

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The use of air purifiers is rapidly increasing due to increases in fine dust and respiratory diseases.1 Particulate matter with an aerodynamic diameter of 2.5 µm or less (PM2.5) is a principal component of indoor air pollution in homes and is a major cause of asthma exacerbation and lung dysfunction.23 With people spending most of their time indoors nowadays, there has been increasing interest in the practical effect of using air purifiers to improve indoor air pollution.
In South Korea, a recent study suggested that air purifiers may improve the severity of atopic dermatitis by reducing air pollutants and fine particles.4 However, no studies have analyzed the effects of air purifiers on children with asthma in South Korea. According to a recent study in Fresno, CA, air purifiers are effective in reducing indoor PM2.5 and significantly improve symptoms and peak flow rates in children with allergic diseases.5 However, the study was limited by the small number of study subjects and a very low basal PM2.5 levels in the city where the study was conducted. Also, recent evidence has indicated that microbial diversity and phthalate can exacerbate asthma.67
The purpose of this study was to evaluate the control of indoor air quality through the use of air purifier actually and its effects on Korean children with asthma. This study measured PM2.5 levels, asthma severity, lung function, and urine microbiome and phthalate concentrations.
MATERIALS AND METHODS
Patients and study setting
The participants consisted of elementary school students who were living in cities in the Incheon and Gyeonggi-do regions and who had been diagnosed with asthma at Inha Hospital. The diagnosis was determined according to the GINA guidelines.8 This study was conducted as a randomized, single-blind, cross-over study between September 3 and October 27, 2018 with a 2-week wash out period.
Inclusion/exclusion criteria
The inclusion criteria comprised at least two periods of asthma exacerbation in the last year. We excluded children who had been born during gestational week 34 or earlier, children with a birth weight of 2.5 kg or lower, children with a congenital deformity, children with immune dysfunction, and cases where consent to participate was not given.
Intervention
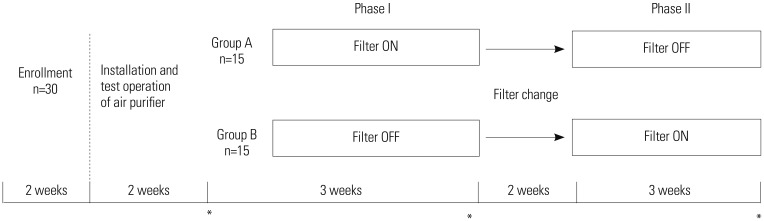
A total of 30 asthma patients were randomly allocated to Group A (n=15) or Group B (n=15) (Fig. 1). The 30 households participating in the study installed an air purifier (TOWER XQ; Winix, Siheung, South Korea) in the living room, where the children spent most of their time. Participants were instructed to use the air purifier 24 hours per day, every day, for 6 weeks. The air purifiers operated normally throughout the study period, without any problems. Group A used the air purifier with a filter for the first 3 weeks, while Group B used the air purifier without a filter during that time, so that it did not provide any actual function. Following a 2-week filter change period, the groups were changed over the next 3 weeks (Supplementary Table 1, only online).
Outcome measurement
We compared indoor PM2.5, carbon dioxide (CO2) concentration, relative humidity, and temperature before and after air purifier use. We also examined whether there were any changes in asthma symptoms and frequency of medication use. To compare lung function and airway inflammation, we measured peak expiratory flow rate (PEFR) and fractional exhaled nitric oxide (FeNO). In addition, we analyzed changes in microbes and phthalate metabolites in urine.
Indoor air quality
Indoor air quality data, including PM2.5, CO2, temperature, relative humidity, were obtained using ESCORT (ESCORT, Asan, Korea). PM2.5 concentrations were measured through a laserlight scattering sensor at 2-minute intervals in each household's main living space. Then, to match our health symptom data, we calculated daily mean values. We also evaluated the performance of a real-time PM2.5 sensor, compared with the US EPA Federal Equivalent Method.9
Asthma control questionnaire
To objectively measure symptom improvements and changes in medication use after air purifier use, we had the participants complete the asthma control questionnaire every day. The asthma control questionnaire used in this study was based on the Test for Respiratory and Asthma Control in Kids (TRACK)10 (Supplementary Tables 2 and 3, only online). The response to each question was scored, with higher scores indicating greater improvement in symptoms and a lower frequency of medication use.
Lung function test
We used PEFR as surrogate marker for lung function. The PEFR measurement was performed using Smart One® (Medical International Research; Roma, Italy). Portable measuring instruments were distributed to the study subjects, and measurements were taken three times each morning and evening, the highest value of which was recorded. Measurements were linked to mobile phone applications, and data were extracted for each follow-up visit.
Airway inflammatory test
We used FeNO as a surrogate marker for airway inflammation. FeNO was measured at each follow-up visit using NIOX MINO® (Aerocrine, Solna, Sweden). To do so, the participant was asked to sit in a chair and, while wearing a nose plug, inhale nitric oxide-free air to maximum lung capacity. Then, while biting a mouthpiece and looking at a monitor, the participant exhaled at a constant rate of 50 mL/s. In accordance with the NIOX MINO® instruction manual, the test was performed once using the method in the ATS/ERS guidelines11 and repeated in the event of errors.
Isolation of microbiome extracellular vesicles and DNA extraction from urine
Two milliliters of voided clean catch midstream urine were collected and stored at −20℃. To isolate the extracellular vesicles, urine samples underwent differential centrifugation by a micro-centrifuge at 10000×g for 10 minutes at 4℃.12 The supernatant was then filtered through a 0.22-µm filter to eliminate bacteria and foreign particles. For DNA extraction, isolated extracellular vesicles were boiled at 100℃ for 40 minutes and centrifuged at 13000 rpm for 30 minutes at 4℃ to eliminate the remaining floating particles and waste. Subsequently, the supernatant was collected and subjected to DNA isolation using a FastDNA® SPIN Kit for Soil (MP Biomedicals, Solon, OH, USA) according to the standard protocol for DNA extraction. The DNA in each sample was quantified using an Epoch™ Spectrophotometer system (BioTek Instruments, Winooski, VT, USA).
16S rDNA sequencing and taxonomic assignment
Bacterial genomic DNA PCR amplification was executed with primers specific for V3–V4 hypervariable regions of the 16S rDNA gene. The amplicons were pooled, and the sequencing was carried out at ChunLab, Inc. (Seoul, Korea), with a MiSeq Sequencing system (Illumina Inc., San Diego, CA, USA) according to the manufacturer's instructions.
Raw reads were processed with quality check and filtering of low quality (<Q25) reads by Trimmomatic 0.32.13 After passing quality control, paired-end sequence data were merged together using PANDAseq.14 Primers were then trimmed with a ChunLab in-house program at a similarity cut off of 0.8. Non-specific amplicons that do not encode 16S rRNA were detected by HMMER's hmmsearch program15 with 16S rRNA profiles. Sequences were denoised using DUDE-Seq,16 and non-redundant reads were extracted by UCLUST-clustering.17 The EzBio-Cloud database was used for taxonomic assignment using USEARCH (8.1.1861_i86linux32),17 followed by more precise pairwise alignment.18 UCHIME19 and the non-chimeric 16S rRNA database from EzBioCloud were used to detect chimera on reads that contained a less than 97% best hit similarity rate. Sequence data were then clustered using CD-HIT20 and UCLUST.17 The alpha diversity indices and rarefaction curves were estimated by in-house code.
Urine phthalate
For analysis of monophthalates, we focused on mono-n-butylphthalate, mono-(2-ethyl-5-hydroxyhexyl) phthalate, mono-(2-ethyl-5-oxohexyl) phthalate, mono-(2-ethyl-5-carboxylpentyl) phthalate, and mono-benzylphthalate, which are widely used metabolites of di-n-butyl phthalate (DnBP), di(2-ethylhexyl) phthalate (DEHP), and butylbenzyl phthalate (BBzP). After collection, urine specimens were frozen at −70℃ until analyzed. Samples were thawed at room temperature before pretreatment. In an 8-mL glass vial, 1 mL of 2 M sodium acetate and 20 µL of β-glucuronidase were added to 500 µL of each urine sample. After vortexing for 10 minutes using a large vortexer, the mixture was incubated at 37℃ for 16 hours to hydrolyze the phthalate metabolite complexes. After adding 100 µL of 2 M HCl, 50 µL of internal standard, and 4 mL of ethyl acetate and vortexing for 15 minutes, the solution was centrifuged for 5 minutes at 3000 rpm. The supernatant was collected for analysis, with care being taken not to disturb the solid at the bottom of the tube. The quantity of phthalate metabolites in the samples was measured using LC-MS/MS.
RESULTS
A total of 30 children were randomized and evenly assigned to two groups. All of them completed the study without any complications. The mean age of the enrolled patients was 9.20±1.98 years (minimum–maximum age: 6.08–12.41 years). Baseline characteristics, including sex, age, height, weight, body mass index, FeNO, forced expiratory volume in 1 second (FEV1), immunoglobulin E (IgE), and allergen sensitization, are summarized in Table 1 and Supplementary Table 4 (only online).
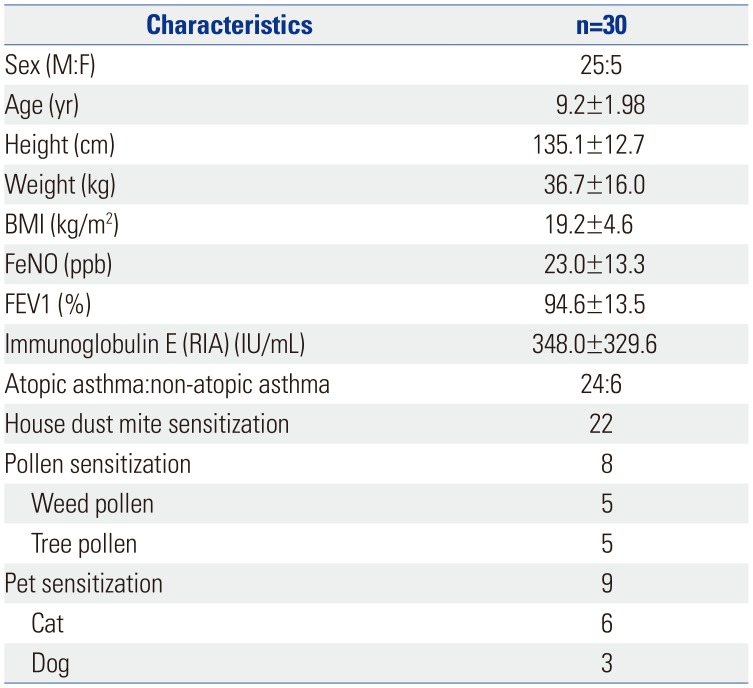
Table 1
Baseline Characteristics of the Study Population
![]()
Indoor air pollutant concentration
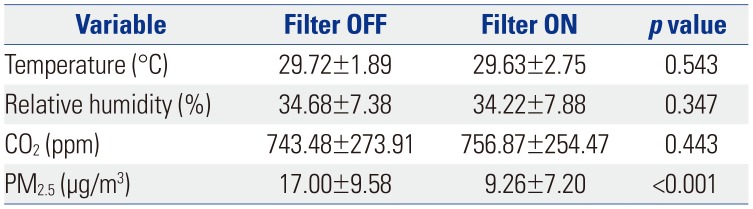
PM2.5 and CO2 concentrations were measured to assess indoor air pollution. The mean levels of PM2.5 were 17 µg/m3 with the filter off and 9.26 µg/m3 with the filter on, indicating a statistically significant decrease when the air purifier was used (p<0.001) (Table 2). However, CO2 concentration, relative humidity, and temperature showed no significant differences depending on air purifier use (Supplementary Table 5, only online).
Asthma symptoms, medication use, and PEFR
Symptom scores were 14.03 in the filter-off condition and 13.97 in the filter-on condition, with no significant difference between the two (Table 3). Medication scores were 6.9 in the filter-off condition and 7.12 in the filter-on condition, reflecting a statistically significant decrease in the use of anti-asthmatic medications when the air purifier was used (p<0.001) (Table 3). PEFRs were 326.24 L/min in the filter-off condition and 321.33 L/min in the filter-on condition, which was not a statistically significant difference (Table 4).


FeNO, urine microbiome, and urine phthalate
FeNO levels were 27.76 ppb in the filter-off condition and 28.5 ppb in the filter-on condition, which was not a statistically significant difference (Table 4). Bacterial richness, as determined using the Chao 1 index, was markedly lower in the filter-on condition than in the filter-off condition (Fig. 2). No significant difference in the diversity of bacterial extracellular vesicles between the filter-on and -off conditions was observed under principal component analysis (Fig. 3). The concentration of phthalate metabolites also showed no significant difference between the two (Table 5).
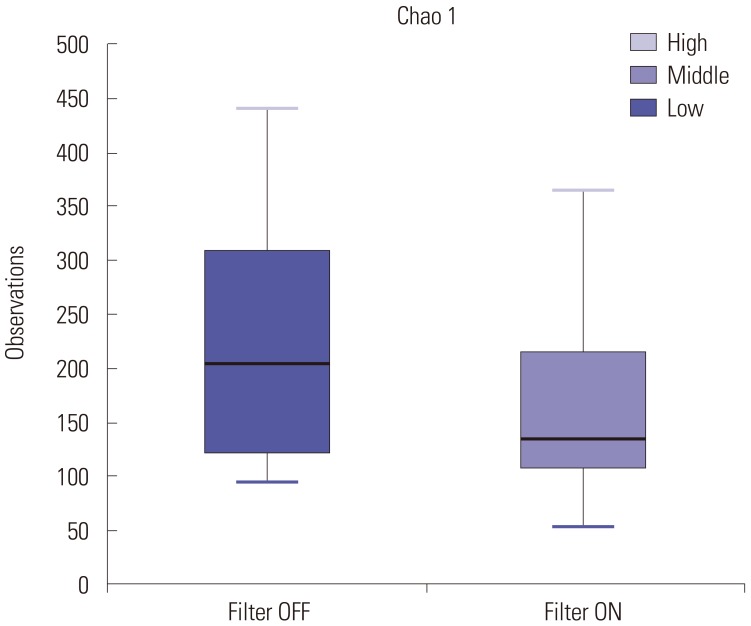
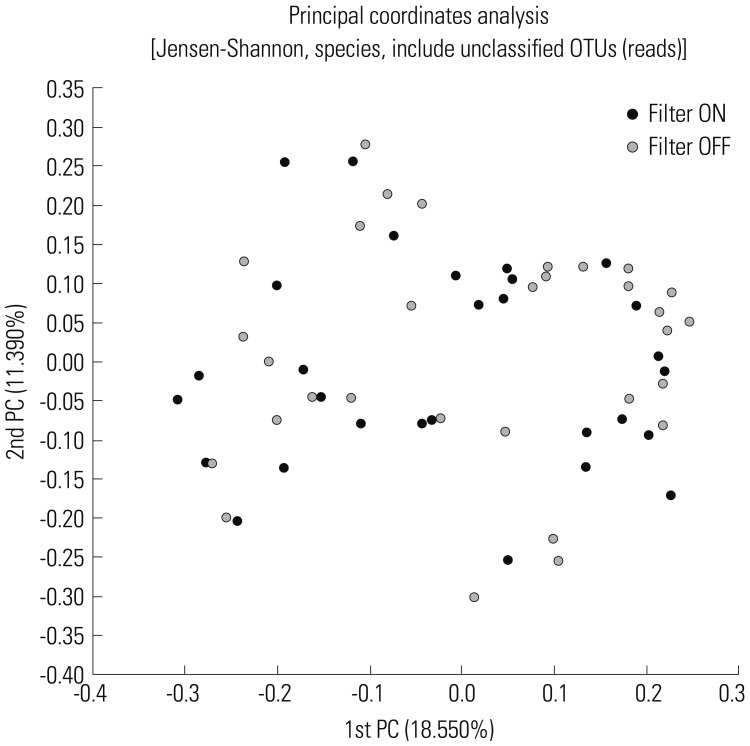
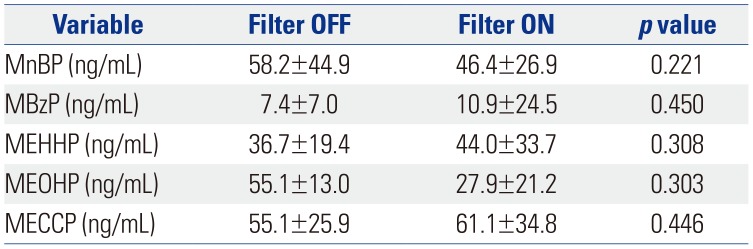
Fig. 2
Alpha-diversity as determined by the Chao 1 index (p=0.040). Alpha diversity summarize the structure of an ecological community with respect to its richness.
![]()
Fig. 3
Beta-diversity defined by principal component analysis. Beta diversity summarize the quantified differences in species composition between ecological community. OTU, operational taxonomic unit; PC, principal component.
![]()
Table 5
Concentration of Urine Phthalate with the Filter OFF or ON
![]()
DISCUSSION
PM2.5 is known to penetrate the vascular and lymphatic systems after inhalation and to be strongly associated with respiratory and allergic diseases.21 Moreover, a significant association between short-term PM exposure and asthma-related hospital visits has been demonstrated.22 Accordingly, reducing indoor exposure to PM2.5 may be beneficial to asthma management. The results of this study showed that the use of an air purifier for 3 weeks significantly decreased indoor PM2.5 levels, thereby reducing the frequency of medication use and urine microbiome burden in children with asthma.
As of now, the role of an air purifier in allergic disease prevention continues to be debated. While a number of studies have evaluated the impact of air purifiers on allergic disease, many are limited by small sample sizes and inadequate blinding.23 A study funded by Samsung Electronics Co., Ltd demonstrated that reducing indoor PM2.5 levels with air purifiers improved childhood asthma control test scores and mean evening peak flow rates.4 However, since the city where the study was conducted had a very low basal PM2.5 level of 7.42 µg/m3, and the concentration change due to the use of air purifiers was not significant, it is thought that the symptom relief will not be significant. It is also likely that the placebo effect was not excluded since crossover study was not performed with a small sample size of 9 people.
In the present study, we documented a significant reduction in indoor PM2.5 levels and improvement in medication scores. While the outdoor temperature and air pollutants might have differed during the cross-over period, the study was conducted under the same conditions during this period, and thus, the difference in outdoor atmospheric factors would not have affected the study outcomes. In addition, since the basal PM2.5 value was higher than that in the study mentioned above, the decrease in PM2.5 values after use of the air purifier is more meaningful. Moreover, the decrease in the frequency of medication used was significant since the placebo effect was excluded through the single blind and cross-over study design with a sample size of 30 people.
There is a hygiene hypothesis that suggests that decreased microbiome diversity is an environmental cause of increased asthma prevalence.6 Although the exact mechanism by which PM2.5 exposure perturbs airway microbiome is unknown, it has been found that individuals with better lung function have greater airway bacteria diversity in the bronchial tree.24 In support thereof, previous studies in patients with respiratory or allergic diseases have consistently shown reduced airway microbiome diversity and increased total richness.25 In our study, there was a significant decrease in urine microbiome richness in the filter-on condition, while there was no significant difference in urine bacterial diversity. Also, another study demonstrated that the number of airborne fungi decreases when an air purifier fan is on.26 These results suggest that air purifiers are beneficial to asthma patients by reducing total microbiome burden. Accordingly, we suggest that the urine microbiome burden is significantly reduced with the use of an air purifier to filter out and reduce the number and volume of bacteria in indoor air.
Recent research has proposed that phthalates, which are used as plasticizers, can affect bronchial epithelial cells to cause remodeling, resulting in asthma exacerbation,7 and significant correlations between concentrations of dust in indoor air and excreted phthalate metabolites in urine.27 We also observed higher phthalate concentrations in the asthma patient group than in a healthy control group (data not shown). This is consistent with the hypothesis of previous studies, in which phthalates exacerbate asthma by causing remodeling of the bronchial epithelium.28 However, in this study, urine phthalate metabolites did not differ between the individuals using the air purifier and those who were not, perhaps because of the route of phthalate exposure. Specifically, in prior research, the routes of phthalate exposure have included ingestion, inhalation, and direct dermal absorption.29 In the present study, DEHP and BBzP exposure mostly occurred by ingestion, while DnBP exposure occurred via inhalation and dermal absorption, suggesting that using an air purifier filter reduces phthalate exposure by inhalation, but does not affect exposure by ingestion or dermal absorption.
Our study also evaluated the role of PM2.5 in respiratory function and respiratory inflammation. It has been shown that urban air pollution is associated with PEFR decrements in children.30 As a well-known noninvasive biomarker for assessing airway inflammation, FeNO has been positively linked to exposure to PM2.5 in recent human studies.3132 In our study, no significant changes in asthma scores, PEFR, FeNO, or urine phthalate values were identified. Considering that a PM2.5 concentration exceeding the alarm standard set by the Ministry of Environment occurred only 3 days during the study period, it would be difficult to expect the air purifier would exert its maximum effect (Supplementary Fig. 1, only online).
In conclusion, we found that the indoor PM2.5 concentrations significantly decreased through the use of air purifier for 3 weeks, thereby reducing the frequency of medications used and significantly reducing the urine microbiome burden in children with asthma. We concluded that air purifiers can have a positive effect on the health of asthma patients by filtering fine dust and microbes from indoor air. This study can be used as basic data for further studies in the future, given that it is the first study in Korea on the effects of using air purifiers on children with asthma.
 XML Download
XML Download