

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite the rapid advances in chemotherapy and molecular targeted therapy and development of immune checkpoint inhibitors, surgical resection with lymphadenectomy is the only curative treatment for gastric cancer. Approximately 10% of patients with advanced proximal gastric cancer develop splenic hilar lymph node (No. 10 lymph node) metastasis [12345678910111213]. In Japan, No. 10 lymph node dissection with splenectomy has routinely been performed in these patients. In complete No. 10 lymph node dissection, splenectomy is considered to be essential. If the tumor directly invades the spleen or there is an obvious No. 10 lymph node metastasis, splenectomy should be performed for curative resection. However, there is no clear consensus as to whether splenectomy should be performed in all patients undergoing prophylactic lymph node dissection. Since splenectomy is known to have some disadvantages [1415], there is a need to demonstrate the survival benefit accruing from splenectomy in these patients. However, studies that have shown the efficacy of splenectomy in this respect are limited. One pivotal randomized controlled trial (RCT) from Japan [16] changed the gastric cancer treatment. Currently, prophylactic splenectomy is performed only in patients with advanced proximal gastric cancer with greater curvature invasion or in those with type 4 gastric cancer. There is still no clear evidence on the need for splenectomy in these patients. Recent studies have described spleen-preserving No. 10 lymph node dissection as a means to surmount the disadvantages of splenectomy while leveraging the benefits of No. 10 lymph node dissection [171819]. The role of No. 10 lymph node dissection may be separately discussed from that of splenectomy. This procedure should be selected instead of splenectomy for prophylactic No. 10 lymph node dissection if backed by evidence.
In this review, we argue that prophylactic No. 10 lymph node dissection with splenectomy should not be performed in all cases. We investigate the evidence pertaining to the efficacy of splenectomy and discuss the disadvantages of No. 10 lymph node dissection with splenectomy. Moreover, we discuss the category of patients who may benefit from No. 10 lymph node dissection and consider spleen-preserving No. 10 lymph node dissection without splenectomy.
Go to : 
ANATOMY AND DISSECTION OF THE SPLENIC HILAR LYMPH NODE
According to the Japanese Classification of Gastric Carcinoma, the splenic hilar lymph node is defined as follows: “Splenic hilar lymph nodes including those adjacent to the splenic artery distal to the pancreatic tail, and those on the roots of the short gastric arteries and those along the left gastroepiploic artery proximal to its first gastric branch” [20]. Splenic hilar lymph node metastasis is common (approximate incidence, 10%) [12345678910111213]. Moreover, prophylactic No. 10 lymph node dissection is considered to be effective in advanced gastric cancer. From the anatomical perspective, there is a complex network of peripheral branches of the splenic artery and vein in the splenic hilum. Moreover, there is considerable interindividual variability with respect to the vascular anatomy in the splenic hilum. For this reason, it is quite difficult to dissect all lymph nodes located around the splenic artery and vein, especially the posterior lymph nodes, without performing splenectomy. Therefore, splenectomy is considered as the standard technique for complete splenic hilar lymph node dissection.
Go to :
EFFICACY OF SPLENECTOMY
We identified 4 prospective RCTs and 12 retrospective studies that compared splenectomy and spleen-preserving procedure without intentional No. 10 lymph node dissection for gastric cancer to assess the efficacy of splenic hilar dissection and splenectomy (Table 1). In the RCT (n=79) conducted by Toge et al. [21], splenectomy was shown to be associated with improved overall survival (OS). However, the sample size in this study was relatively small. The 3-year OS in the splenectomy group (n=41) and spleen-preserving surgery group (n=38) was 71.7% and 56.0% respectively, and this difference was statistically significant. However, there was no significant between-group difference in the 5-year OS. In the RCT by Csendes et al. [22], there were 90 patients in the splenectomy group and 97 patients in the spleen-preserving surgery group. Clinicopathological characteristics were comparable between the 2 groups. The 5-year OS was not significantly different between the 2 groups (42% and 36%, respectively). They also performed a subgroup analysis of 5-year OS disaggregated by disease stage. Although there were no significant between-group differences across all stages, patients with advanced-stage disease showed slightly better survival after splenectomy. These studies included gastric cancer in all circumferential locations, and the differences in tumor location were not considered. This may have influenced the results. In the study by Galizia et al. [23], splenectomy did not improve the disease-free survival (DFS). This study differed from other studies in that it included only lymph node positive patients (any regional lymph nodes) after randomization. The clinicopathologic characteristics were comparable between the splenectomy group (n=37) and spleen-preserving surgery group (n=36), except for the number of retrieved lymph nodes. The 5-year DFS was comparable in the splenectomy and spleen-preserving surgery groups (42.1% and 42.9%, respectively). However, this was not an RCT in the true sense, owing to the small sample size and inclusion of only lymph node positive patients. Lastly, Sano et al. [16] conducted a phase III RCT that showed non-inferiority of spleen-preserving surgery. They included patients with advanced proximal gastric cancer without invasion of the greater curvature line. The 5-year OS in the splenectomy (n=254) and spleen-preserving surgery groups (n=251) was 75.1% and 76%, respectively. The study demonstrated statistically significant non-inferiority of spleen-preserving surgery. The findings suggested that splenectomy need not be performed in patients who meet the inclusion criteria. In this study, splenic hilar metastatic rate was 2.4% in the splenectomy group. This is a relatively low rate compared to those in other studies and probably attributable to the lack of inclusion of patients with greater curvature invasion. This implies that splenic hilar lymph node metastasis is more common in cancer with greater curvature invasion, which seems plausible. This was a well-designed pivotal study with a relatively large sample size. After this trial, the Japanese Gastric Cancer Treatment Guidelines were modified with respect to the indications for splenectomy. The revised guidelines no longer recommended splenectomy if the tumor has not invaded the greater curvature. Among these RCTs, splenectomy showed only marginally positive results in 1 trial with a small sample size. All other trials failed to demonstrate the superiority of splenectomy over spleen-preserving surgery. This inconsistency may be attributable to the inclusion criteria. Inclusion of patients with gastric cancer with greater curvature invasion may affect the results.
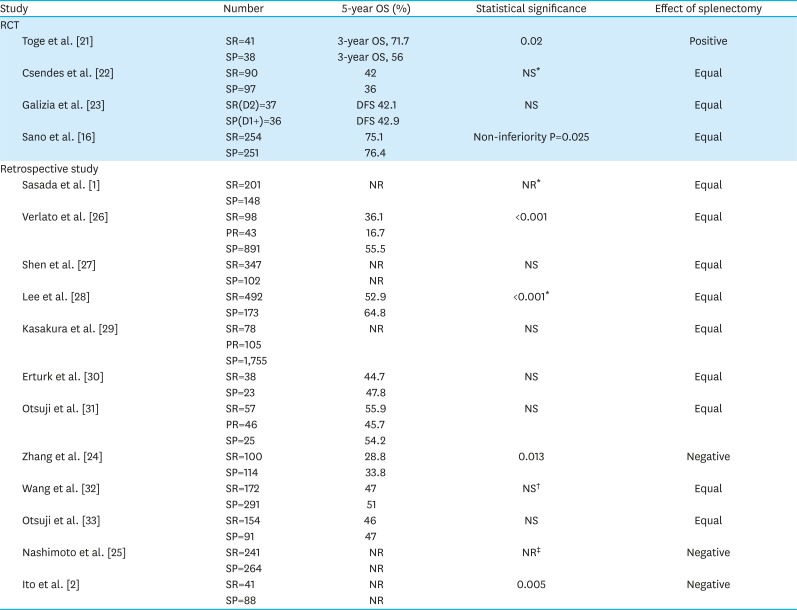
Table 1
Studies comparing splenectomy and spleen-preserving surgery without intentional No. 10 lymph node dissection
| Study | Number | 5-year OS (%) | Statistical significance | Effect of splenectomy | |
|---|---|---|---|---|---|
| RCT | |||||
| Toge et al. [21] | SR=41 | 3-year OS, 71.7 | 0.02 | Positive | |
| SP=38 | 3-year OS, 56 | ||||
| Csendes et al. [22] | SR=90 | 42 | NS* | Equal | |
| SP=97 | 36 | ||||
| Galizia et al. [23] | SR(D2)=37 | DFS 42.1 | NS | Equal | |
| SP(D1+)=36 | DFS 42.9 | ||||
| Sano et al. [16] | SR=254 | 75.1 | Non-inferiority P=0.025 | Equal | |
| SP=251 | 76.4 | ||||
| Retrospective study | |||||
| Sasada et al. [1] | SR=201 | NR | NR* | Equal | |
| SP=148 | |||||
| Verlato et al. [26] | SR=98 | 36.1 | <0.001 | Equal | |
| PR=43 | 16.7 | ||||
| SP=891 | 55.5 | ||||
| Shen et al. [27] | SR=347 | NR | NS | Equal | |
| SP=102 | NR | ||||
| Lee et al. [28] | SR=492 | 52.9 | <0.001* | Equal | |
| SP=173 | 64.8 | ||||
| Kasakura et al. [29] | SR=78 | NR | NS | Equal | |
| PR=105 | |||||
| SP=1,755 | |||||
| Erturk et al. [30] | SR=38 | 44.7 | NS | Equal | |
| SP=23 | 47.8 | ||||
| Otsuji et al. [31] | SR=57 | 55.9 | NS | Equal | |
| PR=46 | 45.7 | ||||
| SP=25 | 54.2 | ||||
| Zhang et al. [24] | SR=100 | 28.8 | 0.013 | Negative | |
| SP=114 | 33.8 | ||||
| Wang et al. [32] | SR=172 | 47 | NS† | Equal | |
| SP=291 | 51 | ||||
| Otsuji et al. [33] | SR=154 | 46 | NS | Equal | |
| SP=91 | 47 | ||||
| Nashimoto et al. [25] | SR=241 | NR | NR‡ | Negative | |
| SP=264 | NR | ||||
| Ito et al. [2] | SR=41 | NR | 0.005 | Negative | |
| SP=88 | NR | ||||
RCT, randomized controlled trial; SR, spleen resection; SP, spleen preservation; PR, pancreatic resection; OS, overall survival; DFS, disease-free survival; NR, not reported; NS, not significant.
*NS after stratification by stage; †NS after stratification by T and N stages; ‡Significantly negative in patients with pSE, pN2, and pStage IIIB.
![]()
None of the retrospective studies have demonstrated any survival benefit conferred by splenectomy. Since patients are not randomly assigned in retrospective studies, the clinicopathologic characteristics were not comparable between the splenectomy and spleen-preserving surgery groups in most studies. The splenectomy group typically included patients with more advanced gastric cancer (e.g., tumor depth, lymph node metastasis, tumor size, undifferentiated type) with relatively poor prognosis. This difference should be considered when interpreting the results. Some studies accounted for differences in background characteristics by comparing patients in the same stage. Three such studies found a negative effect of splenectomy on survival [22425]. The other 9 studies [12627282930313233] concluded that splenectomy has neither positive nor negative impact on survival. The slightly negative results of splenectomy may be attributable to the difference in background characteristics. In most of the cases, splenectomy was performed in patients with more advanced gastric cancer.
The results of RCTs and retrospective studies seem to suggest that splenectomy does not have any impact on survival in patients without greater curvature invasion. Splenectomy may potentially be more effective in cancer with greater curvature invasion. However, there is no robust evidence to support this hypothesis.
Go to :
DISADVANTAGES RELATED TO SPLENIC HILAR LYMPH NODE DISSECTION WITH SPLENECTOMY
The efficacy of No. 10 lymph node dissection with splenectomy has not been proven. However, some disadvantages related to splenectomy have been reported [14]. It increases the incidence of postoperative complications, especially pancreatic fistula, infection caused by encapsulated bacteria, cancer, and postoperative thrombosis. Owing to these disadvantages, unnecessary splenectomy should be avoided.
Postoperative complications
Table 2 presents a list of the studies that have reported the association of splenectomy with morbidity and mortality. Three RCTs that compared the abovementioned prognostic outcomes also compared the mortality and morbidity rate between the groups. Csendes et al. [22] reported no significant difference in mortality between the splenectomy and spleen-preserving surgery groups (4.4% and 3.1%, respectively). The incidence of abdominal abscess was significantly higher in the splenectomy group (11% vs. 4%, respectively; P<0.05). Anastomotic leakage rate was similar in both groups, while none of the patients in either group developed any pancreatic complication. The overall complication rate was not reported by the authors. Galizia et al. [23] reported the details of complication. The overall complication rates in the splenectomy and spleen-preserving surgery groups were 48.6% and 19.4%. The respective incidence rates of other complications were as follows: anastomotic leakage, 5.4% and 5.5%; pancreatic fistula, 16.2% and 0%; and intraabdominal abscess, 10.8% and 2.7%. The mortality rates in the 2 groups were 5.4% and 0%, respectively. Although the authors did not report the statistical results, it seems that complications (except anastomotic leakage) were more common in the splenectomy group. Mortality event occurred only in the splenectomy group; however, the number of patients included in this study was small, and mortality event occurred only in 2 patients. Sano et al. [16] also reported a higher incidence of complications in the splenectomy group. The overall incidence of complications was 30.3% in the splenectomy group and 16.7% in the spleen-preserving surgery group (P<0.01). Anastomotic leakage rates were similar (4.3% and 3.2%, P=0.47), while pancreatic fistula was more frequent in the splenectomy group (12.6% and 2.4%, P<0.0001). Intraabdominal abscess was slightly more frequent in the splenectomy group (7.9% and 4%); however, the between-group difference was not statistically significant (P=0.089). Mortality rate was not significantly different between the 2 groups (0.4% and 0.8%, respectively). All these RCTs showed consistent results; that is, splenectomy increased the incidence of pancreatic fistula and intraabdominal abscess, but not that of anastomotic leakage or mortality.
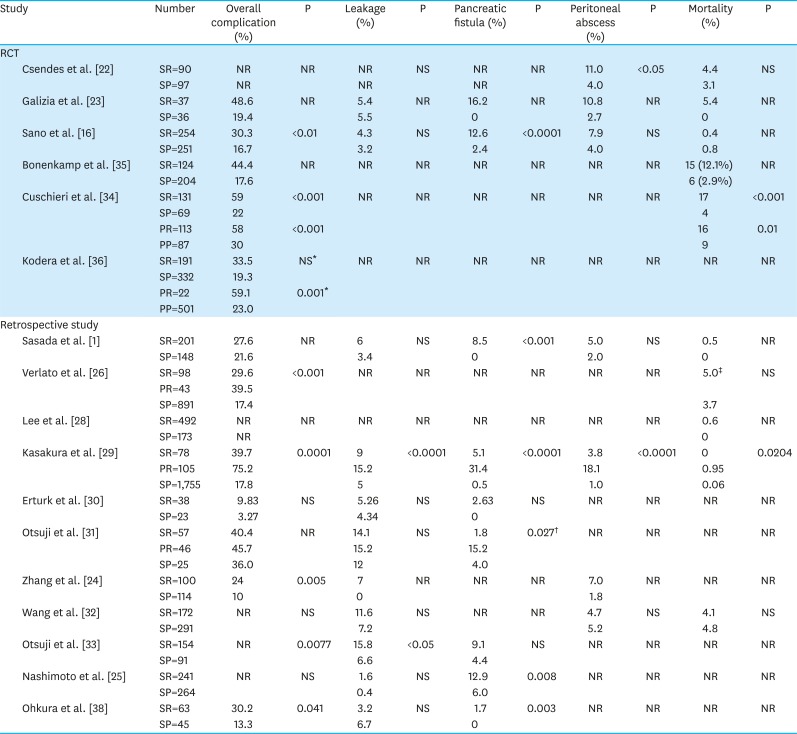
Table 2
Comparison of complications between splenectomy and spleen-preserving surgery without intentional No. 10 lymph node dissection
| Study | Number | Overall complication (%) | P | Leakage (%) | P | Pancreatic fistula (%) | P | Peritoneal abscess (%) | P | Mortality (%) | P | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RCT | ||||||||||||
| Csendes et al. [22] | SR=90 | NR | NR | NR | NS | NR | NR | 11.0 | <0.05 | 4.4 | NS | |
| SP=97 | NR | NR | NR | 4.0 | 3.1 | |||||||
| Galizia et al. [23] | SR=37 | 48.6 | NR | 5.4 | NR | 16.2 | NR | 10.8 | NR | 5.4 | NR | |
| SP=36 | 19.4 | 5.5 | 0 | 2.7 | 0 | |||||||
| Sano et al. [16] | SR=254 | 30.3 | <0.01 | 4.3 | NS | 12.6 | <0.0001 | 7.9 | NS | 0.4 | NR | |
| SP=251 | 16.7 | 3.2 | 2.4 | 4.0 | 0.8 | |||||||
| Bonenkamp et al. [35] | SR=124 | 44.4 | NR | NR | NR | NR | NR | NR | NR | 15 (12.1%) | NR | |
| SP=204 | 17.6 | 6 (2.9%) | ||||||||||
| Cuschieri et al. [34] | SR=131 | 59 | <0.001 | NR | NR | NR | NR | NR | NR | 17 | <0.001 | |
| SP=69 | 22 | 4 | ||||||||||
| PR=113 | 58 | <0.001 | 16 | 0.01 | ||||||||
| PP=87 | 30 | 9 | ||||||||||
| Kodera et al. [36] | SR=191 | 33.5 | NS* | NR | NR | NR | NR | NR | NR | NR | NR | |
| SP=332 | 19.3 | |||||||||||
| PR=22 | 59.1 | 0.001* | ||||||||||
| PP=501 | 23.0 | |||||||||||
| Retrospective study | ||||||||||||
| Sasada et al. [1] | SR=201 | 27.6 | NR | 6 | NS | 8.5 | <0.001 | 5.0 | NS | 0.5 | NR | |
| SP=148 | 21.6 | 3.4 | 0 | 2.0 | 0 | |||||||
| Verlato et al. [26] | SR=98 | 29.6 | <0.001 | NR | NR | NR | NR | NR | NR | 5.0‡ | NS | |
| PR=43 | 39.5 | |||||||||||
| SP=891 | 17.4 | 3.7 | ||||||||||
| Lee et al. [28] | SR=492 | NR | NR | NR | NR | NR | NR | NR | NR | 0.6 | NR | |
| SP=173 | NR | 0 | ||||||||||
| Kasakura et al. [29] | SR=78 | 39.7 | 0.0001 | 9 | <0.0001 | 5.1 | <0.0001 | 3.8 | <0.0001 | 0 | 0.0204 | |
| PR=105 | 75.2 | 15.2 | 31.4 | 18.1 | 0.95 | |||||||
| SP=1,755 | 17.8 | 5 | 0.5 | 1.0 | 0.06 | |||||||
| Erturk et al. [30] | SR=38 | 9.83 | NS | 5.26 | NS | 2.63 | NS | NR | NR | NR | NR | |
| SP=23 | 3.27 | 4.34 | 0 | |||||||||
| Otsuji et al. [31] | SR=57 | 40.4 | NR | 14.1 | NS | 1.8 | 0.027† | NR | NR | NR | NR | |
| PR=46 | 45.7 | 15.2 | 15.2 | |||||||||
| SP=25 | 36.0 | 12 | 4.0 | |||||||||
| Zhang et al. [24] | SR=100 | 24 | 0.005 | 7 | NR | NR | NR | 7.0 | NR | NR | NR | |
| SP=114 | 10 | 0 | 1.8 | |||||||||
| Wang et al. [32] | SR=172 | NR | NS | 11.6 | NS | NR | NR | 4.7 | NS | 4.1 | NS | |
| SP=291 | 7.2 | 5.2 | 4.8 | |||||||||
| Otsuji et al. [33] | SR=154 | NR | 0.0077 | 15.8 | <0.05 | 9.1 | NS | NR | NR | NR | NR | |
| SP=91 | 6.6 | 4.4 | ||||||||||
| Nashimoto et al. [25] | SR=241 | NR | NS | 1.6 | NS | 12.9 | 0.008 | NR | NR | NR | NR | |
| SP=264 | 0.4 | 6.0 | ||||||||||
| Ohkura et al. [38] | SR=63 | 30.2 | 0.041 | 3.2 | NS | 1.7 | 0.003 | NR | NR | NR | NR | |
| SP=45 | 13.3 | 6.7 | 0 | |||||||||
RCT, randomized controlled trial; SR, spleen resection; SP, spleen preservation; PR, pancreatic resection; PP, pancreatic preservation; NR, not reported; NS, not significant.
*P<0.001 on univariate analysis; †SP vs. SR and PR; ‡SP and PR.
![]()
Some RCTs investigated the adequate extent of lymph node dissection and assessed the relationship between complications and splenectomy. Cuschieri et al. [34] and Bonenkamp et al. [35] compared D1 and D2 lymphadenectomy in the Western population. The former included 131 patients who underwent splenectomy and 69 patients who underwent spleen-preserving surgery in the D2 group. The complication rates were 59% and 22%, respectively (P<0.001), and the mortality rates were 17% and 4%, respectively (P<0.001). The splenectomy group showed worse morbidity and mortality. Similarly, in the study by Bonenkamp et al. [35], the overall morbidity and mortality rates were 44.4% and 12.1%, respectively, in the splenectomy group and 17.6% and 2.9%, respectively, in the spleen-preserving surgery group. These trials demonstrated an unfavorable effect of splenectomy on morbidity and mortality. However, it is noteworthy that the morbidity and mortality rates in these studies were extremely high. These trials were conducted in Western countries that have a relatively low incidence of gastric cancer; moreover, the studies were conducted >20 years ago. Low hospital volume and shortage of experience on D2 lymphadenectomy may have affected the outcomes. In contrast, Kodera et al. [36] presented a detailed analysis of JCOG9501 [37], which compared D2 and D2 + paraaortic lymph node dissection, to clarify the risk factors for complications. They found that splenectomy did not have an effect on the morbidity rate. The overall complication rates in the splenectomy and spleen-preserving surgery groups were 33.5% and 19.3%, respectively. In the univariate analysis, the between-group difference was statistically significant (P<0.001); however, this was not the case in the multivariate analysis (P=0.304). The overall complication rates were relatively high in this study. However, the criteria for complications were not well defined in this study; therefore, comparison of results with other studies is not straightforward. This trial included patients who underwent paraaortic lymph node dissection. This procedure tends to increase the morbidity and may have affected the results of the multivariate analysis.
Most retrospective studies also showed the negative impact of splenectomy on morbidity. Eleven studies reported the association of splenectomy with morbidity or mortality [124252628293031323338]. Five studies showed a significant negative effect of splenectomy on overall morbidity, while 3 studies showed no significant between-group difference. Anastomotic leakage was more frequent only in 2 studies, while 6 studies found no significant between-group difference. Intraabdominal abscess was reported in only 4 studies, and 2 of these found no significant between-group difference. In contrast, the incidence of pancreatic fistula seemed to be affected by splenectomy; 5 studies found unfavorable effect of splenectomy, while 2 studies found no significant between-group difference. Both RCTs and retrospective studies showed a similar trend; namely, splenectomy increases the incidence of pancreatic fistula and overall complication rate, although it does not affect the incidence of anastomotic leakage. Splenectomy entails manipulation of the pancreas and mobilization of the pancreatic tail, which increases the risk of pancreatic injury. Moreover, ligation of the splenic artery proximal to the great pancreatic artery renders the pancreatic tail vulnerable to ischemia, leading to pancreatic fistula. Mortality rate was similar in all these studies. Advances in the treatment of major surgical complications have helped decrease the mortality rate.
Overwhelming post-splenectomy infection (OPSI)
The spleen has a crucial role in immunity by removing bacteria and antigen-antibody complexes from the bloodstream. The spleen also stimulates the production of immunoglobulin (Ig) M protein and antibodies against pneumococcal capsular polysaccharide, which facilitate phagocytosis by opsonization. Encapsulated organisms (e.g., Streptococcus pneumoniae, Haemophilus influenza, and Neisseria meningitidis) evade phagocytosis if they are not opsonized. Therefore, patients who underwent splenectomy are vulnerable to infection by encapsulated pathogens. Among these, S. pneumoniae is the most frequent cause of severe infection [3940]. OPSI is a serious disease developing in patients who underwent splenectomy. It is a fulminant condition associated with an extremely high mortality rate (36%–69%) [41]; therefore, prophylaxis against OPSI is quite important for these patients. All patients who underwent splenectomy are recommended to receive pneumococcal vaccine, H. influenzae type b vaccine, and meningococcal vaccine [42]. However, vaccination does not eliminate the risk of OPSI as these vaccines do not target all subtypes. A patient who underwent splenectomy has to live with the risk of OPSI and need to undergo regular vaccination. Splenectomy should be avoided if it does not confer a distinct advantage during gastric cancer surgery.
Relationship to development of cancer
The important role of immune function in cancer development has been increasingly recognized recently. Immune checkpoint inhibitors are currently used in patients with gastric cancer. The spleen is one of the most important organs for immunological function, and its role in cancer development or cancer suppression has been investigated recently. The effect of splenectomy on cancer is unclear. A large observational study investigated the relationship between splenectomy and cancer development [14]. If splenectomy increases the risk of cancer development, prophylactic splenectomy should be avoided. We reviewed the studies that investigated this subject. Three studies compared the risk of cancer development between patients who underwent splenectomy and those with functioning spleen [434445]. Patients who underwent splenectomy were divided into 2 groups; splenectomy performed due to trauma and splenectomy performed for other reasons. Mellemkjoer et al. [43] found that the risk of cancer development did not increase in 1,103 patients who underwent splenectomy due to trauma (relative risk [RR], 1.0; 95% confidence interval [CI], 0.6–1.6). In contrast, patients who underwent splenectomy due to other conditions showed a higher risk of malignant neoplasms (RR, 2.2; 95% CI, 1.6–2.9). The most common neoplasms were lung cancer, non-melanoma skin cancer, and leukemia. Sun et al. [44] reported similar results. The hazard ratio (HR) for overall cancer was 1.29 (95% CI, 1.05–1.6) in patients with trauma and 2.64 (95% CI, 2.30–3.05) in patients without trauma compared with patients who did not undergo splenectomy. The incidence rates of esophageal, gastric, and liver cancers and non-Hodgkin's lymphoma were increased in both groups. In a study by Linet et al. [45], the standardized incidence rates were 1.1 (95% CI, 0.8–1.5) in patients with trauma and 1.4 (95% CI, 1.1–1.6) in patients without trauma. All these studies showed that patients who underwent splenectomy tend to have a risk of cancer development; the risk is especially noticeable in patients who underwent splenectomy due to conditions other than trauma. Some studies have investigated the relationship between the immune system and splenectomy associated with gastric cancer. Saji et al. [46] reported 2 distinct patterns of the effect of splenectomy on post-gastrectomy survival, based on the levels of immunosuppressive acid protein (IAP). This study included 253 patients with gastric cancer. Patients who underwent splenectomy with low preoperative serum IAP level (<580 μg/mL) (which reflects positive antitumor immune reactions) showed a higher mortality rate (risk ratio=1.35 versus patients without splenectomy). Splenectomy had a negative effect in these patients. However, in the high IAP group (≥580 μg/mL), mortality rate was similar between the splenectomy and spleen-preserving surgery groups (risk ratio=2.26 and 2.24, respectively). Thus, splenectomy had a positive effect in patients with high IAP levels. Immunotherapy was also affected by the IAP levels and splenectomy. In case of low IAP levels, immunotherapy showed favorable effect, and the effect was greater in the spleen-preserving surgery group. However, in the high IAP group, immunotherapy had some negative effects in patients with preserved spleen and better results in patients who underwent splenectomy. They concluded that the spleen exhibits biphasic activity in terms of antitumor immune response depending on the IAP level. Some studies focused on circulating T-lymphocyte subsets after splenectomy in patients with gastric cancer [4748]. Cho et al. [47] investigated the proportion of lymphocytes in 40 patients with stage III gastric cancer who underwent curative total gastrectomy with or without splenectomy. They compared the CD3, CD4, CD8, CD16, CD19, and CD25 levels between the 2 groups. The 5-year DFS rate was comparable in the splenectomy and spleen-preserving surgery groups (52.4% and 50.0%, respectively). CD3, CD8, and CD25 levels were significantly higher in the splenectomy group only at 3 postoperative months. CD16 level was significantly higher in the splenectomy group after 3 postoperative months. CD4 level was significantly lower in the splenectomy group only at 3 postoperative months. CD19 showed no difference at any time during the observation period. Only CD16 level was significantly different in the long term. These findings suggest that patients who underwent splenectomy have more natural killer cells, while there was no survival or oncological benefit from splenectomy. The authors concluded that splenectomy did not affect postoperative survival. Pan et al. [48] compared the CD3, CD4, CD8, IgG, IgA, and IgM levels in the splenectomy and spleen-preserving surgery groups consisting of patients with stage IV gastric cancer who underwent palliative surgery. After 6 postoperative months, all these immune indices, except CD8, were significantly lower in the splenectomy group. However, there was no significant between-group difference in survival, and the role of these immune indices is uncertain.
These reports suggest that splenectomy influences the immune system. While it is not related with cancer recurrence, it may affect other cancer developments in the long term. Splenectomy may also potentially affect the efficacy of immunotherapy. The details of the changes in the immune system after splenectomy or the effect of splenectomy on some treatments are still unclear. Further studies in this field may help assess the importance of splenectomy.
Post-splenectomy thrombosis
Thrombosis is a critical and potentially fatal complication. Few studies have investigated the relationship between thrombosis and splenectomy performed concomitantly with gastrectomy for gastric cancer; however, splenectomy has been shown to increase the risk of thrombosis. Virchow's triad (hypercoagulability, hemodynamic changes, and endothelial injury) refers to the 3 main factors that contribute to thrombosis. Malignancy is believed to contribute to hypercoagulability, and splenectomy itself may be an independent factor for hypercoagulative status. Pommerening et al. [49] used serial rapid thromboelastography and demonstrated that splenectomy is associated with hypercoagulable state at least 120 hours postoperatively. They also reported a higher rate of thromboembolic complications in patients who underwent splenectomy (17.5% vs. 7.8%; P=0.015). Although this study included only patients with trauma and the operative situation is different from that of elective surgery, this study showed the relationship between splenectomy and hypercoagulability. Mukherjee et al. [50] compared the risk of venous thromboembolism according to the type of surgery. They compared bariatric surgery, colorectal surgery, esophagectomy, gastrectomy, hepatectomy, nephrectomy, pancreatectomy, and splenectomy. This study had an extremely large sample size that involved 375,748 patients. The odds ratio (OR) for venous thromboembolism was the highest in patients who underwent splenectomy (OR, 2.69; 95% CI, 2.03–3.56) even after adjusting for age, sex, year, Charlson score, length of stay, hospital teaching status, elective procedure status, trauma, and malignancy. However, the authors did not control the prophylactic use of anticoagulants in their analysis. As a result, bariatric surgery, which increases the risk for thrombosis, showed the lowest risk of thromboembolism probably due to anticoagulant use. Whether splenectomy had the highest risk among the procedures is uncertain. However, this study showed that splenectomy is a risk factor for postoperative thrombosis.
Splenectomy may be related to not only deep venous thrombosis (DVT) and pulmonary embolism (PE) but also portomesenteric venous thrombosis (PMVT). In the study by Boyle et al., the incidence rates of both DVT/PE and PMVT were increased after splenectomy [51]. They retrospectively analyzed data of 9,976 patients with immune thrombocytopenia. They compared cumulative incidence of DVT/PE and PMVT between patients who underwent splenectomy and those who did not undergo splenectomy. The incidence rates of DVT/PE in patients who underwent splenectomy and those who did not undergo splenectomy were 4.3% and 1.7%, respectively (P<0.0001). The corresponding incidence rate of PMVT were 1.6% and 1%, respectively (P=0.0544). They also focused on the time elapsed between surgery and the development of thrombosis. They defined <90 days after surgery as early thrombosis and ≥90 days as late thrombosis. Regarding PMVT, splenectomy was associated with increased HR for early PMVT (HR, 5.4; 95% CI, 2.3–12.5) but not for late PMVT (HR, 1.5; 95% CI, 0.9–2.6). In contrast, splenectomy increased the incidence of both early and late DVT/PE (HR, 5.2; 95% CI, 3.2–8.5; HR, 2.7; 95% CI, 1.9–3.8). These findings suggest that we should prevent both PMVT and DVT/PE in the early phase after splenectomy and DVT/PE even in the late phase. In a study by Han et al. [52], 31 of 4611 patients (0.67%) who underwent gastric surgery developed PMVT. In the multivariate analysis, advanced gastric cancer stage (RR, 2.236; 95% CI, 1.017–4.919), synchronous malignancies (RR, 29.236; 95% CI, 10.451–81.785), and splenectomy (RR, 8.563; 95% CI, 3.233–22.648) were independent risk factors for PMVT. In addition to the systemic factors (hypercoagulability), the procedure for splenectomy per se has some locoregional effects (hemodynamic changes and endothelial injury). Splenectomy entails manipulation of the splenic or portal vein and mobilization of the distal pancreas. The former procedure may cause endothelial injury during clamping of the vessels by tweezers, and the latter procedure tends to induce hemodynamic changes. Postoperative pancreatic fistula may also be related with PMVT due to the inflammation around the splenic vein, leading to a hypercoagulative state. As a result, PMVT tends to develop in the early phase [5153].
Extremely few studies have assessed the relationship between splenectomy performed in conjunction with gastric cancer surgery and thrombosis. Theoretically, splenectomy increases the risk of thrombosis; however, the increased risk of thrombosis has been reported only in patients who underwent splenectomy for reasons other than gastric cancer surgery. Thrombosis is a rare but potentially fatal complication. We should be conscious of this complication in the long period after splenectomy.
Go to :
IS SPLENECTOMY NOT NEEDED ANYMORE?
Several disadvantages of splenectomy have been reported. However, there are some situations wherein it would be better to perform splenectomy during gastric cancer surgery.
Risk factors for No. 10 lymph node metastasis
The therapeutic effect of splenectomy has not been adequately evaluated. In most studies that compared splenectomy and spleen-preserving surgery, patients with direct invasion of the spleen or those with obvious No. 10 lymph node metastasis were excluded. Huang et al. [54] retrospectively compared patients with No. 10 lymph node metastasis who underwent splenectomy (n=73) or spleen-preserving surgery with No. 10 lymph node dissection (n=143). The 5-year OS in the 2 groups were 30% and 19.7%, respectively (P<0.0001). This study suggested that splenectomy may be effective as a therapeutic intervention. It is also important to be conscious of the pattern of No. 10 lymph node metastasis. Table 3 shows the studies that reported clinicopathological characteristics and risk factors for No. 10 lymph node metastasis. In several studies, type 4 tumor, tumor invading the greater curvature, deep invasion into the gastric wall, and presence of lymph node metastasis were related to No. 10 lymph node metastasis. More advanced cancer is typically associated with more extensive lymph node metastasis. The No. 10 lymph node is located near the greater curvature. From the perspective of lymphatic drainage, No. 10 lymph node metastasis will occur through No. 4sa or 4sb lymph nodes located along the greater curvature. On the contrary, in case of tumors located in the lesser curvature, the cancer cells will have to pass through many lymph nodes, like No. 1 and 3 lymph nodes to No. 7, 9, and 11 lymph nodes to reach the No. 10 lymph node. It is important to verify the necessity of splenectomy in patients with advanced proximal gastric cancer with invasion of the greater curvature.
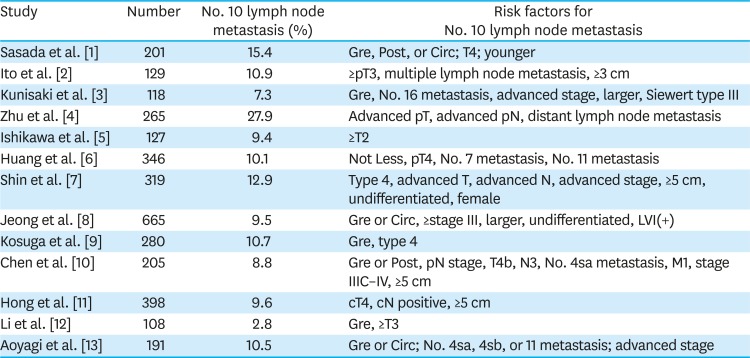
Table 3
Risk factors for No. 10 lymph node metastasis
| Study | Number | No. 10 lymph node metastasis (%) | Risk factors for No. 10 lymph node metastasis |
|---|---|---|---|
| Sasada et al. [1] | 201 | 15.4 | Gre, Post, or Circ; T4; younger |
| Ito et al. [2] | 129 | 10.9 | ≥pT3, multiple lymph node metastasis, ≥3 cm |
| Kunisaki et al. [3] | 118 | 7.3 | Gre, No. 16 metastasis, advanced stage, larger, Siewert type III |
| Zhu et al. [4] | 265 | 27.9 | Advanced pT, advanced pN, distant lymph node metastasis |
| Ishikawa et al. [5] | 127 | 9.4 | ≥T2 |
| Huang et al. [6] | 346 | 10.1 | Not Less, pT4, No. 7 metastasis, No. 11 metastasis |
| Shin et al. [7] | 319 | 12.9 | Type 4, advanced T, advanced N, advanced stage, ≥5 cm, undifferentiated, female |
| Jeong et al. [8] | 665 | 9.5 | Gre or Circ, ≥stage III, larger, undifferentiated, LVI(+) |
| Kosuga et al. [9] | 280 | 10.7 | Gre, type 4 |
| Chen et al. [10] | 205 | 8.8 | Gre or Post, pN stage, T4b, N3, No. 4sa metastasis, M1, stage IIIC–IV, ≥5 cm |
| Hong et al. [11] | 398 | 9.6 | cT4, cN positive, ≥5 cm |
| Li et al. [12] | 108 | 2.8 | Gre, ≥T3 |
| Aoyagi et al. [13] | 191 | 10.5 | Gre or Circ; No. 4sa, 4sb, or 11 metastasis; advanced stage |
Gre, greater curvature; Post, posterior; Circ, circumferential; Less, lesser curvature; LVI, lymphovascular invasion.
![]()
Table 4 shows the studies that investigated this issue. Five studies [89555657] used therapeutic value index (TVI) to evaluate the efficacy of splenectomy in patients with advanced gastric cancer with greater curvature invasion. TVI is calculated by multiplying the incidence of No. 10 lymph node metastasis by the 5-year survival rate of patients with No. 10 lymph node metastasis. Four studies compared TVI between patients with invasion of the greater curvature (Gre group) and those with no invasion of the greater curvature (non-Gre group). In these studies, the incidence rate of No. 10 lymph node metastasis in the Gre group ranged from 13.4% to 24.1%, which was higher than the overall metastatic rate. TVI was also higher in the Gre group. All authors concluded that splenectomy may be effective in the Gre group. However, they did not directly compare patients with greater curvature invasion in the splenectomy and spleen-preserving surgery groups. Therefore, no definitive conclusions can be drawn from these studies.
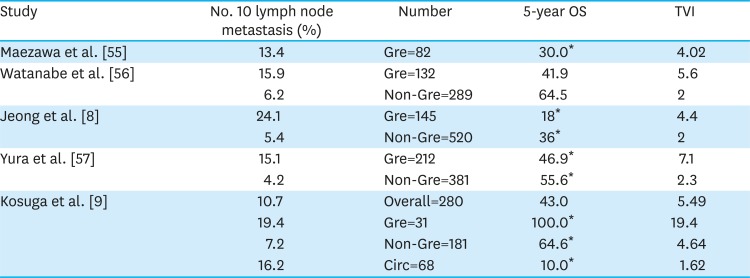
Table 4
Studies discussing the efficacy of splenectomy in patients with gastric cancer with greater curvature invasion
| Study | No. 10 lymph node metastasis (%) | Number | 5-year OS | TVI |
|---|---|---|---|---|
| Maezawa et al. [55] | 13.4 | Gre=82 | 30.0* | 4.02 |
| Watanabe et al. [56] | 15.9 | Gre=132 | 41.9 | 5.6 |
| 6.2 | Non-Gre=289 | 64.5 | 2 | |
| Jeong et al. [8] | 24.1 | Gre=145 | 18* | 4.4 |
| 5.4 | Non-Gre=520 | 36* | 2 | |
| Yura et al. [57] | 15.1 | Gre=212 | 46.9* | 7.1 |
| 4.2 | Non-Gre=381 | 55.6* | 2.3 | |
| Kosuga et al. [9] | 10.7 | Overall=280 | 43.0 | 5.49 |
| 19.4 | Gre=31 | 100.0* | 19.4 | |
| 7.2 | Non-Gre=181 | 64.6* | 4.64 | |
| 16.2 | Circ=68 | 10.0* | 1.62 |
OS, overall survival; TVI, therapeutic value index.
*OS in patients with No. 10 lymph node metastasis.
![]()
One retrospective study [38] compared patients with advanced proximal gastric cancer with greater curvature invasion in the splenectomy and spleen-preserving surgery groups. The clinicopathological features were comparable between the 2 groups. The 5-year OS of patients in the splenectomy and spleen-preserving surgery groups was 63.7% and 73.6%, respectively. This study suggested that splenectomy is unnecessary even in patients in the Gre group. However, the metastatic rate was only 6% and lower than that in other studies. Besides, 76% of patients in the spleen-preserving surgery group underwent No. 10 lymph node dissection or pickup. These factors probably affected the outcome, and it does not imply that No. 10 lymph node dissection is unnecessary. Advanced gastric cancer with greater curvature invasion is a risk factor of No. 10 lymph node metastasis, and these patients may benefit from No. 10 lymph node dissection.
Patients with remnant gastric cancer
Since remnant gastric cancer is a relatively rare disease, the efficacy of splenectomy on remnant gastric cancer is inadequately discussed. The lymphatic pathways tend to change especially after surgery for malignant cancer. Dissection of lymph nodes along the lesser curvature during initial surgery will hinder the lymphatic drainage of the lesser curvature and lead to the development of an alternative lymphatic pathway to the splenic hilar nodes [5859]. This change may increase the incidence of No. 10 lymph node metastasis, and splenectomy may have a beneficial effect in these patients. A few studies have investigated the efficacy of splenectomy in the context of remnant gastric cancer surgery. Sugita et al. [60] analyzed the effect of splenectomy. In the T1/2 group, there were no No. 10 lymph node metastasis and no difference in 5-year OS. However, in the T3/4 population, the No. 10 lymph node metastatic rate was 30.4%, which was higher than that observed in the context of primary cancer. Moreover, the 5-year OS was significantly better in the splenectomy group (P<0.05). Although the authors did not stratify the patients by disease stage, patients with advanced remnant gastric cancer may benefit from splenectomy. Ohashi et al. [61] also reported the potentially therapeutic benefit of dissection of splenic hilar nodes. They included patients with T2–4 remnant gastric cancer after surgery for malignancy; the TVI in these patients (3.38) was higher than that for other lymph node stations. In contrast, Son et al. [58] found that splenectomy did not have an effect on survival outcomes. In the subgroup analysis disaggregated by disease stage, they found no significant difference between the splenectomy and non-splenectomy groups. In this study, patients with both benign and malignant diseases at initial surgery were included. Furthermore, there was a relatively low number of patients with advanced remnant gastric cancer, who may have benefited from splenectomy.
Theoretically, it seems better to perform splenectomy in patients with remnant gastric cancer especially after surgery for malignancy with lesser curvature dissection. However, further study is warranted to obtain definitive evidence in this regard.
Go to :
NO. 10 LYMPH NODE DISSECTION WITHOUT SPLENECTOMY
Splenectomy is the standard treatment for advanced gastric cancer invading the greater curvature. However, owing to the aforementioned disadvantages, the indication for splenectomy should be carefully considered. In a therapeutic situation, splenectomy may be effective [54], while prophylactic splenectomy in patients in the Gre group (high risk for metastasis) is still controversial. Several recent studies have investigated spleen-preserving No. 10 lymph node dissection [6263646566676869707172]. However, whether this procedure allows for adequate dissection is also controversial. Spleen-preserving No. 10 lymph node dissection is desirable if it is as effective as splenectomy and overcomes the disadvantages of splenectomy. Table 5 shows the studies that compared splenectomy and spleen-preserving No. 10 lymph node dissection. None of these studies showed a beneficial effect of splenectomy. Spleen-preserving No. 10 lymph node dissection did not seem to worsen the OS. There is one RCT among these studies. Yu et al. [70] randomly assigned 207 patients to the splenectomy and spleen-preserving No. 10 lymph node dissection groups. The 5-year OS was comparable in the 2 groups (54.8% and 48.8%, respectively; P=0.503). In other retrospective studies, splenectomy showed either a negative impact or no impact on survival. However, the splenectomy group tended to include more advanced cancer, and this bias should be taken into consideration. Huang et al. [73] had a different perspective. They retrospectively compared patients who underwent and did not undergo No. 10 lymph node dissection in the spleen-preserving surgery group. The 3-year DFS was significantly better in the dissection group in patients with stage III gastric cancer. This result suggests that No. 10 lymph node dissection without splenectomy is effective.
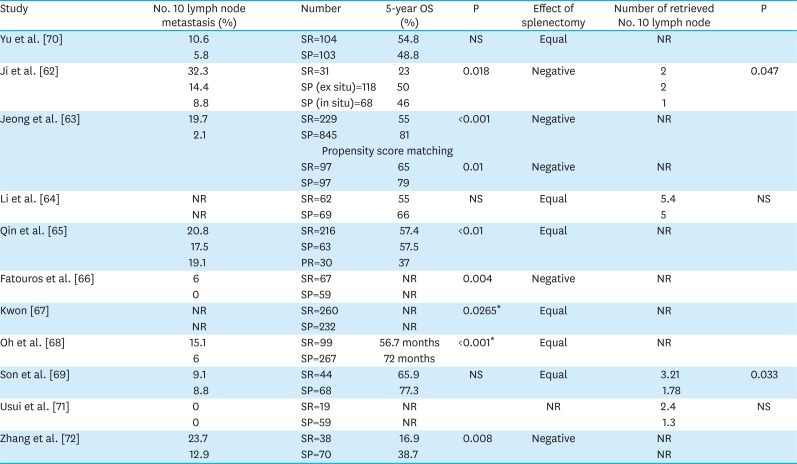
Table 5
Efficacy of splenectomy in spleen-preserving No. 10 lymph node dissection
| Study | No. 10 lymph node metastasis (%) | Number | 5-year OS (%) | P | Effect of splenectomy | Number of retrieved No. 10 lymph node | P |
|---|---|---|---|---|---|---|---|
| Yu et al. [70] | 10.6 | SR=104 | 54.8 | NS | Equal | NR | |
| 5.8 | SP=103 | 48.8 | |||||
| Ji et al. [62] | 32.3 | SR=31 | 23 | 0.018 | Negative | 2 | 0.047 |
| 14.4 | SP (ex situ)=118 | 50 | 2 | ||||
| 8.8 | SP (in situ)=68 | 46 | 1 | ||||
| Jeong et al. [63] | 19.7 | SR=229 | 55 | <0.001 | Negative | NR | |
| 2.1 | SP=845 | 81 | |||||
| Propensity score matching | |||||||
| SR=97 | 65 | 0.01 | Negative | NR | |||
| SP=97 | 79 | ||||||
| Li et al. [64] | NR | SR=62 | 55 | NS | Equal | 5.4 | NS |
| NR | SP=69 | 66 | 5 | ||||
| Qin et al. [65] | 20.8 | SR=216 | 57.4 | <0.01 | Equal | NR | |
| 17.5 | SP=63 | 57.5 | |||||
| 19.1 | PR=30 | 37 | |||||
| Fatouros et al. [66] | 6 | SR=67 | NR | 0.004 | Negative | NR | |
| 0 | SP=59 | NR | |||||
| Kwon [67] | NR | SR=260 | NR | 0.0265* | Equal | NR | |
| NR | SP=232 | NR | |||||
| Oh et al. [68] | 15.1 | SR=99 | 56.7 months | <0.001* | Equal | NR | |
| 6 | SP=267 | 72 months | |||||
| Son et al. [69] | 9.1 | SR=44 | 65.9 | NS | Equal | 3.21 | 0.033 |
| 8.8 | SP=68 | 77.3 | 1.78 | ||||
| Usui et al. [71] | 0 | SR=19 | NR | NR | 2.4 | NS | |
| 0 | SP=59 | NR | 1.3 | ||||
| Zhang et al. [72] | 23.7 | SR=38 | 16.9 | 0.008 | Negative | NR | |
| 12.9 | SP=70 | 38.7 | NR | ||||
SR, spleen resection; SP, spleen preservation; PR, pancreatic resection; OS, overall survival; NR, not reported; NS, not significant.
*NS after stratification by stage.
![]()
Spleen-preserving No. 10 lymph node dissection necessarily involves manipulation of the distal pancreas, which increases the risk of postoperative morbidity. Table 6 shows the postoperative complication rate in the splenectomy and spleen-preserving dissection groups. Nine studies reported the total complication rate, and approximately half of these studies showed a significant increase in the splenectomy group. This result is similar to the results shown in Table 2. The total complication rate in the spleen-preserving No. 10 lymph node dissection ranged from 11.6% to 19.8%, and this rate was also similar to the results in the spleen-preserving surgery group shown in Table 2. Among the complications, the incidence of anastomotic leakage was not different in any of the studies, while the incidence of pancreatic fistula decreased with spleen preservation. This result suggests that No. 10 lymph node dissection did not increase the postoperative morbidity compared with spleen preservation without No. 10 lymph node dissection.
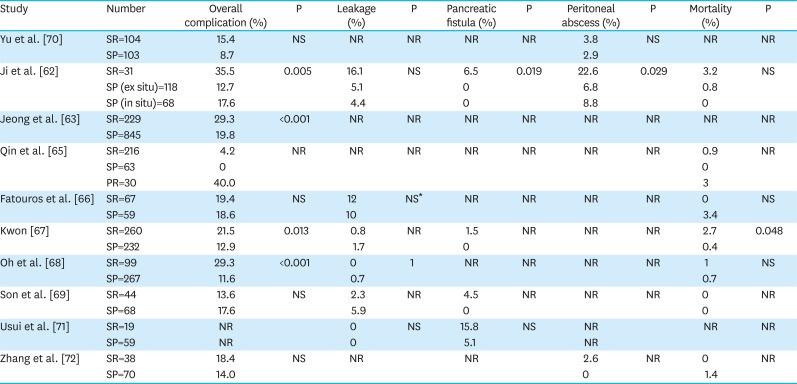
Table 6
Complications of splenectomy and spleen-preserving No. 10 lymph node dissection
| Study | Number | Overall complication (%) | P | Leakage (%) | P | Pancreatic fistula (%) | P | Peritoneal abscess (%) | P | Mortality (%) | P |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Yu et al. [70] | SR=104 | 15.4 | NS | NR | NR | NR | NR | 3.8 | NS | NR | NR |
| SP=103 | 8.7 | 2.9 | |||||||||
| Ji et al. [62] | SR=31 | 35.5 | 0.005 | 16.1 | NS | 6.5 | 0.019 | 22.6 | 0.029 | 3.2 | NS |
| SP (ex situ)=118 | 12.7 | 5.1 | 0 | 6.8 | 0.8 | ||||||
| SP (in situ)=68 | 17.6 | 4.4 | 0 | 8.8 | 0 | ||||||
| Jeong et al. [63] | SR=229 | 29.3 | <0.001 | NR | NR | NR | NR | NR | NR | NR | NR |
| SP=845 | 19.8 | ||||||||||
| Qin et al. [65] | SR=216 | 4.2 | NR | NR | NR | NR | NR | NR | NR | 0.9 | NR |
| SP=63 | 0 | 0 | |||||||||
| PR=30 | 40.0 | 3 | |||||||||
| Fatouros et al. [66] | SR=67 | 19.4 | NS | 12 | NS* | NR | NR | NR | NR | 0 | NS |
| SP=59 | 18.6 | 10 | 3.4 | ||||||||
| Kwon [67] | SR=260 | 21.5 | 0.013 | 0.8 | NR | 1.5 | NR | NR | NR | 2.7 | 0.048 |
| SP=232 | 12.9 | 1.7 | 0 | 0.4 | |||||||
| Oh et al. [68] | SR=99 | 29.3 | <0.001 | 0 | 1 | NR | NR | NR | NR | 1 | NS |
| SP=267 | 11.6 | 0.7 | 0.7 | ||||||||
| Son et al. [69] | SR=44 | 13.6 | NS | 2.3 | NR | 4.5 | NR | NR | NR | 0 | NR |
| SP=68 | 17.6 | 5.9 | 0 | 0 | |||||||
| Usui et al. [71] | SR=19 | NR | 0 | NS | 15.8 | NS | NR | NR | NR | ||
| SP=59 | NR | 0 | 5.1 | NR | |||||||
| Zhang et al. [72] | SR=38 | 18.4 | NS | NR | NR | 2.6 | NR | 0 | NR | ||
| SP=70 | 14.0 | 0 | 1.4 |
SR, spleen resection; SP, spleen preservation; PR, pancreatic resection; NR, not reported; NS, not significant.
*Leakage and abscess.
![]()
Spleen-preserving No. 10 lymph node dissection did not worsen the prognosis and may decrease the complication rate. From these results, spleen-preserving No. 10 lymph node dissection would be a good surgical option for prophylactic dissection in advanced gastric cancer with greater curvature invasion, as an alternative to splenectomy.
Go to :
CONCLUSIONS
Splenectomy is performed in a therapeutic situation or prophylactic dissection in patients with high risk of splenic hilar metastasis. However, splenectomy has some disadvantages. It definitely increases the risk of pancreatic fistula, infection with encapsulated bacteria, and thromboembolic events. Besides, it also affects the immune system, which may have a negative effect on survival, e.g., increasing the risk of cancer development. Due diligence should be exercised to avoid splenectomy, whenever possible. Spleen-preserving No. 10 lymph node dissection might be an alternative treatment for high-risk patients. This treatment does not appear to worsen the prognosis but decreases the postoperative complication rate and prevents other problems associated with splenectomy. However, robust evidence on the efficacy of this procedure is lacking, and further trials comparing splenectomy and spleen-preserving No. 10 lymph node dissection in patients with greater curvature invasion are required.
Go to :
 XML Download
XML Download