

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Surgical resection of the primary tumor with its lymphatics remains the gold standard for curative treatment of gastric adenocarcinoma. Earlier studies aiming to improve prognosis in gastric cancer patients have investigated the lymphatic flow by using activated carbon particles or India ink injection [1234]. The possible lymphatic spread of the tumor was determined with the lymphangiogram results, incidence of lymph node metastasis, and potential survival benefit of the systematic dissection of the lymphatic flow; moreover, radical surgery for gastric cancer has been standardized based on these data.
Comprehensive investigations have demonstrated that the stomach has a sophisticated lymphatic flow, and gastric tumors follow various spreading patterns according to the tumor location or biology [3456]. The lymphatic flow of upper body tumors, specifically those located along the greater curvature, is drained to splenic hilar lymph nodes via the left gastroepiploic artery, short gastric artery, celiac artery, and posterior gastric artery [47]. Therefore, splenic hilar lymph nodes, which are also classified as number 10 lymph nodes, were defined as one of the regional lymph node groups (N2 group) of gastric cancer (except for lower, lower/middle tumors, which are classified as N3 group) [48]. In a study that analyzed the lymph node metastasis pattern in 1,931 gastric cancer patients, the incidence of splenic hilar lymph node metastasis was 9%, with the 5-year survival rate of 12% [9]. This study also confirmed that the incidence of splenic hilar lymph node metastasis for proximal tumors located at the greater curvature is substantially high (32%), whereas that of the tumors along the lesser curvature or on the anterior/posterior walls is only up to 6%. Okajima and Isozaki [10] reported that the incidence of the splenic hilar lymph node metastasis according to the location of gastric cancer was 26.7%, 15.5%, and 1.9% for tumors located in whole stomach, upper body and mid body, respectively; however, no metastases were found in the splenic hilar lymph nodes with cancer of the lower third part of the stomach. In this context, total gastrectomy with splenectomy for dissecting splenic hilar lymph nodes was accepted as a part of curative gastrectomy for proximal gastric cancer [11].
Go to : 
THE INCIDENCE AND RISK FACTORS FOR SPLENIC HILAR LYMPH NODES METASTASIS
Following the adoption of splenic hilar lymph node dissection as a part of D2 lymph node dissection for proximal gastric cancer, the incidence of splenic hilar lymph node metastasis in gastric cancer has been published repeatedly. This incidence in various series, and metastasis rates according to the cross-sectional tumor location, Borrmann classification, depth of invasion, and pathological stage are summarized in Tables 1, 2, 3 [7121314151617181920212223242526]. In these series, the incidence of splenic hilar lymph node metastasis was reported to be 8.1%–27.9%, and 571 (11.7%) of the 4,900 included patients presented this metastasis. The incidence was higher in majority of the studies for tumors located at a greater curvature or encircling tumors, Borrmann III–IV class, deeper T stage, and advanced pathological stage. Additional clinical factors including younger age, female sex, increased tumor size, poorly differentiated or undifferentiated tumors, advanced N stage, presence of lymphovascular invasion, and presence of distant metastasis were also identified as risk factors for the splenic hilar lymph node metastasis [71415161718202125].
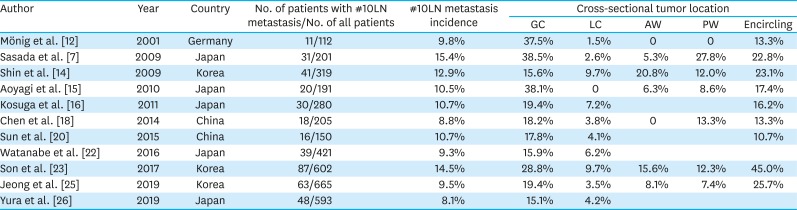
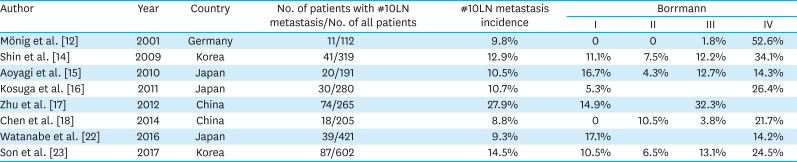
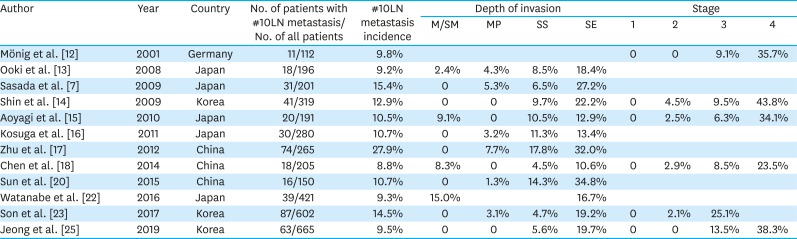
Table 1
The incidence of #10LN according to the cross-sectional tumor location
| Author | Year | Country | No. of patients with #10LN metastasis/No. of all patients | #10LN metastasis incidence | Cross-sectional tumor location | ||||
|---|---|---|---|---|---|---|---|---|---|
| GC | LC | AW | PW | Encircling | |||||
| Mönig et al. [12] | 2001 | Germany | 11/112 | 9.8% | 37.5% | 1.5% | 0 | 0 | 13.3% |
| Sasada et al. [7] | 2009 | Japan | 31/201 | 15.4% | 38.5% | 2.6% | 5.3% | 27.8% | 22.8% |
| Shin et al. [14] | 2009 | Korea | 41/319 | 12.9% | 15.6% | 9.7% | 20.8% | 12.0% | 23.1% |
| Aoyagi et al. [15] | 2010 | Japan | 20/191 | 10.5% | 38.1% | 0 | 6.3% | 8.6% | 17.4% |
| Kosuga et al. [16] | 2011 | Japan | 30/280 | 10.7% | 19.4% | 7.2% | 16.2% | ||
| Chen et al. [18] | 2014 | China | 18/205 | 8.8% | 18.2% | 3.8% | 0 | 13.3% | 13.3% |
| Sun et al. [20] | 2015 | China | 16/150 | 10.7% | 17.8% | 4.1% | 10.7% | ||
| Watanabe et al. [22] | 2016 | Japan | 39/421 | 9.3% | 15.9% | 6.2% | |||
| Son et al. [23] | 2017 | Korea | 87/602 | 14.5% | 28.8% | 9.7% | 15.6% | 12.3% | 45.0% |
| Jeong et al. [25] | 2019 | Korea | 63/665 | 9.5% | 19.4% | 3.5% | 8.1% | 7.4% | 25.7% |
| Yura et al. [26] | 2019 | Japan | 48/593 | 8.1% | 15.1% | 4.2% | |||
#10LN = number 10 lymph nodes; GC = greater curvature; LC = lesser curvature; AW = anterior wall; PW = posterior wall.
![]()
Table 2
The incidence of #10LN according to the Borrmann classification
| Author | Year | Country | No. of patients with #10LN metastasis/No. of all patients | #10LN metastasis incidence | Borrmann | |||
|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | |||||
| Mönig et al. [12] | 2001 | Germany | 11/112 | 9.8% | 0 | 0 | 1.8% | 52.6% |
| Shin et al. [14] | 2009 | Korea | 41/319 | 12.9% | 11.1% | 7.5% | 12.2% | 34.1% |
| Aoyagi et al. [15] | 2010 | Japan | 20/191 | 10.5% | 16.7% | 4.3% | 12.7% | 14.3% |
| Kosuga et al. [16] | 2011 | Japan | 30/280 | 10.7% | 5.3% | 26.4% | ||
| Zhu et al. [17] | 2012 | China | 74/265 | 27.9% | 14.9% | 32.3% | ||
| Chen et al. [18] | 2014 | China | 18/205 | 8.8% | 0 | 10.5% | 3.8% | 21.7% |
| Watanabe et al. [22] | 2016 | Japan | 39/421 | 9.3% | 17.1% | 14.2% | ||
| Son et al. [23] | 2017 | Korea | 87/602 | 14.5% | 10.5% | 6.5% | 13.1% | 24.5% |
![]()
Table 3
The incidence of #10LN according to the depth of invasion and stage
| Author | Year | Country | No. of patients with #10LN metastasis/No. of all patients | #10LN metastasis incidence | Depth of invasion | Stage | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M/SM | MP | SS | SE | 1 | 2 | 3 | 4 | |||||
| Mönig et al. [12] | 2001 | Germany | 11/112 | 9.8% | 0 | 0 | 9.1% | 35.7% | ||||
| Ooki et al. [13] | 2008 | Japan | 18/196 | 9.2% | 2.4% | 4.3% | 8.5% | 18.4% | ||||
| Sasada et al. [7] | 2009 | Japan | 31/201 | 15.4% | 0 | 5.3% | 6.5% | 27.2% | ||||
| Shin et al. [14] | 2009 | Korea | 41/319 | 12.9% | 0 | 0 | 9.7% | 22.2% | 0 | 4.5% | 9.5% | 43.8% |
| Aoyagi et al. [15] | 2010 | Japan | 20/191 | 10.5% | 9.1% | 0 | 10.5% | 12.9% | 0 | 2.5% | 6.3% | 34.1% |
| Kosuga et al. [16] | 2011 | Japan | 30/280 | 10.7% | 0 | 3.2% | 11.3% | 13.4% | ||||
| Zhu et al. [17] | 2012 | China | 74/265 | 27.9% | 0 | 7.7% | 17.8% | 32.0% | ||||
| Chen et al. [18] | 2014 | China | 18/205 | 8.8% | 8.3% | 0 | 4.5% | 10.6% | 0 | 2.9% | 8.5% | 23.5% |
| Sun et al. [20] | 2015 | China | 16/150 | 10.7% | 0 | 1.3% | 14.3% | 34.8% | ||||
| Watanabe et al. [22] | 2016 | Japan | 39/421 | 9.3% | 15.0% | 16.7% | ||||||
| Son et al. [23] | 2017 | Korea | 87/602 | 14.5% | 0 | 3.1% | 4.7% | 19.2% | 0 | 2.1% | 25.1% | |
| Jeong et al. [25] | 2019 | Korea | 63/665 | 9.5% | 0 | 0 | 5.6% | 19.7% | 0 | 0 | 13.5% | 38.3% |
#10LN = number 10 lymph nodes; M = mucosa; SM = submucosa; MP = muscularis propria; SS = subserosa; SE = serosa.
![]()
In a study by Sasada et al. [7], splenic hilar lymph node metastasis was detected in 31 (15.4%) of 201 patients who underwent total gastrectomy and splenectomy for proximal gastric cancer. In multivariate analysis of their study, age was the only predictive factor, whereas the presence of distant metastasis, tumor size, differentiation, and macroscopic type were not. The most important finding of their study was the relationship between the frequency of lymph node metastasis and the splenic hilum, cross-sectional tumor location, and T stage. Splenic hilar lymph node metastasis was more common in patients with tumor located at the greater curvature (38.5%), posterior wall (27.8%), encircling involvement (22.8%), and this incidence increased with elevation in the T stage (27.2% for serosa-positive tumors). No splenic hilar lymph node metastasis was observed for patients with serosa-negative tumors located at the lesser curvature and anterior wall.
Aoyagi et al. reported that cross-sectional tumor location and pathological stage were associated with splenic hilar lymph node metastasis. In contrast, age, T stage, N stage, and the number of lymph node metastasis were not [15]. In their study, the incidence of splenic hilar lymph node metastasis was 38.1% (8 of 21 patients) for the greater curvature tumors and 17.4% (8 of 46 patients) for encircling tumors. No splenic hilar lymph node metastasis was observed in patients with lesser curvature tumors (none of 73 patients). Splenic hilar lymph node metastasis was not observed in stage-I tumor patients (none of 25 patients); however, it was observed in 34.1% (14 of 41 patients) stage-IV patients. The authors also demonstrated the correlation between positivity in #4sa, #4sb, or #11 lymph nodes and the splenic hilar lymph node metastasis.
One of the highest incidences for splenic hilar lymph node metastasis was observed in a study, which enrolled 265 patients subjected to gastrectomy combined with splenectomy (curative or palliative intent), of which 74 (27.9%) patients had splenic hilar lymph node metastasis (23.5% for patients who underwent R0 resection) [17]. Younger age, Borrmann III–IV lesions, Lauren diffuse-type histology, lymphovascular invasion, T stage, N stage, presence of nonregional lymph node metastasis, and peritoneal cytology positivity as significant risk factors correlated with splenic hilar lymph node metastasis. Among these, T stage, N stage, and the presence of distant lymph node metastasis were independent risk factors. While no splenic hilar lymph node metastasis was observed in early gastric cancer, 28.9% (41 of 142 patients) of serosa positive tumors and 39.3% (24 of 61 patients) of tumors with adjacent organ invasions had splenic hilar lymph node metastasis. Moreover, splenic hilar lymph node metastasis was identified in 49.3% (33 of 67 patients) of patients with 7–15 positive lymph nodes, 82.4% (28 of 34 patients) of patients with >15 positive lymph nodes, and 72.8% (16 of 22 patients) with distant lymph node (#13, #14a, and those beyond #15) metastasis.
In another study, the risk factors related to splenic hilar lymph node metastasis in patients with advanced cancer, T stage, differentiation, tumor size, cross-sectional location, and Bormann type were associated with the splenic hilar lymph node metastasis; however, multivariate analysis demonstrated that only T stage and tumor size act as the independent factors [20]. Incidences of splenic hilar lymph node metastasis were 1.3%, 14.3%, and 34.8% for T2, T3, and T4 tumors, respectively. Splenic hilar lymph node metastasis was observed in only 3 of 89 (3.4%) patients with tumors smaller than 5 cm and in 13 of 61 (21.3%) patients with larger tumors. In this study, they highlighted the importance of preoperative risk prediction for developing a rational surgical strategy for advanced gastric cancer.
In 2017, Hong et al. [21] designed a modeling system to predict the risk of splenic hilar lymph node metastasis for advanced upper gastric cancer. Tumor size, cT stage, and cN stage are considered as independent risk factors for patients undergoing curative gastrectomy with spleen-preserving splenic hilar lymph node dissection excluding stump cancer, tumors invading the adjacent organs, and M1 disease. To create a scoring system, patients were divided into three groups (low, intermediate, and high risk) by using the following factors: 2 points for ≥5 cm tumor size, 1 point for serosal involvement, and 1 point for lymph node positivity. The incidences of splenic hilar lymph node metastasis were 2.8%, 13.9%, and 34.9%, for low, intermediate, and high-risk groups, respectively. Moreover, an algorithm based on the scoring system for splenic hilar lymph node management was proposed.
Go to :
SURVIVAL BENEFIT OF NUMBER 10 LYMPH NODE DISSECTION
Several studies have compared the survival outcomes of patients with and without splenic hilar lymph node metastasis. Moreover, the therapeutic value of splenic hilar lymph node dissection was evaluated as a form of the therapeutic index (TI), which was calculated by multiplying the splenic hilar lymph node metastasis incidence by the 5-year overall survival in patients suffering from this disorder [27].
In patients who underwent total gastrectomy plus splenectomy, 5-year survival rates were reported as 5.4%–26% for patients with splenic hilar lymph node metastasis, and majority of the studies have reported poor outcomes in patients with splenic hilar lymph node metastasis compared to the patients without it [714172528]. Subsequent studies have also investigated the efficacy of dissecting splenic hilar lymph nodes in subgroups, not all patients. The 5-year survival rate has been reported up to 51.3% in the subgroups. No survival difference was found in few studies, whereas some studies argued the potential benefits of splenic hilar lymph node dissection in the subgroups.
In Aoyagi's study [15], the presence of splenic hilar lymph node metastasis did not reveal survival difference for stages IIIB and IV patients. In a study by Kosuga et al. [16], no significant difference was observed in 5-year survival between patients with splenic hilar lymph node metastasis and those without it (51.3% and 42.1%, respectively). The overall TI of the projected benefits from splenic hilar lymph node dissection was 5.49 (incidence was 10.7%). In subgroups of greater curvature and Borrmann-IV cancers, therapeutic indices were 19.4 and 12.9, respectively; however, encircling tumors (TI=1.62) and tumors invading the adjacent organs (TI=0) demonstrated quite low therapeutic value from splenic hilar lymph node dissection.
We recently investigated the impact of splenic hilar lymph node metastasis on prognosis in patients with advanced gastric cancer [23]. To this end, we analyzed 602 patients who underwent total gastrectomy with D2 lymph node dissection. We evaluated the subgroups of patients with metastasis to the splenic hilar lymph node, patients with metastasis to extraperigastric stations (#8a, #9, #11, or #12a), and patients with distant metastasis. 5-year overall survival in patients with splenic hilar lymph node metastasis was 24.1% (54.8% for patients without splenic hilar lymph node metastasis) and the TI for splenic hilar lymph node was 3.5; however, no significant differences were observed in the overall survival between patients with splenic hilar lymph node metastasis and those with metastasis to extraperigastric stations. Overall survival in patients with splenic hilar lymph node metastasis was better than that of patients with splenic hilar lymph node plus distant metastasis, and that of patients with distant metastasis but without splenic hilar lymph node metastasis. Moreover, the peritoneum was the most common recurrence site, despite involvement of any extraperigastric lymph nodes. This study revealed that dissection of splenic hilar lymph node provides a similar prognosis to that achieved with the dissection of extraperigastric lymph nodes in patients who underwent total gastrectomy for advanced gastric cancer.
Three studies from Japan investigated the value of splenic hilar lymph node dissection in proximal gastric cancer by dividing the patients into two groups as a greater curvature group (with tumors involving the greater curvature) and a nongreater curvature group (without tumors involving the greater curvature) [222426]. In the first study by Watanabe et al. [22], the incidence of splenic hilar lymph node metastasis in the greater curvature group was 15.9% (6.2% for nongreater curvature group, P=0.032). In the greater curvature group, 5-year overall survival rates with and without splenic hilar lymph node metastasis were 35.4% and 43.1%, respectively (P=0.135), and these rates in the nongreater curvature group were 32.8% and 66.5%, respectively (P<0.001). The TI of splenic hilar lymph node was 5.6 in the greater curvature group and 2.0 in the nongreater curvature group. The greater curvature group was further analyzed in the study, and patients aged <65 years (TI=8.2), with Borrmann-IV (TI=7.1), and with <T4 stage (TI=10.0) demonstrated relatively higher therapeutic indices.
Maezawa et al. [24] investigated the efficacy of splenic hilar lymph node dissection by comparing it to that of the other regional nodes in locally advanced proximal gastric cancer invading the greater curvature. The incidence of splenic hilar lymph node metastasis, 5-year overall survival, and TI were 13.4%, 30%, and 4.02%, respectively. The most important finding of the study was the substantially higher TI of splenic hilar lymph node than those of #8a, #11p, and #11d. The authors suggest that the presence of splenic hilar lymph node is higher than that of the #11 lymph nodes, and they recommended the removal of the splenic hilar lymph nodes as a part of D2 dissection for proximal gastric cancer detected in the greater curvature.
A recent study evaluated the efficacy of splenic hilar lymph node dissection for advanced gastric cancer invading the greater curvature [2629]. No statistically significant difference was observed in 5-year survival for the patients with and without splenic hilar lymph node metastasis in the greater curvature group, whereas significant difference was observed in the nongreater curvature group. The TI of the splenic hilar lymph node station was 7.1 in the greater curvature group, and higher than those of the essential components of D2 dissection, including #5, #6, #8a, #9, #11p, #11d, and #12.
In addition to the observational studies, randomized comparative studies evaluating the impact of splenic hilar lymph node dissection were also published. The first randomized study in English literature was the Chilean study published in 2002 [30]. Herein, the authors compared total gastrectomy versus total gastrectomy with pancreas-preserving splenectomy in patients with gastric cancer. Patients with macroscopic metastasis at the splenic hilum and macroscopic findings of spleen invasion have not been included. Splenic hilar lymph node metastasis was detected in 8 (9%) of 90 patients in total gastrectomy plus splenectomy group. The 5-year survival rates were not statistically different between groups (36% in total gastrectomy group and 42% in total gastrectomy plus splenectomy group). The authors concluded that splenectomy does not influence the survival after total gastrectomy in early stages and may be performed only in selected patients with an advanced-stage disease.
The most systematic randomized study to evaluate splenectomy in total gastrectomy for proximal gastric cancer was published by the Stomach Cancer Study Group of the Japan Clinical Oncology Group in 2017 (JCOG0110) [31]. In this noninferiority trial, 505 patients from 36 institutions were randomized to splenectomy or spleen preservation groups. The 5-year overall survival rates were 75.1% and 76.4% for the splenectomy and the spleen preservation group, respectively. Statistically significant noninferiority of spleen preservation was presented, and the authors concluded that splenectomy should be avoided; however, certain crucial points were highlighted in the study design. Patients with the tumor invading the greater curvature, those with gastric remnant cancer, those with Borrmann-IV, and patients with gross lymph node metastasis at splenic hilum were excluded from the study, that is, patients at high risk for splenic hilar lymph node metastasis were eliminated. Moreover, only advanced cancer was supposed to be included; 14.1% of the included patients had pathological T1 tumors. Therefore, the incidence of splenic hilar lymph node metastasis was quite low (2.4%) in the splenectomy group, compared to the previous studies [3233]. In 58 of 254 patients in the spleen preservation group, splenic hilar lymph node dissection or sampling was performed without splenectomy. Considering the strict eligibility study criteria, the results should not be extrapolated to all gastric cancer patients, and certain questions still need to be answered.
Go to :
FEASIBILITY OF SPLENIC HILAR LYMPH NODE DISSECTION WITHOUT SPLENECTOMY
Removal of the spleen, which is a part of the immune system, has been questioned due to its possible effects on short- and long-term outcomes. Although several surgeons have routinely performed splenectomy for the removal of splenic hilar lymph nodes, it is possible to remove the same group of lymph nodes by preserving the spleen and splenic vessels. A randomized study comparing spleen-preserving splenic hilar lymph node dissection and splenectomy for proximal gastric cancer demonstrated that a similar number of lymph nodes could be removed with both approaches, and that no survival advantage of splenectomy exists over spleen-preserving dissection [34]. In subsequent studies, spleen-preserving dissection was commonly performed with open or laparoscopic approach [35363738]. Interim report of a randomized trial comparing the laparoscopic and open spleen preserving splenic hilar lymph node dissection demonstrated that operative time, number of harvested lymph nodes including splenic hilar lymph node, time taken for splenic hilar lymph node dissection, as well as the complication rates are comparable between the groups [39]. In addition to the successful applications of laparoscopic splenic hilar lymph node dissection, robotic surgery is known to be a feasible and safe approach for spleen-preserving splenic hilar lymph node dissection [4041]. Image-guided surgery with the assistance of 3D simulation and fluorescent lymphography–guided lymph node dissection are also tools that assist surgeons regarding the appropriate anatomy of the splenic vessels before surgery and in identifying all necessary lymph nodes [42434445].
Go to :
SUMMARY
Several factors determine the direction and timing of the lymphatic spread of gastric cancer. The splenic hilar lymph node group is one of the essential targets in the surgical treatment of proximal gastric cancer, and published studies have reported various incidences of splenic hilar metastasis and survival rates for patients with splenic hilar lymph node metastasis. The overall incidence of splenic hilar lymph node metastasis was reported up to 27.9% in gastric cancer, and a correlation was observed between the risk of splenic hilar lymph node metastasis and several clinicopathological factors including age, cross-sectional tumor location, tumor size, T stage, N stage, and pathological stage. All these factors except for the tumor location are parts of advanced or systemic disease and they mostly reflect poor prognosis for gastric cancer patients. Thus, studies exploring long-term outcomes of splenic hilar lymph node dissection failed to present a survival benefit. It is rational to use a cross-sectional tumor location as the best candidate variable in selecting patients who would benefit from the splenic hilar lymph node dissection. The recent randomized trial, which has a strict eligibility criteria, concluded that routine splenic hilar lymph node dissection is not required in all patients requiring total gastrectomy; however, no convincing evidence is available to ignore the benefit of splenic hilar lymph node dissection in patients with a high risk of splenic hilum lymph node metastasis.
Go to :
CONCLUSIONS
The potential benefit of splenic hilar lymph node dissection becomes more pronounced when demonstrated by the relatively higher TI, specifically in tumors involving greater curvature of the proximal stomach and conceivably for Borrmann type IV tumors. Therefore, the dissection of splenic hilar lymph node should be considered and allowed to be a part of curative surgery in selected patient groups, if R0 resection is intended.
Go to :
 XML Download
XML Download