% (95% CI, 37.8–46.2%), and 49.1% (95% CI, 44.7–53.5%), respectively (Fig 1A–C).
When grouped by donor type, the 3-yr GRFS rates were estimated to be 28.6% (95% CI, 22.8–34.4%), 17.5% (95% CI, 10.6–24.4%), and 23.2% (95% CI, 17.2–29.2%) for the HID, PUD, and MUD groups, respectively (Fig. 1D). The estimates of the DFS and OS rates at 3 yr were numerically higher in the MUD group than in the HID and PUD groups, with 45.5% (95% CI, 38.5–52.5%) vs. 41.2% (95% CI, 34.5–47.9%) and 36.3% (95% CI, 27.5–45.1%) for the DFS rates, and 55.1% (95% CI, 48.2–62.0%) vs. 44.9% (95% CI, 37.6–52.2%) and 44.9% (95% CI, 35.9–53.9%) for the OS rates, respectively (Fig. 1E, F). There was no significant difference in the curves for GRFS (P=0.438), DFS (P=0.844), and OS (P=0.802) among the three different donor types, based on log-rank tests (Fig. 1D–F).
When compared between groups with a different DRI, the 3-yr GRFS rates were estimated at 25.2% (95% CI, 20.9–29.5%) and 21.1% (95% CI, 14.5–27.7%) for the low/intermediate and high/very high groups, respectively. There was no significant difference between the curves for GRFS (P=0.189; Fig. 1G). In contrast, the DFS and OS curves differed by DRI groups (P=0.016 for DFS and 0.007 for OS; Fig. 1H, I). The estimates of the 3-yr DFS rates were 40.2% (95% CI, 40.2–50.2%) and 31.6% (95% CI, 24.1–39.1%) for the low/intermediate and high/very high groups, respectively (Fig. 1H). The 3-yr OS rates were 54.0% (95% CI, 48.8–59.2%) and 34.0% (95% CI, 26.3–41.7%) for the low/intermediate and high/very high groups, respectively (Fig. 1I).
Cumulative incidence of individual failure events
Grade III-IV acute GVHD was more frequently noted in the PUD group than in the other two groups, with a 100-d cumulative incidence of 19.4% (95% CI, 12.7–26.2%) vs. 8.1% (95% CI, 4.6–11.6%) and 9.1% (95% CI, 5.2–13.0%) for the PUD vs. HID and MUD groups, respectively (Fig. 2A). The incidence of chronic GVHD requiring systemic treatment was higher in the HID and MUD groups than in the PUD group, with a cumulative incidence of 34.3% (95% CI, 28.1–40.4%) and 25.9% (95% CI, 19.9–32.0%) vs. 17.6% (95% CI, 10.9–24.3%) at 3 yr, respectively (Fig. 2B). These differences in number, however, were not statistically significant (P=0.213 for acute GVHD; P=0.261 for chronic GVHD).
The cumulative incidence of relapse was similar among different donor types, with 34.4% (95% CI, 28.3–40.6%), 37.5% (95% CI, 28.4–46.5%), and 39.8% (95% CI, 32.8–46.7%) at 3 yr for HIDs, PUDs, and MUDs, respectively (P=0.920; Fig. 2C). NRM was not significantly different between the HID, PUD, and MUD groups, with 21.1% (95% CI, 15.9–26.4%), 29.5% (95% CI, 18.6–34.0%), and 14.7% (95% CI, 9.8–19.6) at 3 yr post-HCT, respectively (P=0.594; Fig. 2D). Relapse was observed later than 2 yr after HCT, whereas most NRM events in this study occurred within 1 yr after HCT.
Prognostic factor analysis for survival
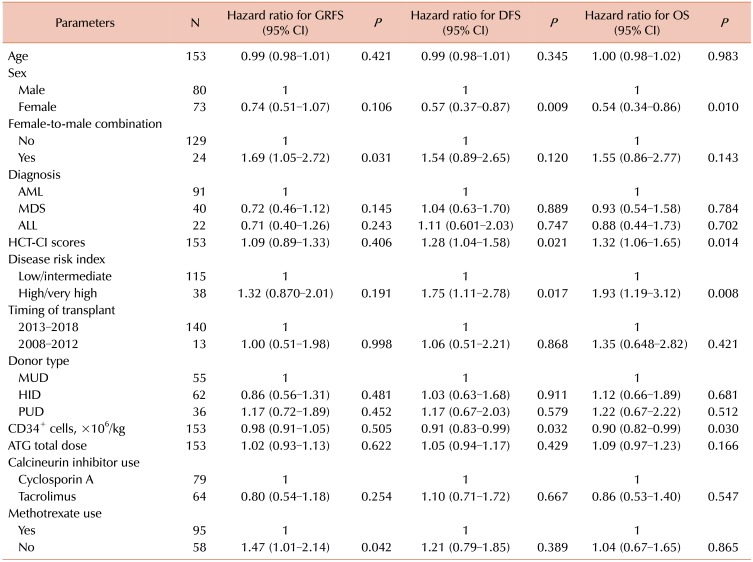
Of the clinical and treatment variables analyzed in univariable analyses, female donor-to-male recipient and no methotrexate use (vs. use) were associated with a significantly worse GRFS. Patient sex (female vs. male) and a higher dose of infused CD34+ cells were associated with a better DFS and OS, while higher HCT-CI scores and high/very high DRI (vs. low/intermediate) were associated with a worse DFS and OS (Table 2).
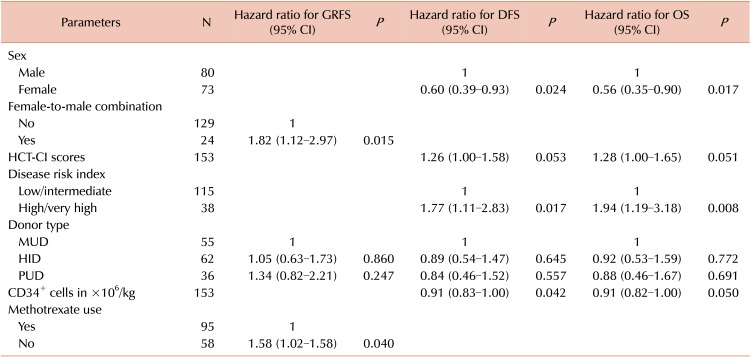
Subsequent multivariable analyses showed that female donor-to-male recipient and no methotrexate use (vs. use) were independently associated with a significantly worse GRFS, with a hazard ratio (HR) of 1.82 (95% CI, 1.12–2.97; P=0.015) and 1.58 (95% CI, 1.02–1.58; P=0.040), respectively. Patient sex (female vs. male) was associated with a better DFS and OS with an HR of 0.60 (95% CI, 0.39–0.93; P=0.024) for DFS and 0.56 (95% CI, 0.35–0.90; P=0.017) for OS. A high/very high (vs. low/intermediate) DRI was associated with a worse DFS and OS, with an HR of 1.77 (95% CI, 1.11–2.83; P=0.017) for DFS and 1.94 (95% CI, 1.19–3.18; P=0.008) for OS (Table 3). Donor type was not associated with survival in both univariable and multivariable analyses.
DISCUSSION
In this study, we found that GRFS, DFS, and OS were similar between HIDs, PUDs, and MUDs, but DFS and OS differed by patient sex and DRI in our cohort of HCT recipients with acute leukemia or MDS who used the same graft source of peripheral blood and the same RIC regimen of busulfan, fludarabine, and ATG. NRM tended to be higher with a mismatched donor than with a matched donor in this population, although without statistical significance.
Our estimates for alternative donor HCT for adult patients with acute leukemia closely followed those recently reported, based on a large registry of the European Society for Blood and Marrow Transplantation. Piemontese et al. [15] analyzed 3,568 recipients of alternative donor HCT from 2007 to 2013 for acute leukemia in their first or second remission. DFS and OS were longer with MUD than with HID and PUD, at 50% vs. 41% and 46% for 3-yr DFS rates and 56% vs. 46% and 48% for 3-yr OS rates. NRM at 3 yr was higher with HID and PUD than with MUD, at 29% and 29% vs. 21%, respectively. GRFS rates and relapse rates at 3 yr were similar among these donor types, at 33–36% and 25–30%, respectively [15].
Although our study was comparable to that of Piemontese et al. [15] to some extent, several differences make a direct comparison between these two studies difficult. Patients with advanced disease were not included, and myeloablative conditioning was given in more than half of the cases in the above-mentioned study. In addition, different graft sources and GVHD prophylaxis platforms were used according to different donor types, with HCT from HIDs adopting a higher proportion of bone marrow as the graft source and PTCy for GVHD prophylaxis.
With such diverse factors involved, heterogeneity has been inherent between studies on the outcome of allogeneic HCT. In this context, DRI was devised to risk-stratify recipients of allogeneic HCT by their disease type and status, the strongest determinants of survival in this setting, which was shown to be stable across different age groups, conditioning intensity, graft source, and donor type [1112]. McCurdy et al. [16] reported a risk-stratified outcome with HCT from HIDs using non-myeloablative conditioning and PTCy, as most cases used for the refinement of DRI were recipients of matched donor HCT. Low, intermediate, and high/very high groups demonstrated 65%, 37%, and 22% for the DFS rate at 3 yr and 71%, 48%, and 35% for the OS rate at 3-yr, respectively, which were generally comparable to ours as well.
Notably, female recipients had better DFS and OS than male recipients in multivariable analyses in the present study. These results are similar to those reported by Kim et al. [17], who evaluated data from 11,797 patients transplanted from 2008 to 2010 to see how recipient-donor sex affected the outcome. They found that male recipients had worse OS and PFS compared to female recipient independent of donor sex, and that male recipients with female donors were associated with increased NRM and chronic GVHD. The latter finding is similar to that in the present study—female-to-male combination exhibited a significantly worse GRFS.
ATG is one of the two main platforms for GVHD prophylaxis along with PTCy. It has been shown to be protective against GVHD in HCT from MUDs [18] and MSDs [19] and has been successfully incorporated into protocols for T-cell replete HCT from HIDs [82021]. Among these, RIC with busulfan, fludarabine, and ATG for HCT from HIDs has shown promising results in terms of consistent engraftment and low rates of GVHD and NRM [2223].
Interestingly, the frequencies of acute GVHD of grade III–IV and chronic GVHD requiring systemic therapy were numerically higher and lower in the PUD group than in the HID and MUD groups, respectively, but the difference was not statistically significant. Raiola et al. [24] noted a more frequent occurrence of acute GVHD of grade III–IV with PUDs than with MUDs and HIDs in a heterogenous population with various hematologic malignancies. Two recent large studies, in contrast, found no difference in the incidence of acute GVHD among PUDs, MUDs, and HIDs in a population with acute leukemia [1525]. A future prospective trial is needed to confirm whether the risk of acute GVHD is higher with HCT from PUDs than from other donor types.
Our study has several limitations. First, the retrospective nature of the study and limited number of patients included may render this analysis hypothesis-generating at most and subtle differences likely went unnoticed. Second, the follow-up period of the study population was relatively short, and the long-term effect of the treatment remains to be evaluated. Finally, the present study did not address a different dosage of ATG, however previous reports have suggested that different doses of ATG have a differential impact on the outcome [26]. Despite these limitations, the study population was highly homogenous, in terms of conditioning regimen and use of peripheral blood as graft source, which enabled us to compare different donor types independent of these confounders.
In conclusion, the present study suggests that T-cell replete HCT from HIDs using an ATG-containing RIC regimen may be a reasonable option in the absence of MRDs in patients with acute leukemia or MDS.

 XML Download
XML Download