

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
The classification system developed by Yannuzzi et al. [1] indicates that type 1 idiopathic macular telangiectasia (IMT) is an aneurysmal telangiectasia and a form of Coats' disease that involves the macula. Type 1 IMT is unilateral, predominantly occurs in middle-aged men, and is typically located in the temporal half of the macula. The therapeutic options for type 1 IMT include laser photocoagulation and intravitreal injections of triamcinolone acetonide (IVTA) or anti-vascular endothelial growth factor (VEGF) [2]. Nondamaging retinal laser therapy with a micropulse laser recently has emerged as a promising treatment option for other macular diseases, including type 2 IMT [3]. We report a case of 577 nm subthreshold micropulse yellow laser (SMYL) treatment for macular edema of type 1 IMT that was nonresponsive to intravitreal injections, with a 4-year follow-up period.
A 54-year-old man presented with decreased central vision in the left eye that had persisted for 2 years. On examination, his best-corrected visual acuity was 20 / 800 in the left eye and 20 / 20 in the right eye. He had received 2 intravitreal injections of bevacizumab in his left eye at another clinic. Fundus examination of the left eye showed multiple dot hemorrhages and circinate hard exudates in the macula. Fluorescein angiography showed extensive juxtafoveal capillary telangiectasia and aneurysms. Spectral domain optical coherence tomography showed severe cystoid macular edema (CME) (Fig. 1A). He was diagnosed with type 1 IMT and received IVTA, but the treatment was ineffective. Thus, we administered 577 nm SMYL (Supra Scan, Quantel Medical, Cedex, France) around the juxtafoveal telangiectatic area with the following settings: 120-µm spot diameter, 20-ms duration, 15% duty cycle, 3 × 3 matrix pattern (0.5 widths), and low power, ranging from 200 to 400 mW with monthly increases in 100 mW increments, based on the response to treatment [4]. We performed a SMYL (200 and 300 mW) session for 2 months (for a total of 2 treatment sessions). Dot hemorrhages, circinate hard exudates, and intraretinal cysts were diminished for 9 months posttreatment (Fig. 1B). However, CME recurred 11 months after SMYL, and aneurysms and telangiectatic vessels were observed in the temporal parafoveal area (Fig. 1C). We performed the third SMYL treatment with 300 mW power, which was the previously determined effective threshold, around the entire macular area; SMYL was repeatedly applied to a large temporal aneurysm that was considered the main leakage point. There was no visible laser burn immediately after the third SMYL. One month after the last treatment, Spectral domain optical coherence tomography showed CME resolution and no definite retinal damage in the macula (Fig. 1D). For 3 years after the third SMYL, the patient's left eye remained stable, and best-corrected visual acuity improved to 20 / 40. However, in the large aneurysmal area that was repeatedly treated, progressive focal atrophic change developed approximately 1 year after the third SMYL treatment (Fig. 1E).
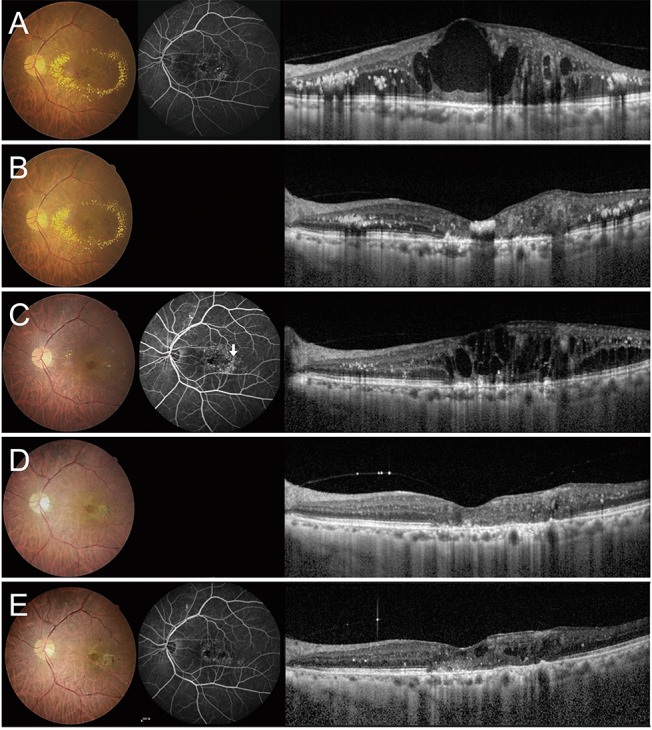 | Fig. 1Serial fundus photography, fluorescein angiography (FA), and spectral domain optical coherence tomography (SD-OCT) of the left eye. (A) Initial fundus photograph shows multiple aneurysmal capillary dilatations and large circinate hard exudates. FA shows aneurysmal telangiectasia in the juxtafoveal area. SD-OCT shows cystoid macular edema (CME). (B) After 2 applications of subthreshold micropulse yellow laser (SMYL), fundus photography shows resolution of aneurysms and exudates. SD-OCT shows improved CME. (C) Hard exudates are not seen on fundus photography, but FA shows aneurysms and telangiectatic vessels in the temporal parafoveal area (arrow) at 11 months after SMYL. SD-OCT shows recurrent CME. (D) At 1 month after the third SMYL treatment, there is no definite retinal damage on fundus photography, and the SD-OCT shows CME resolution. (E) Crystalline deposits and a few new aneurysms are seen on fundus photography. Retinal atrophy at the temporal macula is seen in the area of ablative laser application. SD-OCT shows improved CME but mild cystic changes.
|
Treatment options for type 1 IMT include laser photocoagulation and intravitreal injection of anti-VEGF or triamcinolone. Intravitreal injections of anti-VEGF and triamcinolone acetonide have proven beneficial for treating macular edema due to anti-inf lammatory effects, down-regulation of VEGF production, and stabilization of the blood-retinal barrier [2]. Our patient was treated with 2 injections of intravitreal bevacizumab and 1 of IVTA, without therapeutic effect. Therefore, aflibercept, which blocks both VEGF-A and placental growth factor, may be more effective in type 1 IMT than other anti-VEGFs and could be another treatment option in drug-resistant cases [5]. Laser photocoagulation remains most effective in type 1 IMT, but conventional photocoagulation produces thermal damage to photoreceptors of the inner retina, which is unacceptable near the fovea [2]. Thus, we applied SMYL, a type of nondamaging retinal laser therapy that raises the temperature of the RPE to just below the threshold for protein denaturation, thereby preventing retinal damage.
This case report with a 4-year follow-up period shows that SMYL may be effective in the CME of type 1 IMT, especially in cases that do not respond to intravitreal injections. In this case, definite retinal damage did not develop in most of the SMYL-treated area after 3 treatments, but progressive focal atrophic change developed over time. The atrophic change could have been the result of long-standing CME but could also have been triggered by repeated SMYL applications. Based on these results, additional cases are needed to evaluate the effectiveness and safety of SMYL for type 1 IMT and to develop detailed SMYL treatment guidelines to prevent retinal damage.
 XML Download
XML Download