

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Proximal gastrectomy (PG) is a function-preserving surgery that is used to treat an early-stage of proximal gastric cancer. Unlike partial distal gastrectomy, which is usually performed in cases of distal gastric cancer, PG is not commonly performed in cases of proximal gastric cancer despite having been reported as a function-preserving surgery that prevents long-term metabolic adverse effects after total gastrectomy [123]. The main reason for this is the high postoperative occurrence of reflux and anastomotic stricture, and the lack of studies showing the functional and metabolic benefits of PG over total gastrectomy.
Many reconstruction techniques have been proposed to prevent reflux symptoms following a PG [456]; however, an optimal reconstruction technique remains elusive. The main issues are reflux, stricture, surveillance of remnant stomach, technical complexity, cost, operative time, and other morbidities; a major issue is a reflux, which is caused by loss of the food-containing function of the fundus, transition of a newly formed esophagogastric junction (EGJ) above the diaphragm like a sliding hiatal hernia, and loss of the angle of His [78].
We recently devised an anastomosis method to fix the distal part of the posterior esophageal wall and the proximal part of the anterior stomach wall to resolve those 3 physiological mechanisms that create a reflux. We named this method the SPADE operation because of its spade shape as an acronym of spade-shaped esophagogastrostomy (EG) after PG involving partial duplication of the esophagogastric wall [9].
This technique enabled anastomosis creation in the abdominal cavity as well as an artificial angle of His and pseudo-fornix and duplication of 2–3 cm of esophagogastric walls in the anastomosis that could have sphincter function because of distal peristaltic muscles [10].
This study aimed to show the safety and feasibility of the SPADE operation as an alternative to PG by comparing its short-term outcomes with those of conventional esophagogastrostomy (CEG).
Go to : 
MATERIALS AND METHODS
A total of 56 patients who underwent PG from January 2012 to June 2017 were enrolled in the study. All patients were diagnosed with gastric cancer according to the 7th edition of TNM staging by endoscopy (EGD) and computed tomography. We included patients with T1N0 cancer and a tumor size smaller than 4 cm. Esophageal invasion was not a contraindication. However, in cases of esophageal invasion, the procedure is difficult because the abdominal esophagus is short. After PG, 30 patients underwent CEG using a circular end-to-end anastomosis (EEA; CEG group), while 26 patients underwent the SPADE operation (SPADE group). We collected the patients' demographic characteristics and operative and short-term postoperative outcome data from the prospectively collected database of the Center for Gastric Cancer.
Postoperative complications were coded according to the Clavien–Dindo classification. The reflux symptoms were classified into 3 stages as follows: no or mild symptoms, occasional symptoms requiring medication, and severe symptoms that were not fully improved by medication or that interfered with daily life. The presence of postoperative stenosis was identified if any interventions were required to treat the stenosis. All patients were followed up by routine clinical visits every 6 months for 5 years. They were evaluated for symptoms, underwent EGD, and were prescribed proper medication; interventions were decided according to the clinical assessment during visits.
In the follow-up endoscopic examinations, reflux esophagitis was classified according to the Los Angeles (LA) classification [11]. Bile reflux and residual food were evaluated as part of the Red, Green, Blue (RGB) classification [12]. This study was approved by the Institutional Review Board of the National Cancer Center (No. NCC2018-0371).
All analyses were performed using SAS® version 9.1.3 for Windows® (SAS Institute, Cary, NC, USA). Categorical variables were compared using the Pearson χ2 test, while continuous variables were compared using Student's t-test for normally distributed data and the Mann-Whitney U test for non-normally distributed data. All values are expressed as means±standard error of the mean. Statistical significance was set at P<0.05.
Surgical techniques
In all patients, laparoscopy-assisted or laparoscopic D1+PG was performed according to the Japanese gastric cancer treatment guidelines [13]. The hepatic branch of the vagus nerve was preserved in all cases. Pyloromyotomy or pyloroplasty in any form was never performed.
Conventional esophagogastroscopy
The CEG procedure was performed using the laparoscopic-assisted method (open method). The abdominal esophagus was transected, and a 25-mm anvil was introduced and anchored by a purse string. The stomach was divided using a linear stapler. After the negative resection margins were confirmed, the anastomosis was performed using a circular EEA on the anterior wall 3–4 cm below the proximal end of the remnant stomach. No pyloric manipulation for pyloroplasty was performed.
SPADE operation
The abdominal esophagus was transected right above the EGJ, and the stomach was divided at least 2 cm below the distal margin of the tumor using linear staplers (Fig. 1). After a negative resection margin was confirmed on the frozen biopsy, the center of the proximal margin of the remnant stomach and the region 3 cm above the esophagus stump were fixed with an interrupted suture to maintain the anastomosis in the abdominal cavity and attach the 2 intestinal walls 3 cm above the anastomosis. A 3-cm opening was made 3 cm below the proximal margin on the anterior remnant stomach. The stapled line of the esophageal stump was cut with ultrasonic shears to open the esophagus to perform a hand sewing anastomosis with the gastric opening. Finally, hand sewing anastomosis was performed with 2 lines of continuous barbed suture: one for the posterior wall and the other for the anterior wall. Each continuous suture was initiated from the left corner toward the opposite right side. When the anastomosis was completed, a spade shape was formed, and an artificial angle of His and pseudo-fornix was created with a sphincter in the abdominal cavity (Figs. 2 and 3).
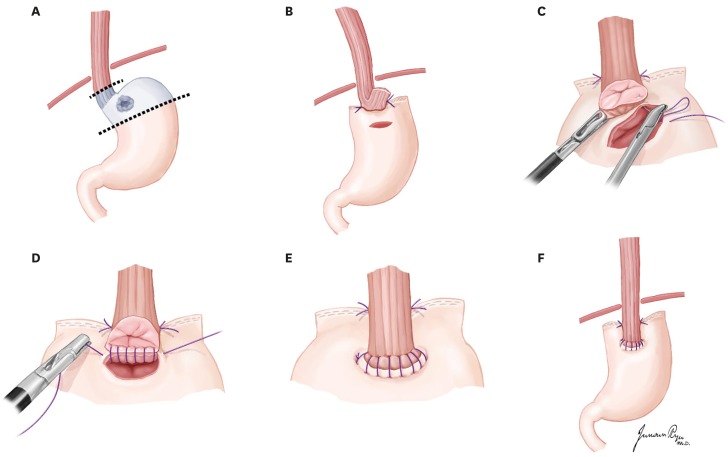 | Fig. 1Illustration of SPADE operation. (A) Laparoscopy assisted or totally laparoscopic D1+ proximal gastrectomy was conducted. (B) Both distal part of posterior wall of esophagus and proximal part of anterior wall of stomach with an interrupted suture. (C) After opening was made, one stitch was made at the left corner of esophagus posterior wall and stomach anterior wall. (D) The anastomosis was performed using 2 continuous suture V-Loc™ or Stratafix™. Each continuous suture was started from the left corner to the opposite direction. (E) After completion of posterior wall anastomosis, anterior wall anastomosis is performed in the middle direction from both ends. (F) After completion of anastomosis, spade shape is formed and, the artificial his angle and pseudo-fornix is made with sphincter and intraabdominal anastomosis.
|
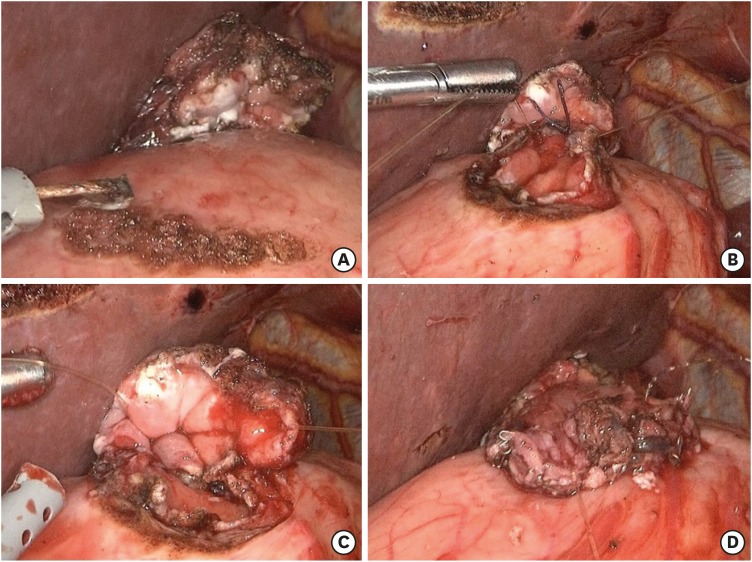 | Fig. 2Laparoscopic view of SPADE operation. (A) Both distal part of posterior wall of esophagus and proximal part of anterior wall of stomach with an interrupted suture. (B) After opening was made, one stitch was made at the left corner of esophagus posterior wall and stomach anterior wall. (C) The anastomosis was performed using 2 continuous suture V-Loc™ or Stratafix™. (D) After completion of anastomosis, spade shape is formed and, the artificial his angle and pseudo-fornix is made with sphincter and intraabdominal anastomosis.
|
Go to :
RESULTS
The demographic and clinicopathological characteristics of the patients who underwent the SPADE operation versus conventional reconstruction using conventional anastomosis are presented in Table 1. There were no significant intergroup differences.
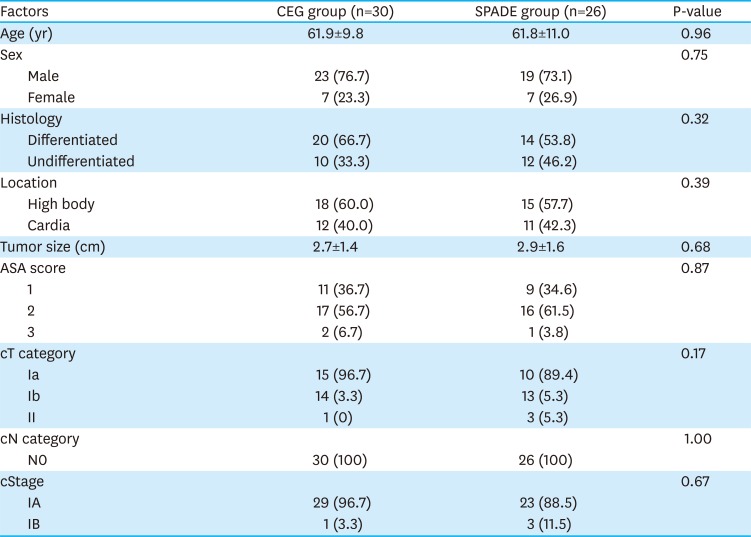
Table 1
Patients' clinicopathological factors
CEG group = conventional esophagogastrostomy anastomosis using a circular end-to-end anastomosis stapler; SPADE group = SPADE operation group; ASA = American Society of Anesthesiologists.
![]()
No significant intergroup differences were seen in postoperative complications (Table 2). In the CEG group, 1 patient had anastomotic leakage and underwent esophageal stent insertion. Four patients had anastomotic stricture and were treated with balloon dilatation. In the SPADE group, 1 patient had anastomotic leakage and was treated with esophageal stent insertion. EG leakage was found postoperatively in both cases for which esophageal stent insertion was performed. Nil per os status and parenteral nutrition support were initiated. After more than a week, follow-up EGD showed no leakage, a regular diet was started, and the stents were removed. An outpatient follow-up exam showed good recovery without symptoms such as stricture.
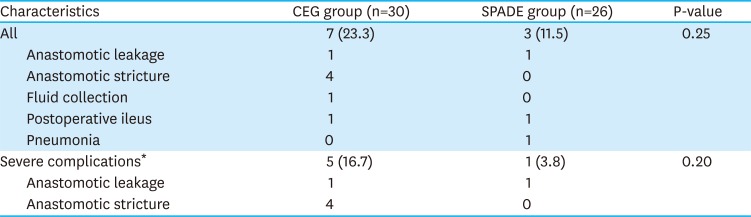
Table 2
Postoperative complications
CEG group = conventional esophagogastrostomy anastomosis using a circular end-to-end anastomosis stapler; SPADE group = SPADE operation group.
*Above Clavien–Dindo classification III.
![]()
Follow-up EGD showed frequent reflux esophagitis cases in the CEG group than in the SPADE group (30% vs. 15.3%, P=0.19). Similarly, the mean bile reflux grade was higher (26.7% vs. 7.7%, P=0.08) in the CEG group than in the SPADE group, as was the residual food grade (P=0.01). In the CEG group, mild reflux symptoms were seen in 13 patients, whereas severe reflux symptoms in 3 patients. In the SPADE group, 3 patients had mild reflux symptoms, while 1 had severe reflux symptoms, i.e., 31.8% lower than the CEG group (P=0.01) (Table 3).
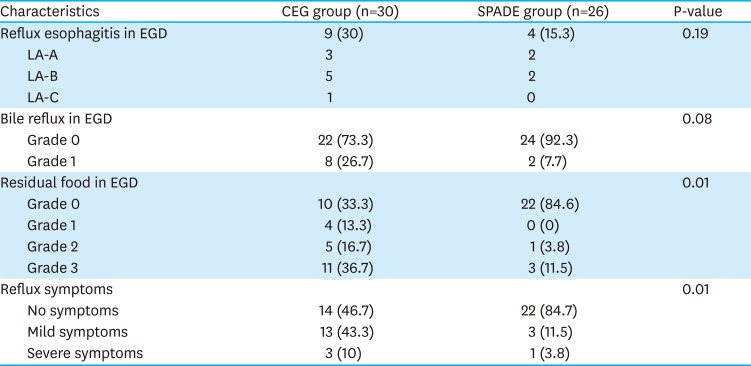
Table 3
Postoperative endoscopic findings and reflux symptoms
CEG group = conventional esophagogastrostomy anastomosis using a circular end-to-end anastomosis stapler; SPADE group = SPADE operation group; EGD = esophagogastroduodenoscopy; LA = The Los Angeles Classification system.
![]()
The mean operating time was longer in the SPADE group. Estimated blood loss and length of stay did not differ between the 2 groups (Table 4).

Table 4
Surgical findings and short-term clinical course
CEG group = conventional esophagogastrostomy anastomosis using a circular end-to-end anastomosis stapler; SPADE group = SPADE operation group.
![]()
Go to :
DISCUSSION
In this study, the SPADE operation resulted in reduced postoperative reflux symptoms and stricture compared to the CEG operation.
The advantages of the SPADE operation are derived from physiological factors including the loss of fundus function, creation of a new sliding EGJ above the diaphragm, and loss of the angle of His, all of which are significant physiological changes contributing to the high prevalence and severity of reflux symptoms after a CEG anastomosis. When the anastomosis is performed in the abdominal cavity, the angle of His is formed and a pseudo-fornix is made. The angle of His, the acute angle usually present between the upper position of the fundus and the EGJ, is an important factor in preventing natural backflow [1011]. Side pressure of the pseudo-fornix could be useful in closing the duplicated portion of the EGJ like a valve. Compared to the stapler method for anastomosis, the hand sewing method is associated with a reduction in anastomosis stricture, although it has the disadvantage of a longer operation time and increased intraoperative blood loss. The SPADE operation used laparoscopic suturing to perform the anastomosis, which is expected to reduce the anastomotic stricture as opposed to the stapler method [14].
In the SPADE group, 4 patients (15.3%) had mild to severe reflux symptoms. These patients had EGJ, and the length of the remaining abdominal esophagus was relatively short, which made the SPADE operation difficult. In contrast to the CEG group, there were no anastomotic stricture cases in the SPADE group because there were fewer postoperative reflux symptoms, and use of the hand sewing suture could reduce the risk of stricture [15]. As with a reflux esophagitis, the presence of an anastomosis site in the abdominal cavity may have a beneficial effect on residual food.
To date, many studies have aimed to reduce the reflux symptoms and anastomotic stricture after PG in several ways; however, an optimal method has not been established yet. Although the double tract method reportedly reduces the reflux symptoms [6], it is complicated because of the need for 3 anastomoses. In addition, it is nutritionally less beneficial because of the food bypassing the stomach considerably, and performing surveillance of remnant gastric cancers is not easy [8]. Because the incidence of remnant gastric cancer after a PG was 5.4% in one report, the potential of a failing endoscopic examination is a serious pitfall of double tract reconstruction [16]. Jejunal interposition is technically demanding and complicated [17]. The hinged double flap method (Kamikawa's method) has the advantage of requiring only one EG and reducing the reflux symptoms; however, it is difficult to perform because it requires a complicated intracorporeal suturing [181920]. Moreover, the mechanism of sphincter function occurs in the muscle layer and not in the serosal covering. It became a tedious surgery because of the complicated and inconsequential serosal flap. In contrast, the SPADE operation has the advantage of having a mean operation time of 247.8±42.6 minutes, which is lower than that of the previously introduced double flap operation time (386.5±78.9 minutes) [20].
The disadvantage of the SPADE operation might be its technical aspects. The posterior wall suture is more difficult because the esophageal mucosa is difficult to identify. This could be overcome through experience.
This study has several limitations because of being an explorative small case series compared to a retrospective historical control group. The difference between laparoscopy-assisted PG and laparoscopic PG may have also influenced the difference in short-term postoperative outcomes. The operator's experience can also affect the operation time and post-operative complications, both of which are limitations of this study. However, because of the clear intergroup differences in surgical procedures, it is assumed that this is a more crucial factor than operation time and post-operative complications. This study reports a short-term postoperative result, i.e., the presence or absence of reflux symptoms and strictures; thus, long-term postoperative results such as nutritional advantages should be identified in future studies. Further objective measures of nutritional or functional studies such as physiological pressure, function, and pH should be examined in the future.
In conclusion, the SPADE operation showed the potential ability to reduce reflux symptoms in PG. To verify and improve its benefits and safety, large-scale prospective clinical studies should be conducted in the future.
Go to :
 XML Download
XML Download