

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gastric cancer (GC) is the world's most common malignant disease and among the leading causes of cancer mortality [1]. Radical gastrectomy with lymph node dissection is currently the only potentially curative treatment method for patients with resectable GC [2]. Laparoscopic gastrectomy combined with lymph node dissection has become the preferred treatment for early GC [34]. Recent large multicenter randomized clinical trials have demonstrated that laparoscopic gastrectomy is both safe and effective for the treatment of advanced GC [567].
Although the complications and mortality rates of laparoscopic gastrectomy have been very low with improvements in surgical techniques, periprocedural complications must be monitored [89]. Duodenal stump leakage (DSL), one of the most serious complications during gastrectomy, is a rare complication with up to 20% mortality rate [10]. DSL mainly occurs in patients undergoing Billroth II (B-II) and Roux-en-Y (R-Y) reconstructions in which a duodenal stump exists. Due to the higher requirements inherent to laparoscopic surgeries, difficulty persists regarding duodenal stump management and no consensual agreement has been reached regarding it in laparoscopic gastrectomy for GC.
Some studies stated that laparoscopic surgery would increase the incidence of DSL, therefore reinforcing that the duodenal stump can reduce DSL occurrence [11]. In contrast, most researchers believe that routine duodenal stump reinforcement was not necessary for gastrectomy [121314]. A recent study of 965 patients from Japan showed that laparoscopic duodenal stump reinforcement reduced the incidence of DSL during R-Y reconstruction [15]. However, the study was limited to patients with early GC, and 70 patients had an unreinforced duodenal stump. Furthermore, reconstruction was limited to R-Y, as B-II was rarely performed in Japan. Therefore, this study lacked guiding significance by not including advanced GC and is not relevant for locations that perform B-II of reconstruction. Therefore, our study further investigated the risk factors of DSL after laparoscopic radical gastrectomy for GC and included patients with advanced GC and both reconstruction methods R-Y and B-II (B-II with Braun).
Go to : 
MATERIALS AND METHODS
Study population
The data of all patients diagnosed with GC who underwent laparoscopic gastrectomy with R-Y or B-II with Braun reconstruction between January 2013 and December 2018 at Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, and between January 2014 and December 2018 at HwaMei Hospital, University of Chinese Academy of Sciences, were extracted from a prospectively collected database and retrospectively analyzed in this study. The inclusion criteria were 1) with histologically proven primary gastric adenocarcinoma; 2) no history of gastrectomy or other malignant tumor; 3) pathologically negative resection margins (R0 resection) and lymphadenectomy (D1+ or more); and 4) no combined viscera resection. This study was approved by the research Ethics Committee of Zhejiang University School of Medicine Sir Run Run Shaw Hospital and HwaMei Hospital, University of Chinese Academy of Sciences (NO.PJ-SRRSH-KY-2019-1-21-21 and NO.PJ-NBEY-KY-2019-032-15).
Surgical procedures
According to the Japanese Gastric Cancer Association guidelines, all patients underwent radical gastrectomy with lymphadenectomy (D1+ or D2–3) [16]. The duodenal stump was cut to about 2 cm long using a linear stapler. In the unreinforced group, no additional treatment was performed of the duodenal stump. In the reinforcement group, the duodenal stump was reinforced using several different methods, including continuous suture, interrupted suture, semi-pouch suture, and complete-pouch suture under laparoscopy, with all suturing performed by hand. The suture depth included the full or seromuscular layer. One or two abdominal drainage tubes were routinely left in the abdominal cavity after surgery [13171819].
Surgical complications
DSL was defined as follows: presence of fluid in the surgical abdominal drain or after radiological drainage with at least 3 times higher bilirubin or amylase concentrations than normal serum value; or leakage through the abdominal wall regardless of its clinical impact confirmed by abdomen computed tomography (CT) and/or fistulography [20]. Complications were identified when they occurred in the first 30 days after surgery or during the postoperative hospital stay. The severity of surgical complications was evaluated according to Clavien-Dindo classification (C-D). Complications of C-D grade 3a and above were considered events [21].
Statistical analysis
Continuous data are presented as mean and standard deviation or median and range, while categorical data are presented as percentages. The potentially relevant factors obtained from the univariate analysis were assessed in the multivariate model using logistic regression. Odds ratios (OR) and 95% confidence intervals (CIs) were calculated. All statistical tests were performed 2-sided, and values of P<0.05 were considered statistically significant. The analyses were performed using SPSS software (version 25.0; SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
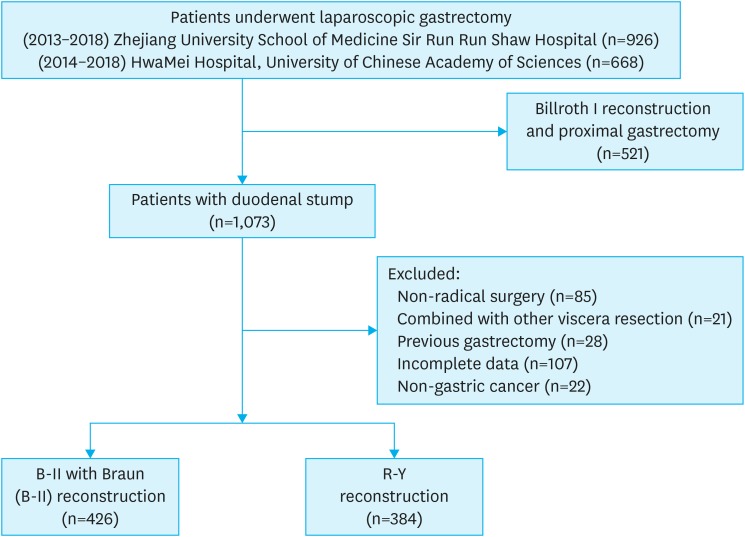
From January 2013 to December 2018, 926 patients underwent laparoscopic gastrectomy at Zhejiang University School of Medicine Sir Run Shaw Hospital, and from January 2014 to December 2018, 668 patients underwent laparoscopic gastrectomy at HwaMei Hospital, University of Chinese Academy of Sciences. Among them, a total of 784 patients were excluded according to the inclusion criteria. Finally, 810 patients were eligible for the analysis (426 patients with R-Y, 384 patients with B-II with Braun) (Fig. 1).
Regarding clinical features, there were more than twice as many males as females, and the vast majority (94%) of patients were American Society of Anesthesiologists (ASA) grade 1–2. Approximately one-third (26.8%) of the patients were overweight or obese, while one-third had (32.2%) varying degrees of anemia. Analysis of the surgical procedure was as follows: patients with distal gastrectomy and total gastrectomy were comparable, and the most common methods of reconstruction were R-Y and B-II with Braun. The median operation time was about 4 hours and the median blood loss was 70 mL. Of the cohort, 527 (65.1%) received duodenal stump reinforcement, while the remaining 283 patients did not receive duodenal stump reinforcement. Additionally, two-thirds of the patients had advanced GC (stages II–IIII) (Table 1).
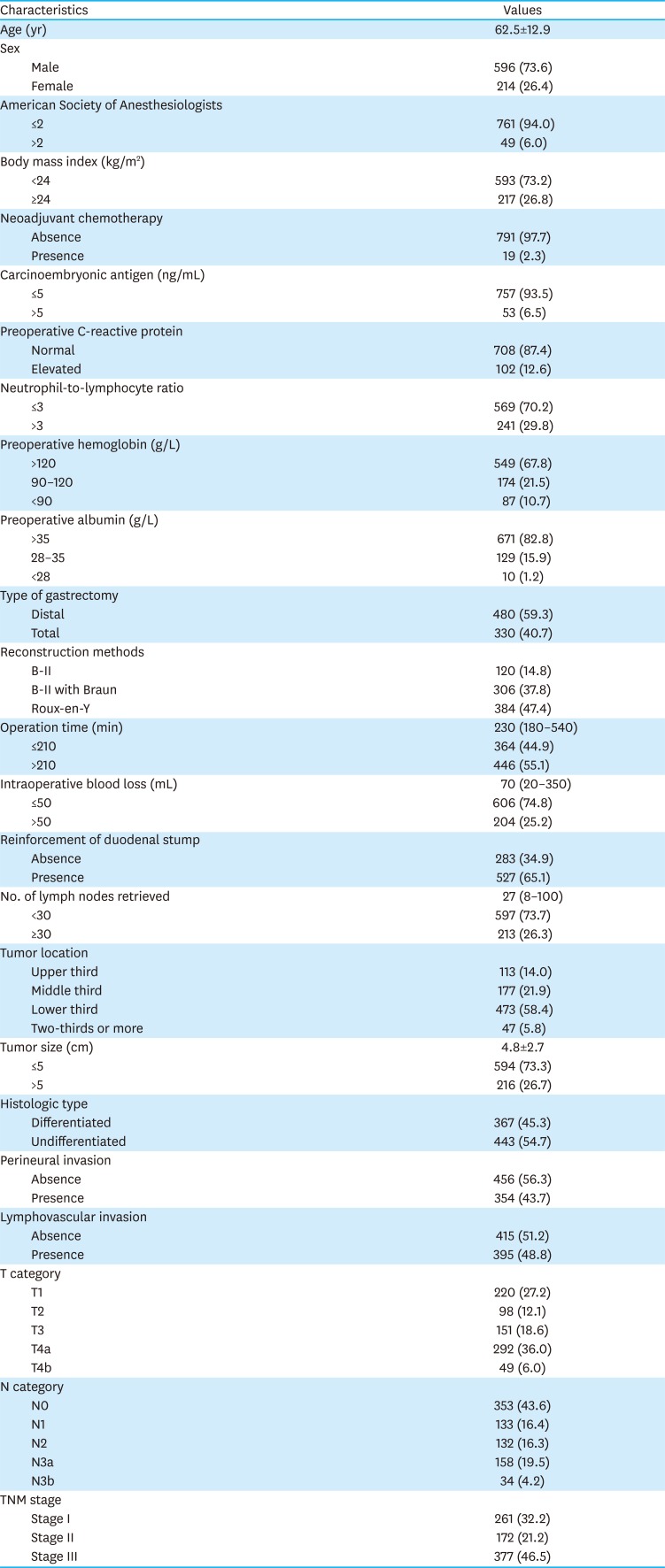
Table 1
Baseline clinicopathological characteristics
![]()
Surgical complications
Complications of C-D grade 3–5 occurred in 90 patients (11.1%), including grade 3a in 73 cases, grade 3b in 13 cases, grade 4 in 2 cases, and grade 5 in 2 cases. Pulmonary complications occurred in 44 patients (5.4%). Other complications included anastomosis or stump leakage (n = 14), intestinal obstruction (n = 10), intra-abdominal abscess (n = 9), postoperative bleeding (n = 6), wound complications (n = 4), pancreatitis (n = 2), and cerebral infarction (n = 1). One patient died of a systemic infection secondary to an intra-abdominal abscess, while another died of respiratory failure. The overall mortality rate was 0.25%.
Risk factors for DSL
A total of 11 patients with DSL (1.36%) were observed. Twenty-four variable parameters were analyzed. On the univariate analysis, the following 5 clinicopathological characteristics were demonstrated to be potentially associated with DSL: body mass index (BMI), preoperative C-reactive protein (CRP), preoperative albumin, reinforcement of the duodenal stump, and T stage (Table 2). The multivariate Cox proportional hazards model analysis showed that BMI, preoperative CRP, and reinforcement of the duodenal stump were the most important independent risk factors for DSL (Table 3). The incidence of DSL was 2.8% in overweight or obese patients versus 0.8% in patients with a BMI <24 kg/m2. The rate of DSL was 0.8% in patients with normal CRP and 4.9% in patients with an elevated CRP (>6 mg/L). The DSL incidence in the duodenal stump reinforcement and unreinforced groups was 0.6% and 2.8%, respectively.
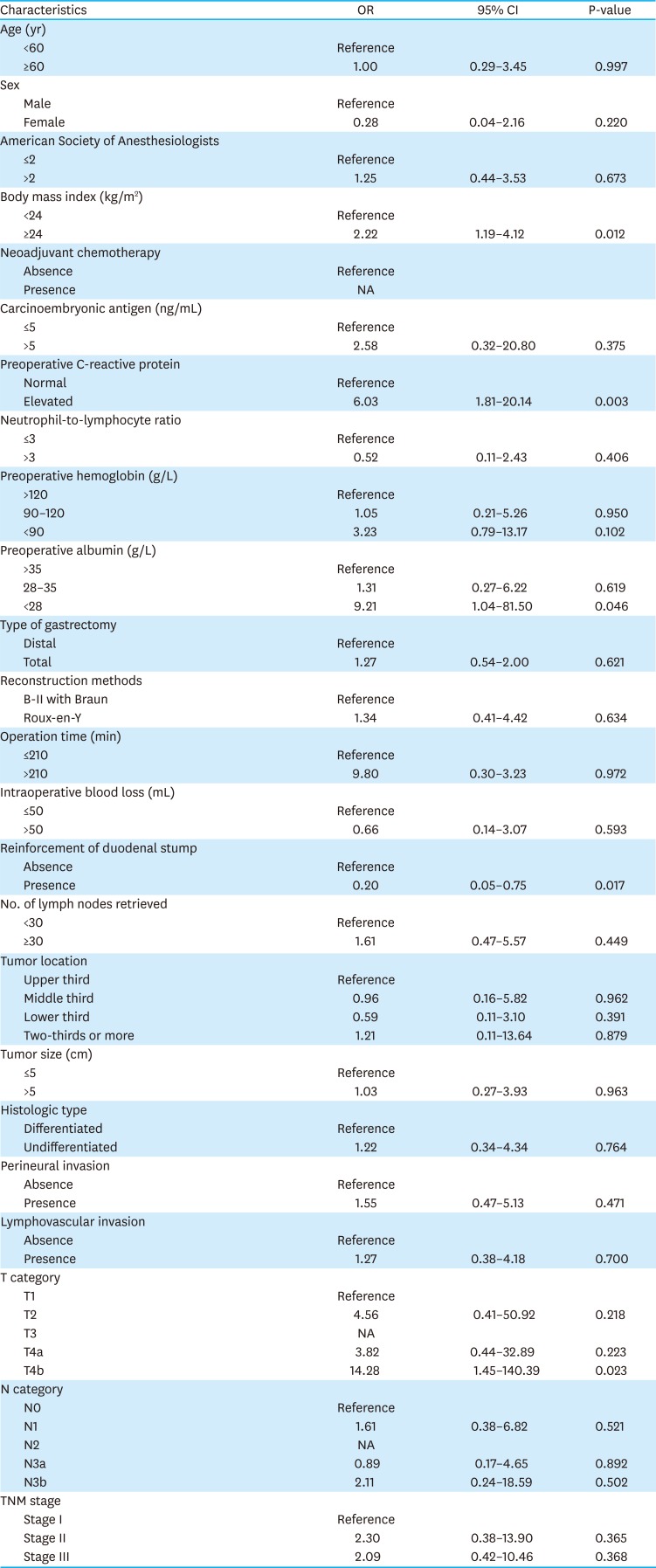
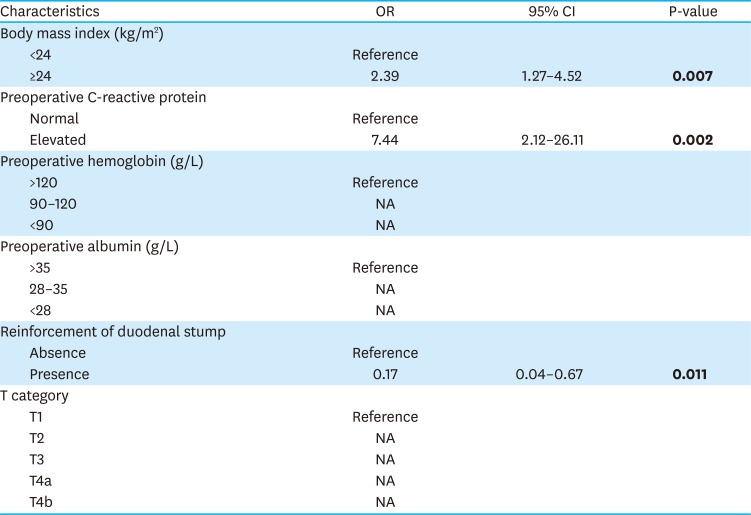
Table 2
Univariate analysis of risk factors for duodenal stump leakage
![]()
Table 3
Multivariate analysis of risk factors for duodenal stump leakage
OR = odds ratio; CI = confidence interval; NA = not available.
Bold words on behalf of the difference is statistically significant (p<0.05).
![]()
Details of patients with DSL
Among the patients with DSL, 10 were male and one was female. One patient had an ASA of 3 and the rest were ASA 1–2. The mean BMI was 23.9 kg/m2; 6 patients were overweight or obese (BMI >24 kg/m2). CRP was elevated in 5 patients before surgery. The duodenal stump was not reinforced in 8 cases. DSL was diagnosed in 2–12 days, with a median of 8 days. Seven patients received conservative treatment, 3 received puncture treatment, and 1 underwent reoperation. All patients recovered after treatment. The average postoperative hospitalization stay was 21 days (Table 4).
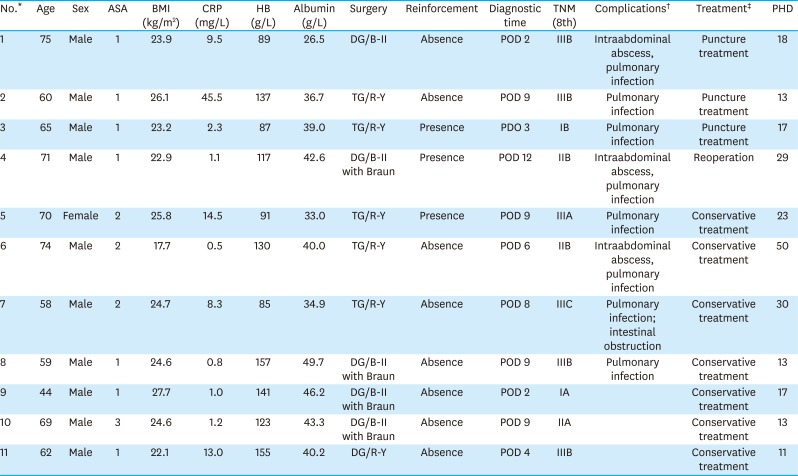
Table 4
Details of patients with DSL
ASA = American Society of Anesthesiologists; BMI = body mass index; CRP = C-reactive protein; HB = hemoglobin; DG = distal gastrectomy; TG = total gastrectomy; R-Y = Roux-en-Y; B-II = Billroth II; POD = postoperative day; PHD = postoperative hospitalization days; DSL = duodenal stump leakage.
*No patients received neoadjuvant chemotherapy; †Complications other than DSL (C-D grade 3–5); ‡All patients recovered after treatment.
![]()
Go to :
DISCUSSION
DSL is a rare complication of gastrectomy that has a high mortality rate. It can lead to intra-abdominal infections and hemorrhage, significantly lengthening the postoperative hospital stay and increasing treatment costs and mortality rates [2223]. In laparotomy, the duodenal stump is usually reinforced. Presently, minimally invasive techniques, especially laparoscopy, have been widely used in the surgical treatment of GC, but no consensus has been reached regarding duodenal stump management. Furthermore, the risk factors of DSL during a laparoscopic radical gastrectomy are controversial.
In this study, patients who received a laparoscopic radical gastrectomy with R-Y or B-II with Braun reconstruction for GC had a duodenal stump. The results showed that the incidence of DSL was 1.36%, consistent with previous studies. Cozzaglio et al. [11] analyzed more than 8,000 cases of GC (7,987 by the laparotomy, 281 by laparoscopy) and found that laparoscopic surgery increased the risk of DSL (OR, 5.6). On the contrary, Paik et al. [24] and Ali et al. [20], among most researchers, reported that laparoscopic gastrectomy was not related to the occurrence of DSL.
A series of clinical factors were analyzed in this study, and the results showed that age, sex, ASA score, carcinoembryonic antigen level, neutrophil-to-lymphocyte ratio, hemoglobin level, and albumin level were not significantly correlated with DSL. Interestingly, preoperative elevated CRP and overweight or obesity status were positively correlated with the incidence of DSL after laparoscopic gastrectomy. Some studies suggested that patients with multiple comorbidities and nutritional impairments might have a higher risk of DSL [2324]. However, Ri's results were the same as ours [15], and the ASA score and nutritional status were not associated with DSL after laparoscopic gastrectomy. The reason may be due to the small number of patients with comorbidities and nutritional impairments included in this study. Obesity makes surgery more difficult and increases operative time. Moreover, patients with a higher BMI may be at higher risk of developing metabolic diseases such as type 2 diabetes or hypertension, which can also lead to a reduced ability to heal after surgery and ultimately increasing the risk of DSL. Although many previous studies reported no link between BMI and DSL [232426], a recent study found that a BMI ≥23 kg/m2 could increase the risk of DSL with an OR of 9.26 [25]. Other complications have also been shown to increase in patients who were obese or had a high BMI [2728].
Most importantly, our study showed that an elevated preoperative CRP level was one of the risk factors of DSL after laparoscopic gastrectomy. After reviewing previous studies, this is the first report of this phenomenon. However, the concrete mechanism for this remains unclear. Many previous studies have shown that the preoperative CRP level was an independent and significant indicator for elevated morbidity and mortality, including pulmonary resection [29], pancreaticoduodenectomy [30], and cardiac surgery [31]. In addition, other studies demonstrated that preoperative CRP could predict long-term survival for diseases such as colorectal cancer [32], GC [3334], and renal cancer [35]. A recent randomized clinical trial showed that the preoperative CRP-albumin ratio was a promising predictor of early recurrence and postoperative adjuvant chemotherapy response [36]. However, the underlying molecular biological mechanism has not yet been elucidated.
The relationship between surgical parameters and DSL is controversial. Orsenigo et al. [24], Ri et al. [25], and Ramos et al. [26] suggested that the D2 lymph node dissection and subtotal gastrectomy were the risk factors for DSL, but our results were similar to those of most studies except for duodenal stump reinforcement, other factors including gastrectomy type, reconstruction method, operative time, intraoperative blood loss, and lymph node dissection had no direct relationship with DSL occurrence. A phase 2 clinical trial involving 100 patients showed that laparoscopic reinforcement suturing prevented DSL [37]. Two previous studies showed that laparoscopic duodenal stump reinforcement reduced the risk of DSL. Nonetheless, R-Y was used in these 2 studies [2425]. Furthermore, duodenal stump reinforcement could not only reduce the incidence of DSL, it could reduce its severity after laparoscopic gastrectomy. Duodenal stump reinforcement increased the duration of surgery but did not increase the risk of intraoperative blood loss or other complications. A linear stapling device with bioabsorbable polyglycolic acid sheets could be used to reinforce the duodenal stump without the need for manual suturing, ultimately reducing the incidence of DSL [38].
No association between tumor characteristics (including location, size, differentiation, and Tumor Node Metastasis stage) and DSL was found in this study. According to Ramos et al. [26], a tumor in the distal stomach was a risk factor for DSL. More importantly, DSL might reduce long-term survival for patients with GC. Gastric outlet obstruction was thought to increase the occurrence of DSL in Paik's study [23]. The underlying mechanism may be that tumors located in the distal stomach are more prone to gastric outlet obstruction, which increases the risk of mucosal edema and impaired systemic nutrition, all of which increase the risk of DSL.
DSL is one of the most serious complications; fortunately, all patients recovered after treatment in this study. Numerous studies including this one showed that although DSL can occur at different periods after surgery, the most common period is about 1 week postoperative. A systematic review of 20 studies including 294 patients with DSL showed that the DSL diagnosis occurred between the fifth and tenth postoperative days [39]. Many patients with DSL developed more than one complication, including but not limited to sepsis, abdominal abscess, wound infection, pneumonia, and intra-abdominal bleeding. In this study, some patients with DSL had other complications, but none were serious. Our experience was that early intervention was needed once these complications occurred.
For example, if the patient has a small amount of abdominal fluid with a low-grade fever or normal body temperature, especially if the drainage tube can successfully drain fluids around the duodenal stump, conservative treatment (antibiotics and enhanced nutritional support) may be appropriate. Additionally, if the patient's abdominal cavity effusion can be resolved using puncture treatment, a conservative treatment approach can be selected. Surgical treatment decisions should be based on a patient’s situation and symptoms. If the patient has recurrent or increased abdominal effusion or continues to suffer from a repeated high fever and fails to respond to antibiotic treatment, guided ultrasound or CT puncture drainage should be used and the drainage fluid should be cultured to develop a specific treatment plan. In the event that conservative or puncture treatment fails and fluid accumulation is increased excessively or if the fluid accumulation in the abdominal cavity is intractable despite measures taken, surgical treatment should be provided as soon as possible. It must be emphasized that patients must be kept under close observation to reduce the possibility of conservative treatment-induced aggravations.
The treatment of DSL includes conservative, percutaneous, endoscopic, and surgical treatments. Nonsurgical treatments are typically the preferred choice. The surgical approach should be reserved for severe cases or those in which nonsurgical approaches fail. Cornejo et al. [40] believed that conservative management had better outcomes than surgery. Paik et al. [23] reported 16 cases of DSL, 3 of which were treated with reoperation; all patients had to undergo reoperation 1–2 days after surgery. Ali et al. [19] reported that all patients with DSL (n = 19) were successfully treated nonsurgically and no patients died. A study included 10 patients with DSL, 4 of whom received unreinforced duodenal stump and underwent reoperation after DSL. In contrast, 6 patients were treated with duodenal stump reinforcement after the diagnosis of DSL; of them, only 1 needed reoperation, while the rest received conservative treatment [25]. Other studies reported the use of endoscopic clipping in the treatment of DSL [41].
This study is of particular importance in China as 1 to 2 intra-abdominal drainage tubes are routinely indurated after gastrectomy, one close to the duodenal stump, if present. DSL can be diagnosed according to the amylase level of the drainage tube fluid. Moreover, once the diagnosis is made, this drainage tube can continue to drain the fluid around the stump, reducing the risk of intra-abdominal infection and facilitating duodenal stump healing. As a result, the proportion of patients receiving conservative treatment in this study was significantly higher. However, Schots et al. [42] believed that abdominal drainage and amylase measurement did not influence the early recognition and management of leakage in GC, but his study included only 3 patients with DSL. Therefore, we recommend that the duodenal stump be reinforced during laparoscopic radical gastrectomy to reduce the risk of DSL, especially for patients with risk factors.
Although we adopted a scientific and rigorous method for analysis, the study still has shortcomings. It was a retrospective study with some inevitable defects, including selection bias and recall bias. In addition, the patients included in this study were from China, a region with a high incidence of GC; thus, this conclusion might not be directly applicable to Western countries. Most importantly, because this was a retrospective study, the indications for duodenal stump reinforcement are unclear and mostly determined by surgeon experience. This study aimed to confirm the significance of duodenal stump reinforcement and clarify its necessity. Finally, the methods of duodenal stump reinforcement varied, and their differences could not be analyzed. Therefore, the conclusions of this study must be further verified by large multicenter clinical trials.
In conclusion, our research shows that DSL after laparoscopic radical gastrectomy for GC is rare. The main risk factors for DSL are obesity, increased preoperative CRP level, and an unreinforced duodenal stump.
Go to :
 XML Download
XML Download