

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a frequently overlooked, serious disorder1. Its incidence is increasing according to recent reports in western countries and in Korea234.
There are various well-defined risk factors of VTE, including recent major surgery, immobilization, cancer, old age, obesity, use of oral contraceptives, hormonal factors, a previous history of thrombosis, and inherited risk factors 56. In addition to known risk factors, infectious disease and the associated systemic inflammatory response may increase thrombotic events of the venous system78 caused by one or more of the three precipitants of venous thrombosis, as proposed by Virchow: venous stasis, hypercoagulability, and endothelial damage 910. Several reports have documented that the risk of VTE was increased in patients with certain infectious conditions, such as cytomegalovirus, Chlamydia pneumoniae, human immunodeficiency virus (HIV), hepatitis C virus infection, and a recent respiratory tract infection1112131415161718. Despite several reports of recent infection and VTE, its independent relationship is unclear, and clinical data regarding PE combined with infectious conditions are lacking. Therefore, the aim of the study was to evaluate the clinical characteristics and source of infection in patients with PE combined with infectious disease. And, the risk factor associated with combined infectious disease and its influence on mortality in patients with PE were assessed.
Go to : 
Materials and methods
1. Study design and population
Patients with PE found on computed tomography (CT) within 48 hours after admission were enrolled in this study. The study was conducted at regional university affiliated hospital (890 beds) between September 2010 and May 2014. Patients were excluded if they were admitted for pregnancy, preexisting PE or DVT, or were <18 years of age. The diagnosis of PE was confirmed based on chest findings obtained using a 64-detector CT, including enhanced CT and CT pulmonary angiogram, scanner (Brilliance-64; Philips Medical Systems, Eindhoven, Netherlands). A pulmonary radiologist assessed the existence of thrombosis in the pulmonary artery. This study was approved by the hospital's institutional review board (No. GNUCH-2018-07-001). The need for informed consent was waived because of the retrospective nature of the study.
2. Data collection and clinical outcomes
We retrospectively investigated patients' demographics, physiologic data, and laboratory data and the causes of infection, underlying diseases, and clinical outcomes. We divided patients into one of two groups based on information obtained from their medical charts: patients with PE combined with infectious disease or those with PE without infection. Patients' characteristics were compared between those two groups, and between survivors and non-survivors. Finally, we analyzed the risk factors associated with combined infectious disease in PE patients and compared mortality between those two groups. And we assessed the factor associated non-survivors in patients with PE.
3. Definition
The definition of infection was based on microbiologic data and the patient's clinical course upon medical chart review. Infection was classified according to the Centers for Disease Control and Prevention's definitions19.
4. Statistical analysis
Continuous variables are reported as the mean±standard deviation. Categorical variables are expressed as a number (%). Differences between the groups were statistically assessed using Student's t test or the chi-square test, as appropriate. Univariate and multivariate logistic regression analyses were performed to examine the risk factors for the development of infectious disease and mortality. A p-value of <0.05 was considered statistically significant in all tests. All data were analyzed using SPSS version 22.0 for Window (IBM Corp., Armonk, NY, USA).
Go to :
Results
1. Patients' characteristics
Two hundred fifty-eight patients (male:female, 143:115; mean age, 68.2±13.0 years) were included. The most common symptom was dyspnea in up to 60% of patients, and 70 patients (26.9%) were asymptomatic. Twenty patients (7.7%) had a previous history of VTE, and 145 (55.8%) had an underlying malignant disease. One hundred seventy-one patients (65.8%) were older than 65 years, and 13 (5%) had a body mass index more than 30 kg/m2. Fifty-eight patients (22.3%) showed echocardiographic evidence of pulmonary hypertension, such as right ventricular hypokinesia or an increased pulmonary arterial pressure more than 20 mm Hg. The main pulmonary artery was involved in 88 patients (33.8%) based on CT findings. Thirty-seven patients (14.2%) died and the cause of death were underlying malignant disease in 27 patients (10.4%), uncontrolled infectious disease with multiorgan failure in six patients (2.3%), progression of underlying lung disease in three patients (1.1%), and heart failure in one patient (Table 1). Overall, 67 patients (25.9%) had a concomitant infectious disease. The infections involved the respiratory tract in 52 patients (77.6%), genitourinary tract in three (4.5%), hepatobiliary tract in three (4.5%), gastrointestinal tract in two (2.98%), bones and joints in three (4.5%), and other organ systems in four (5.4%) (Table 2).
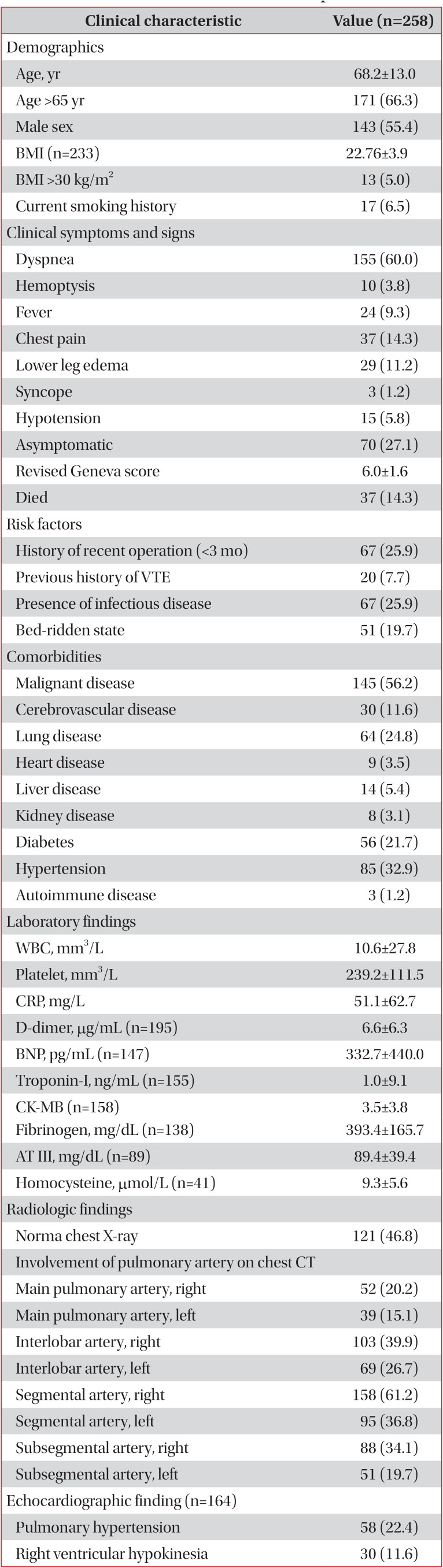
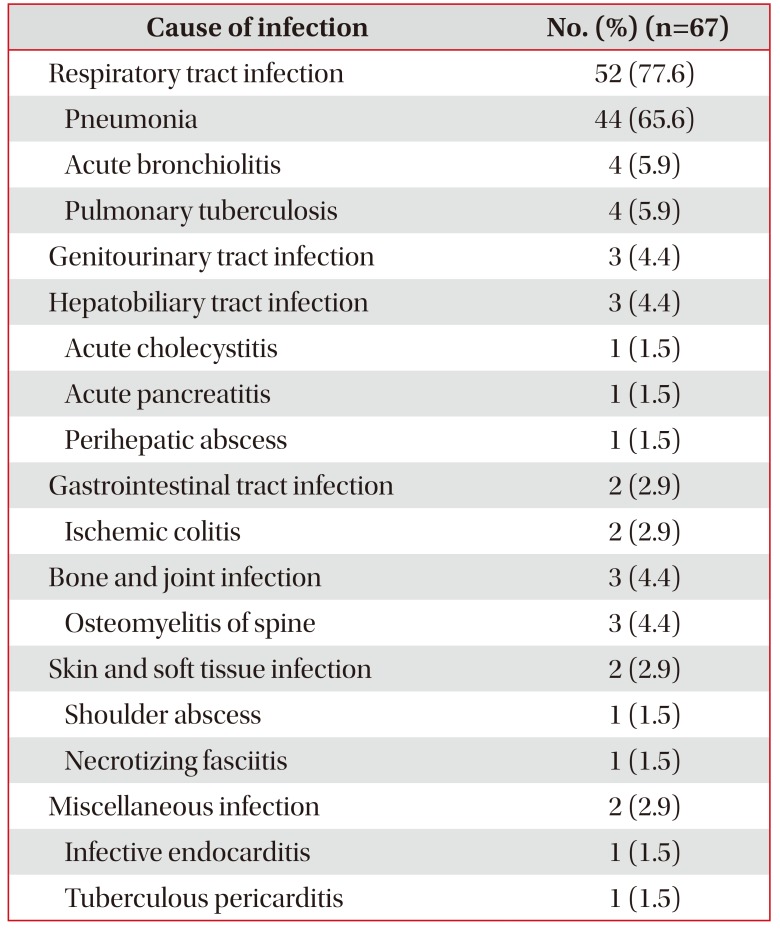
Table 1
Clinical characteristics of enrolled patients with PE
![]()
Table 2
The site and cause of infection in patients with pulmonary embolism combined with infectious disease
![]()
2. Comparison of clinical characteristics in PE patients with infectious disease and without infection
The proportion of patients with dyspnea was greater among patients with PE combined with infectious disease than among those with PE without infection (76.1% vs. 53.9%, p<0.05). The frequency of fever was more common in patients with PE combined with infectious disease than in those with PE without infection (17.9% vs. 6.2%, p<0.05). The proportion of patients older than 65 years was higher among patients with PE combined with infectious disease than among those with PE without infection (77.6% vs. 61.7%, p<0.05). The revised Geneva score20 was not different between the two groups. The white blood cell count, serum C-reactive protein level, B-type natriuretic peptide level, and platelet count were significantly higher in patients with PE combined with infectious disease than in those with PE without underlying infection (p<0.05). The D-dimer level was not significantly different between two groups. The frequency of main pulmonary artery involvement based on CT findings was not different between PE patients with infectious disease and without infection (28% and 22.4%, respectively). The sole segmental or subsegmental pulmonary artery involvement was also not different between PE patients with infectious disease and without infection (48.7% and 55.2%, respectively). In-hospital mortality was higher in patients with PE combined with infectious disease than in those with PE without infection (22.4% vs. 11.4%, p=0.006) (Table 3).
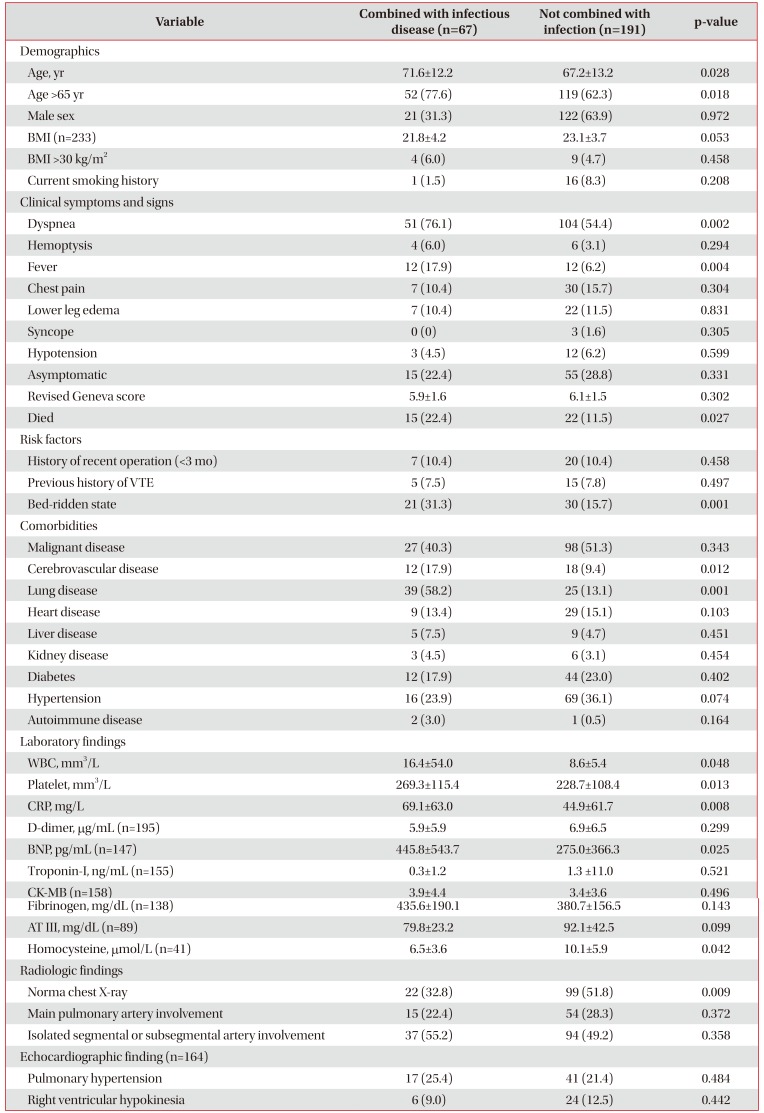
Table 3
Comparison of clinical characteristics in patients with PE combined with infectious disease and in patients with PE without infection
![]()
3. Factors associated with PE combined with infectious disease
In multivariate analysis, the results showed that underlying lung disease (odds ratio [OR], 3.69; 95% confidence interval [CI], 1.926–7.081; p<0.001), bed-ridden state (OR, 2.84; 95% CI, 1.390–5.811; p=0.004), and malignant disease (OR, 1.867; 95% CI, 1.017–3.425; p=0.044) were associated with combined infectious disease in patients with PE (Table 4).
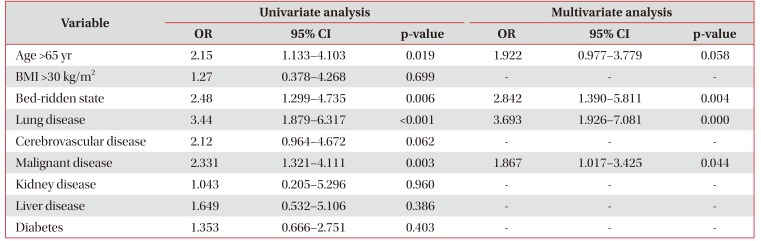
Table 4
Factor associated with infectious disease in patients with PE
![]()
4. Comparison of clinical characteristics between survivors and non-survivors in patients with PE
The clinical characteristics and laboratory findings were compared between survivors and non-survivors in patients with PE (Table 5). The mean age and proportion of patients older than 65 years were higher in non-survivors than in survivors (p<0.05). Clinical symptoms and signs were not different between the two groups. Bed-ridden state, underlying malignant and cerebrovascular diseases were more common in non-survivors than in survivors (p<0.05). Combined infectious diseases were also common in non-survivors than in survivors (44.7% vs. 23.4%, p<0.05). The troponin-I were higher in non-survivors than in survivors (p<0.05). Radiologically, main pulmonary artery involvement was more common in non-survivors than in survivors (43.2% vs. 23.8%, p<0.05). Right ventricular hypokinesia detected by echocardiography was also more common in non-survivors than in survivors (21.6% vs. 9.9%, p<0.05).
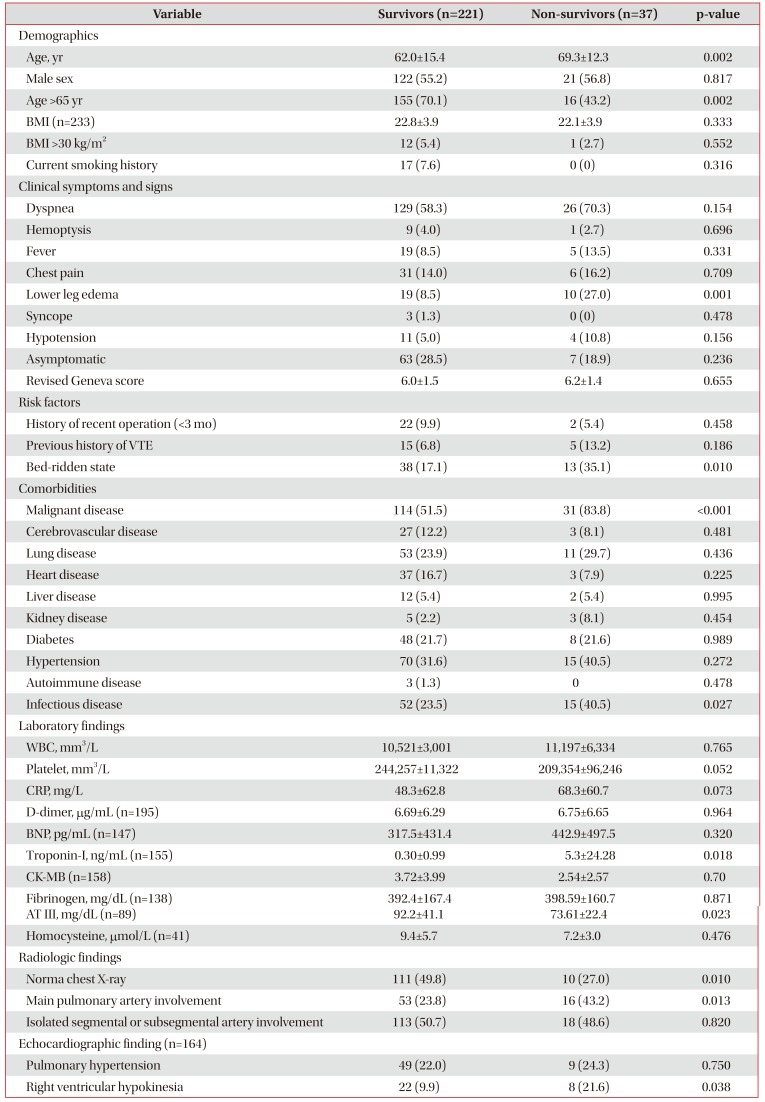
Table 5
Comparison of clinical characteristics between survivors and non-survivors in patients with PE
![]()
5. Factors associated with non-survivors in patients with PE
In multivariate analysis, the result showed that age >65 years (OR, 2.575; 95% CI, 1.125–5.892; p=0.025), bed-ridden state (OR, 3.487; 95% CI, 1.397–8.703; p=0.007), malignant disease (OR, 9.275; 95% CI, 3.181–27.040; p<0.001), main pulmonary artery involvement (OR, 3.032; 95% CI, 1.283–7.162; p=0.011), and concomitant infectious disease (OR, 4.189; 95% CI, 1.692–10.372; p=0.002) were associated with non-survivors in patients of PE (Table 6).
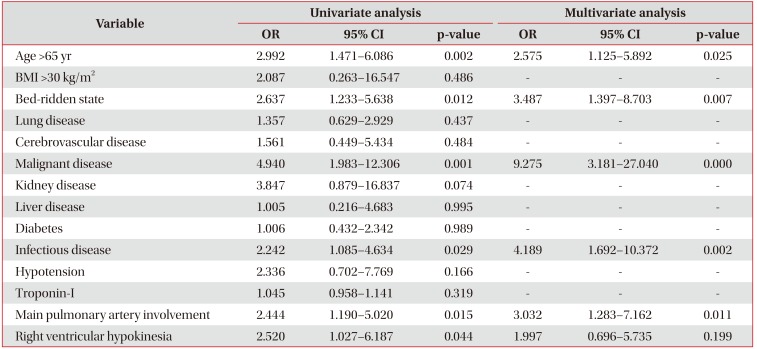
Table 6
Factors associated with non-survivors in patients with PE
![]()
Go to :
Discussion
This study showed that a substantial portion of patients with PE had concomitant infectious disease. The underlying lung disease, bed-ridden state and malignant disease were independent risk factor for PE with combined infectious disease and presence of infectious disease may contribute mortality in patients with PE.
Several reports have shown that various infectious conditions were associated with the development of VTE, and overall, 11%–26% of patients with VTE may have an underlying acute infectious conditions2122232425. For example, cytomegalovirus antigen positivity was significantly higher in patients with VTE than in age-matched and sex-matched controls13. Additionally, in 312,147 patients with inflammatory bowel disease, the presence of VTE was 2-fold higher in patients with Clostridium difficile infection (CDI) than in those without CDI26. It has been also demonstrated that HIV infection and hepatitis virus infection are associated with an increased risk of VTE1112. In a review of a primary care database of 11,557 cases of first-time PE or VTE, Clayton et al.27 reported that a preceding respiratory infection may increase the risk of PE or VTE by more than 2.5-folds for up to a year. A prospective study of 5,451 patients with ultrasound-confirmed DVT showed that beside known risk factors, osteoarthritis, pneumonia, sepsis, and other infectious diseases were present in more than 30% of patients1. In addition, in acutely ill, hospitalized, general medical patients, the presence of acute infectious diseases was significantly associated with an increased risk of VTE (relative risk, 1.47)24. Moreover, the epidemiologic study, a case control study involving patients with a first documented VTE and controls subjects, influenza vaccination during the previous 12 months reduced the risk of VTE by about 50% in those younger than 52 years and had a similar effect on DVT and PE28. Further, when heparin was routinely administered in hospital-admitted patients with underlying infectious disease, the occurrence of non-thromboembolic events was significantly lower in these patients with various infectious diseases than in control patients with infectious diseases22.
However, it is unclear whether the infection itself increases the risk of developing VTE or whether secondary problems, such as immobility caused by infection, increase the incidence of VTE. Although the mechanism was not elucidated here, there are possible explanations for the mechanism underlying infection and VTE. Acute infectious processes may cause endothelial injury, promoting the genesis of thrombosis in the venous system, which is usually much more vulnerable to stasis than is arterial blood. From experimental study, endothelial dysfunction in vein of healthy volunteer exposed to endotoxin may increase the risk of developing cardiovascular thromboticevent10.
Respiratory tract infection was the most common cause of infection in the present study. Cohoon et al.29 reported that genitourinary and lower respiratory tract infection was the most common infections in their study. They also reported a relatively higher risk of VTE in intra-abdominal infection and blood stream infection. This is a reason why patients with lower respiratory tract infection often undergo chest CT for evaluation of the disease. Thus, PE may be detected incidentally by chest CT. The increasing incidence of chest CT is often correlated with an increasing incidence of PE, indicating that PE is incidentally detected by chest CT 3031. In this study, over two-thirds patients were diagnosed in chest CT, not embolism CT. It may indicate that PE is incidentally detected in clinical practice.
As expected, patients with PE combined with infectious conditions had a poor outcome, resulting in a higher mortality in these patients. This has not been reported previously. Other factors associated with an increased risk of mortality, such as older age, malignant disease, right ventricular dysfunction, and immobilization 3233, were similar to those identified in our study. Additionally, main pulmonary artery involvement is associated with a poor short-term outcome in patients with PE34.
This study has a several limitations. First, because of the study's retrospective design, infectious disease could not be clearly classified based on the medial record review and the exact incidence of infectious disease couldn't estimate from this study in all PE patients. Second, some proportion of patients with PE was incidentally detected by chest CT for evaluating respiratory tract infection. So, other infectious disease like intraabdominal and genitourinary tract infection may be underestimated. Third, most of patients had a severe underlying disease which may significantly contribute mortality in these patients. The adjustment of severe underlying disease needed to exact contribution of infectious disease to mortality in patients with PE.
Go to :
 XML Download
XML Download