

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breast metastases of extramammary malignant neoplasms are uncommon, accounting for only 0.3%–2.7% of all malignant mammary tumors. Most cases occur in women, with only 5%–8% of cases in men. Breast metastases of extramammary malignant neoplasms are reported more frequently in hematologic malignancies and cutaneous melanoma but other possible primary tumor sites are the lungs, ovaries, cervix, prostate, kidneys, gastrointestinal tract including the liver, and head and neck (Table 1) [12345678]. Metastases of gastric carcinoma (GC) to the breasts are very rare in Caucasian patients, accounting for <0.1% of all breast carcinomas; the prognosis is generally poor because breast involvement is usually observed as disseminated disease. Signet ring cell histotype, antral location of the tumor, and lymph node involvement are very frequent in GC with breast metastasis [9]. As symptoms of primary mammary carcinoma and breast metastasis are generally similar, differentiating between these 2 conditions is pivotal to determine the appropriate treatment.
Table 1
Metastasis to the breast from extramammary solid neoplasms (n=826)

| Tumor site | Percentages |
|---|---|
| Skin (mainly melanomas) | 24% |
| Lungs | 21% |
| Gynecological organs | 15% |
| Genitourinary tract | 10% |
| Gastrointestinal system | 9% |
| Head and neck | 4% |
| Others | 17% |
Herein, we report the first case of metastasis to the breasts caused by an Epstein-Barr virus-associated gastric carcinoma (EBVaGC) during pregnancy in a Caucasian woman.
CASE REPORT
A 39-year-old woman in the 34th week of pregnancy presented to our clinic because of the appearance of a perisplenic mass, suspected to be malignant, on ultrasound examination.
Three years prior to presentation, the patient had undergone a total gastrectomy with D2 lymphadenectomy for GC of the small curve, stage pT4aN3bM0, R0, according to the American Joint Commission on Cancer (AJCC) Staging System [10]. On the gastrectomy specimen, GC was characterized by the presence of aggregates of malignant cells, arranged in irregular sheets, which were associated with prominent tumor-infiltrating lymphocytes and dense peritumoral lymphoid response. The tumor cell nuclei exhibited vesicular chromatin with prominent nucleoli (Fig. 1). In situ hybridization (ISH) for Epstein-Barr virus (EBV)-encoded RNA (EBER) showed strong positivity in most of the tumor cells (Fig. 2). Therefore, a diagnosis of GC with lymphoid stroma was made according to the 2010 World Health Organization Classification of Tumours of the Digestive System [11].
Fig. 1
Histology of gastric carcinoma. The histologic examination revealed lymphoid stroma, prominent lymphocytic infiltration, and syncytial growth (hematoxylin and eosin staining; magnification ×100).
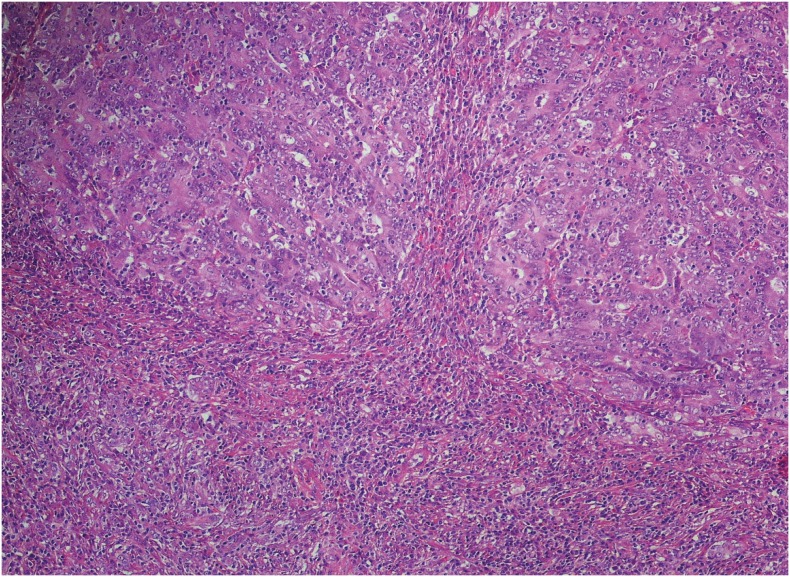
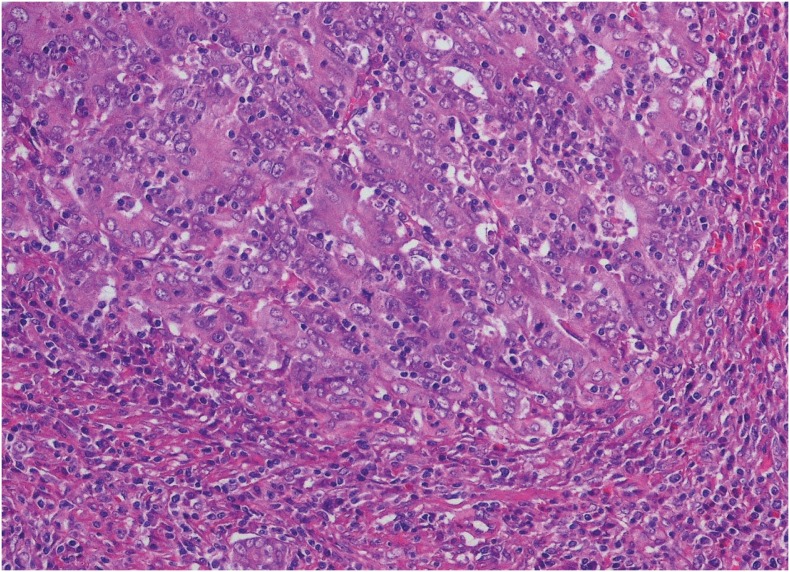
Fig. 2
Histology of gastric carcinoma at higher magnification. At higher magnification (×200), large tumor cell nuclei with open chromatin and prominent nucleoli (hematoxylin and eosin staining) can be observed.
After surgery, the patient underwent six cycles of adjuvant chemotherapy with oxaliplatin and capecitabine; subsequently, she underwent routine follow-up.
After the discovery of the splenic mass, the patient underwent a caesarean operation, as the core biopsy of the splenic nodule revealed metastasis from the previous GC. Immunohistochemistry (IHC) revealed a score of 2+ for c-erbB2 according to the guidelines from the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology [12]; however, the fluorescence in situ hybridization (FISH) test showed negative results for gene amplification.
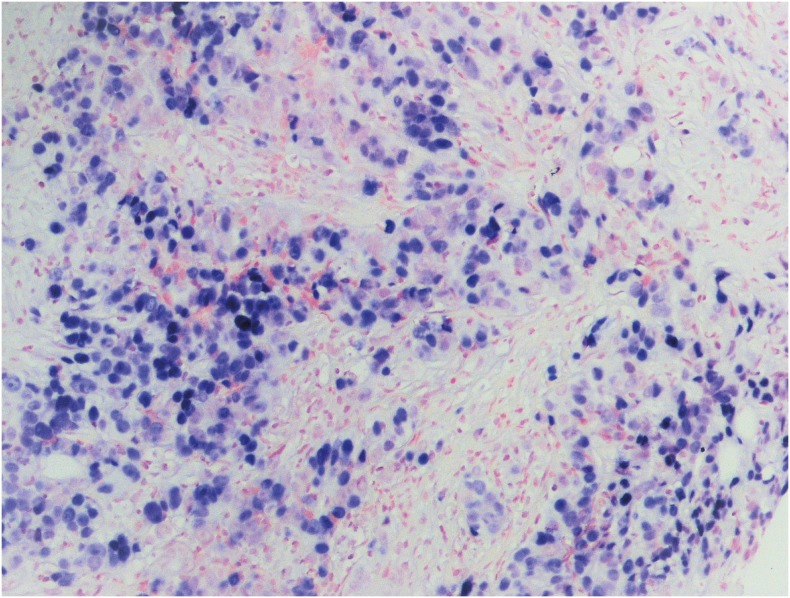
Ten days after delivery, the patient started complaining of pain with tenderness and inflammation in both the breasts. Her gynecologist prescribed cabergoline, and the patient never nursed. On physical examination, her breasts were hardened and showed the presence of orange peel skin, and multiple pathologic axillary and supraclavicular nodes were palpable. A breast ultrasound examination revealed bilateral diffused alteration of the breast parenchyma, with no solitary lesions; we also observed low blood flow on color Doppler imaging owing to the presence of intralesional necrosis. Mammography revealed multiple round irregular lesions without microcalcifications, suspected to be malignant, which were classified as Breast Imaging Reporting and Data System category 5. A biopsy of the breast mass revealed infiltration of poorly differentiated carcinoma associated with discrete lymphoid stroma (Fig. 3). The neoplastic cells were positive for cytokeratin (CK) 8/18 and E-cadherin, and negative for CK7, CK20, CK 5/6, caudal type homeobox 2 (CDX2), androgen receptor (AR), mammaglobin (MMG), gross cystic disease fluid protein-15 (GCDFP-15), and estrogen receptor (ER) and progesterone receptor (PgR). EBER-ISH demonstrated the presence of EBV RNAs in most tumor elements (Fig. 4
). The Mib1/Ki67 proliferative index was 60%, while the IHC staining score was 2+ for c-erbB2; however, FISH again did not reveal any gene amplification. Moreover, programmed death-ligand 1 (PD-L1) expression on IHC was negative. Accordingly, a diagnosis of breast metastasis from GC seemed more reasonable than a primary breast carcinoma owing to the following reasons: 1) the patient's previous history of gastric cancer, 2) the histologic similarity between the breast nodule and the gastric cancer, 3) the EBER positivity of both lesions, and 4) the bi-laterality of breast involvement.
Fig. 3
Histology of breast metastasis. Histology of gastric carcinoma metastatic to the breast: a non-neoplastic breast duct can be observed on the left (hematoxylin and eosin staining; magnification ×200).
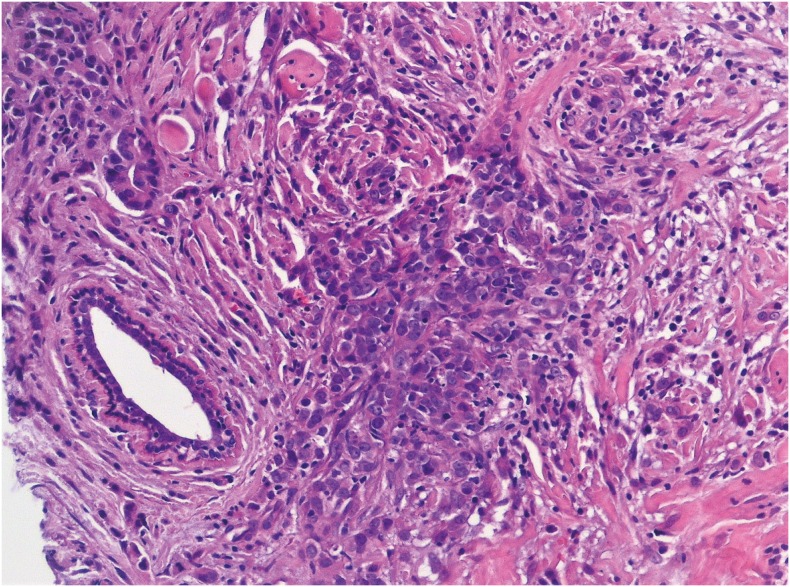
Fig. 4
EBER-ISH. Tumor cells show strong ISH for EBER reactivity (magnification ×200).
EBER = Epstein-Barr virus-encoded RNA; ISH = in situ hybridization; EBV = Epstein-Barr virus.
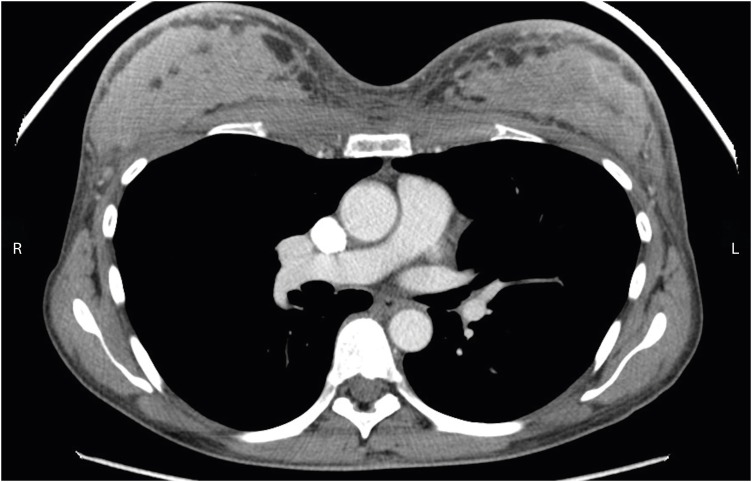
Whole-body computed tomography (CT) revealed the presence of a pelvic parenchymatous lesion, as well as multiple metastases in the spleen and lymph nodes in the mediastinum and in the supraclavicular, axillary, and para-aortic/lumbar regions. CT also showed diffused and highly vascularized alterations in both breasts (Fig. 5).
Fig. 5
CT scan of the breasts. CT scan shows inhomogeneous malignant lesions occupying the parenchyma in both the breasts.
CT = computed tomography; R = right; L = left.
Standard first-line chemotherapy for advanced GC with platinum and 5-fluorouracil was administered, and after 4 cycles, a good clinical and instrumental response was obtained. However, after 8 cycles, CT revealed the appearance of a 5-cm nodule in the inferior part of the sternum. Therefore, the patient started receiving second-line chemotherapy with paclitaxel plus ramucirumab as well as sternal palliative radiotherapy. After three cycles, CT revealed disease progression in the brain and both the breasts. Considering the patient's good performance status and young age, third-line chemotherapy with irinotecan and 5-fluorouracil was initiated. However, the patient's performance status rapidly deteriorated and she died 10.5 months after the diagnosis of metastatic disease.
DISCUSSION
To the best of our knowledge, this is the first reported case of breast metastasis from EBVaGC with lymphoid stroma that developed during pregnancy in a young Caucasian woman.
GC with lymphoid stroma, also referred to as lymphoepithelioma-like carcinoma and medullary carcinoma, is a rare variant, accounting for 1%–7% of all gastric tumors [13]. Considering the histopathologic findings, GC with lymphoid stroma is characterized by irregular sheets, poorly formed tubules, and trabecular or syncytial growth of polygonal cells along with prominent lymphocytic infiltration [12]. This subtype of GC is frequently associated with EBV, with reported rates varying from 22% to 100% [13]. Approximately 90% of the world population is infected by EBV, which has been reported to be associated with several tumor types such as lymphomas and nasopharyngeal, parotid, gastric, and ileal carcinomas [131415]. The reasons why neoplastic transformation occurs only in a small number of patients, while most subjects are spared, are unknown, as are the mechanisms of infection of the gastric epithelium. EBVaGC is more prevalent than EBV-negative GC in younger patients, and it is frequently localized in the proximal stomach or gastric stump and more common in men, suggesting that lifestyle or occupational factors may influence the risk. Moreover, most cases of EBVaGC harbor PIK3CA and ARID1A mutations, genome-wide hypermethylation, and amplification of the CD274 (PD-L1) gene, an important immune checkpoint regulator [1617]. GC with EBV positivity has better prognosis than GC cases that are negative for EBV [14]. Therefore, histological identification of GC with lymphoid stroma and the detection of EBV via EBER testing are biomarkers of good prognosis.
A substantial subset (approximately 40%) of cases of EBV-positive gastric cancer expresses PD-L1 [1718]. Although PD-L1 expression is not an independent prognostic factor, it has been associated with a worse prognosis in EBV-positive gastric cancer [17]. However, in the current case, no PD-L1 positivity was observed despite the aggressive clinical course, which was likely owing to the advanced disease stage at diagnosis.
Metastases to the breasts from extramammary neoplasms are rare, and no case of primary GC with lymphoid stroma and breast involvement has been described till date. However, Lee et al. reported that gastric cancer is the most common tumor to metastasize to the breast, consistent with the high prevalence of this tumor in Korea [2]. In a recent study by Ma et al. [9] on the clinicopathological features and prognosis of 54 patients with breast metastasis from gastric cancer (3 new cases and 51 from previous studies), the median survival time was 8.6 months and the median age at diagnosis of breast metastasis was 43 years. The most frequent characteristics were signet ring cell histology, lymph node involvement, and antral primary lesions.
In pregnant women, breast metastases from solid cancer are not well described. Some hypotheses have been proposed regarding this rare event, suggesting that breast metastases from solid cancer could have been caused by the intrinsic characteristics of the breast tissue or by the hormonal status and subsequent high breast vascularity [19]. In the current case, the pregnancy could have influenced the bilateral and diffuse involvement of both the breasts. Interestingly, another case of a secondary breast tumor from gastric adenocarcinoma has been reported in a French woman in her 32nd week of pregnancy, although she did not have any past history of cancer [20]. However, pregnancy itself does not seem to be a poor prognostic factor for gastric cancer, and according to a recent case-control study, cases of pregnancy-associated GC are not different from cases of GC used as controls considering the expression or amplification of growth factor receptors (ER, PgR, epidermal growth factor receptor, c-erbB2, and fibroblast growth factor receptor 2) [21]. Nevertheless, in our institution, if patients have a past history of advanced neoplastic disease, clinicians inform them of the risk of recurrence and do not recommend pregnancy, in particular within the first year of the diagnosis. Despite this, if pregnancy occurs, a closer and personalized clinical and instrumental follow-up is warranted. A multidisciplinary team, including gynecologists, oncologists, and radiologists, should carefully collaborate during pregnancy. Ultrasound examination is the preferred imaging modality for the breast, abdomen, and pelvis; careful monitoring and iron and vitamin supplementation are also recommended [2223].
As the symptoms due to breast metastasis are non-specific and similar to those due to a primary mammary carcinoma, instrumental and pathological examinations are necessary for making a proper diagnosis. On histological examination, most cases of GC are positive for CDX2 while being negative for MMG, GCDFP-15, ER, and PgR, in contrast to cases of primary breast cancer [24]. The current case was negative for CDX2 on IHC, and this finding may be associated with this peculiar histotype, because EBV-positive GC with lymphoid stroma is often characterized by the low expression of intestinal phenotype markers, including CDX2 [25]. A differential diagnosis could include breast lymphoepithelioma-like carcinoma or carcinoma with medullary features, i.e., a rare entity with a triple-negative, basal-like profile and the following features: a pushing border, a syncytial growth pattern, cells with high-grade nuclei, and prominent lymphoid infiltration [2627]. In the past years, the possible role of EBV in primary breast cancer has shown varying results, according to the geographic area and viral detection methods. The association between EBV and breast cancer appears to be quite inconsistent, mostly if the ISH technique is employed to detect EBV [28]. In the current case, the demonstration of EBER-positive tumor cells, along with the negativity for breast lineage markers, allowed us to make the final diagnosis of breast metastasis from the previous GC.
 XML Download
XML Download