

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neurologic disorders are among the most frequent and devastating complications of human immunodeficiency virus (HIV) infection. Frequently, neurologic disorders negatively impact patient's quality of life and their adherence to medical treatment leading to an increased chance of morbidity and mortality. These neurologic complications are either due to the primary pathogenic process of HIV infection or secondary to opportunistic infections.1
In 2007, the National Institute of Mental Health and National Institute of Neurological Diseases and Stroke, United States2 suggested the term HIV associated neurocognitive disorder (HAND), which encompasses the entire spectrum of neurological disorders associated with HIV-1 infection. This classification proposed for HIV-related central nervous systems (CNS) impairment was referred to as the Frascati criteria3 that included milder forms of neurocognitive disturbance: asymptomatic neurocognitive impairment (ANI) and minor neurocognitive disorder (MND) and HIV associated dementia (HAD). ANI includes cognitive impairment involving at least 2 cognitive domains (performance of at least 1 standard deviation [SD] below the mean for norms on neuropsychological tests) and the cognitive impairment does not interfere with everyday functioning. MND includes cognitive impairment involving at least 2 cognitive domains (performance of at least 1 SD below the mean for norms on neuropsychological tests) and the cognitive impairment that produces at least mild inference in daily functioning. HAD includes marked cognitive impairment involving at least 2 cognitive domains (performance of at least 2 SD below the mean for norms on neuropsychological tests) and the cognitive impairment produces marked interference with day to day functioning.
To adequately evaluate the extent of neurocognitive impairment, a battery of neuropsychological tests is typically administered.4 However, these neuropsychological tests are neither cost effective nor time efficient in the outpatient clinical setting as they often require several hours to complete and can be labor intensive requiring additional trained personnel to administer and correctly score.4 One strategy to overcome this problem is to administer a brief screening tool to identify those who would benefit from a full diagnostic evaluation.
Montreal Cognitive Assessment (MoCA)5 is a screening tool that taps both cortical and subcortical processes which can be completed in about 10 minutes. This screening tool assesses 8 cognitive domains (attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation), which are scored within a range of G-30 points (higher scores reflecting better cognitive function). Valcour et al.4 recommended MoCA in combination with screening for depression (e.g., BDS-II) for screening of HAND. Easy accessibility on the internet and availability in different languages make it more attractive as a screening tool.
Hasbun et al.5 reported that only a MoCA score <26 was associated with neurocognitive impairment and had good screening accuracy (sensitivity: 85%, specificity:40% with a negative predictive value 48% and positive predictive value 81%). The MoCA provides some coverage of executive function, motor skill, language fluency and verbal learning. Therefore, the addition of a neurological examination focused on motor speed, tone, reflexes and integration with clinical variables (e.g., CD4 nadir, viral load) may add to the specificity.
The Mind Exchange Working Group6 advocates that all patient living with human immunodeficiency virus (PLHIV) should be screened for HAND regardless of symptoms or risk factors by using sensitive screening tools. This group recommended that patients should be screened early in the disease and then every 6–24 months. The British HIV Association also suggested annual screening of PLHIV, but they do not give details of which methods should be used and targeted populations.7 Guidelines from the European AIDS Clinical Society recommended that formal neuropsychological tests should be restricted to patients who have symptoms of impaired cognitive function based on a questionnaire.8
Limited studies have been performed among PLHIV in India, mostly utilizing the earlier screening methods. There are no published reports on assessment of risk factors associated with HAND among Indian subjects. This study aims to evaluate the prevalence of HAND and assess the associated risk factors in HIV infected individuals (both pre-antiretroviral therapy [ART] and on ART).
Go to : 
METHODS
A descriptive cross-sectional study was conducted in the Department of Medicine at Chandra Laxmi Hospital, Vaishali, Ghaziabad. Sample size was estimated using an expected prevalence of 50% for HIV associated neurocognitive disorder (HAND) in PLHIV. Hence the study enrolled 160 PLHIV who met the criteria were enrolled age ≥18 years, willing to give informed consent. For pre-ART-subjects — HIV positive, ART naïve, on ART subjects — HIV positive on ART for at least 3 months duration. Exclusion criteria included Known history of confounding neurological disorders, history of ongoing opportunistic infections of brain Toxoplasmosis, cryptococcal meningitis, history of head injury/seizures/loss of consciousness (>30 minutes) in the past, history of known psychiatric illness and active substance abuse.
All of the patients enrolled in the study underwent detailed history and clinical examination. Anthropometric assessment, general physical examination and systemic examination were done to assess the baseline clinical status, any opportunistic infections and for World Health Organization (WHO) clinical staging. All patients were subjected to CD4 count evaluation. Neurocognitive assessment was done in all subjects by administering the MoCA scale.5 A score of less than 26 was considered abnormal. Assessment of functional ability was done in all subjects by using the Lawton and Brody Instrumental Activities of Daily Living Scale (IADL),9 which contains 8 domains: ability to use a telephone, shopping, food preparation, housekeeping, laundry, mode of transportation, responsibility for own medications and the ability to handle finances.
On the basis of MoCA and IADL scores, we classified HAND into: ANI-MoCA score <26 and no functional impairment, MND-MoCA score <26 and mild functional impairment, and HAD-MoCA score <26 and severe functional impairment.
An assessment for risk factors for HAND was done on: age, sex, education, employment, immunological status (CD4 count), WHO staging, body mass index, ART regimen, ART duration, duration of HIV infection.
As presence of depression was considered to be a possible determinant of HAND, depressive symptoms were measured by administering the Patient Health Questionnaire-910 on all participants. Any level of depression based on the questionnaire was considered significant.
All statistical analysis was performed by using SPSS software (version +21.0; SPSS Inc., Chicago, IL, USA). Chi-square test was used to find association between independent and dependent variable and p< 0.05 was considered statistically significant.
Go to :
RESULTS
One hundred sixty patients were enrolled in our study, 80 were on some form of ART while other 80 were ART naïve. Table 1 describes the demographic profile of our patients.
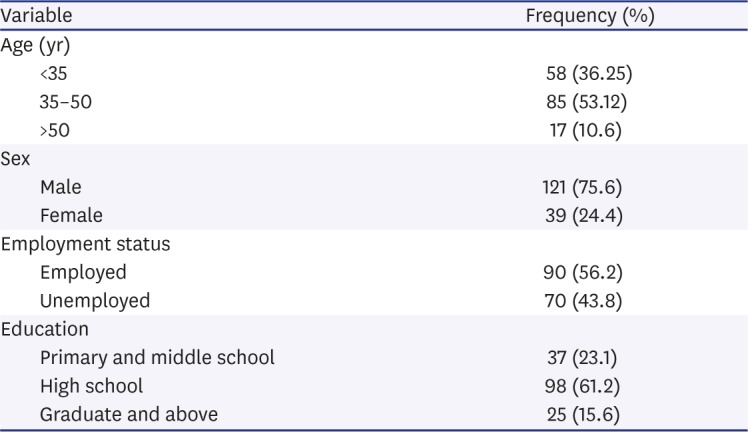
Table 1
Demographic profile of our population (n=160)
![]()
Out of 80 the subjects on ART, most (77.5%) were on first line ART regimen, while only 22.5% were on second line ART regimen. Twenty-six subjects (32.5%) were on tenofovir+lamivudine+efavirenz, 6 (7.5%) on zidovudine+lamivudine+efavirenz, and 30 (18.8%) on zidovudine+lamivudine+nevirapine regimen. The second line regimen was tenofovir+lamivudine+ritonavir boosted atazanavir. The mean duration of ART among the ART group was 4.1±3.3 years (range −10 months to 15.6 years).
Out of 160 patients, 84 (52.5%) had HAND. Majority of them 76 (47.5%) had the mildest form of HAND, i.e., ANI. Five percent (n=8) fell into the MND category. No patient was found to have HAD.
Out of the 160 subjects, 96.3% (n=77) of pre-ART and 93.75% (n=75) of ART subjects reported normal daily living activities (ADL). Overall, only 5% of patients were found to have mild impairment in ADL and no patient had severe impairment in daily activities. The most common affected domain was food preparation (n=4 and 50%); while impairment in transportation, self-medication impairment and handling finance were other domains affected. The subjects who reported impairment in food preparation were all male (n=4).
In order to determine the risk factors for HAND in our study population, p-value was calculated as shown in Table 2. It was found that age >40 and lower education could be attributed to increased chances of HAND.
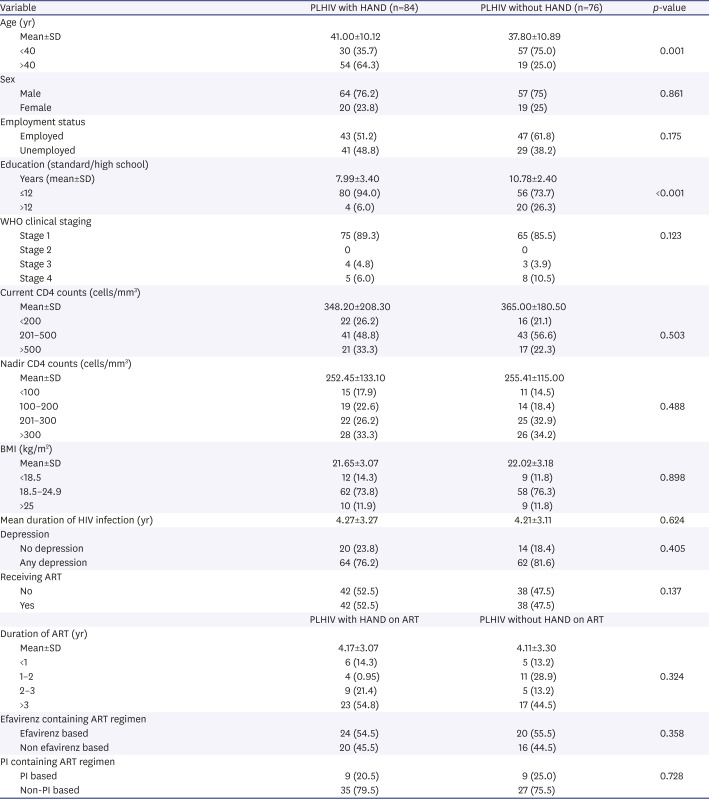
Table 2
Determinants of HAND in PLHIV
Values are presented as number (%).
HAND: human immunodeficiency virus associated neurocognitive disorder, PLHIV: patient living with human immunodeficiency virus, SD: standard deviation, WHO: World Health Organization, BMI: body mass index, HIV: human immunodeficiency virus, ART: antiretroviral therapy, PI: protease inhibitor.
![]()
Go to :
DISCUSSION
Our study showed that the overall prevalence of HAND was 52.5% in our study population. The reported prevalence of HAND among PLHIV in literature is variable ranging from 5.9% to 90.1% in different studies.11121314151617181920
This wide variation in the reported prevalence of HAND is due to multiple reasons such as intrinsic differences in the population studied due to differences in ethnicity, race and composition of population and other factors such as duration of HIV infection, ART. Another crucial point of difference is the tool or instrument used to detect and diagnose HAND.
In the Charter study the prevalence of HAND was 52% as assessed by detailed neurocognitive test battery.11 Yakasai et al.21 also explored the prevalence of HAND in Nigeria by using a MDNPT battery combined with measures of functional status by using PAOFI and Karnofsky performance scale and reported HAND prevalence of 40% in ART naive and 30% in on ART subjects.
In India, the prevalence of HAND was determined to be 33.65% by using Mini-Mental State Exam and 32.5% by using International HIV Dementia Scale.1315 There are no published reports of HAND prevalence using the MoCA instrument from India.
Among PLHIV with HAND in our study, the prevalence of ANI was 47.5%, and of MND was 5%. HAD was not demonstrated among our study population. Though the overall prevalence of HAND is high, there has been a global trend towards a decreasing prevalence of the more severe form of HAND like HAD while the milder forms and asymptomatic neurocognitive dysfunction is on the rise.
The ART probably benefits the brain via multiple mechanisms, including immune recovery, reduced immune activation, and viral suppression- both systemically and in the CNS. This may explain a mitigation in the severity of HAND. However, persistent high prevalence of neurocognitive dysfunction among PLHIV in the ART era could be due to early invasion of CNS by the virus soon after infection, which later on leads to long term complication of HAND. Our findings are consistent with existing literature in this regard. Heaton et al.11 noticed that the prevalence of HAD declined from 20% to 7% in the ART era. In the Charter study, out of 52% of PLHIV with HAND, 32.7% had ANI, 11.7% had MND and only 2.4% had HAD.
Just like our study, Grant et al.22, McCutchan et al.23, Cross et al.24 in US, Troncoso et al.25 in Brazil and Choi et al.26 in Africa also reported that older age (>40 years) was significantly associated with HAND. In Asian studies, Chan et al.27 in Singapore, Ku et al.28 in south Korea, Wang et al.29 in China and Achappa et al.17 in India also demonstrated a similar finding.
Education is considered to be a proxy for cognitive reserve. It was found that educational qualification below graduate level was significantly associated with HAND, consistent with our data, Cross et al.24 in the US and Troncoso et al.25 in Brazil also observed the association of HAND with lower years of education.
Unlike the previous study in South Asian population, the prevalence of HAND was not associated with the severity of HIV infection.27 This suggests that milder disease of HIV infection, i.e., lesser immune suppression does not appear to be protected from the development of HAND. This also supports the view that HIV penetrates the brain early in the infection and stays there leading to long term sequelae like HAND.
It is possible our CD4 counts were not truly reflective of the lowest CD4 counts of the patients. Since our study was a cross sectional in design, possibly a onetime assessment of CD4 counts and its association with HAND was inconclusive. A study in Nigeria by Yakasai et al.21 also reported a similar result in which HAND was found in 40% of the pre-ART group and 30% of the ART group. This finding signified that HAND is common in the present ART era and also implied that ART does not apparently prevent the development nor successfully treat HAND among PLHIV. However, this finding does not mean that ART is not an effective treatment for HAND as half of the study subjects were already on ART.
In the pre-ART era, a progressive subcortical dementia with motor and cognitive slowing was prominent among PLHIV with HAND. This was reflected by an abnormal score of MoCA in visuospatial function, memory, abstraction (reasoning) and concentration (attention) domains. However, in the ART era and in more advanced stages of HAND, cortical involvement is more frequently observed. Clinical features like aphasia, agnosia and apraxia are more typical of cortical involvement.30 Involvement of cortical structures is suggested by impairment in orientation, naming, language and calculation domains of a screening tool.
In our study also, both cortical and sub cortical regions were observed to be affected in HAND. Further analysis on abnormal scores in MoCA cognitive domains showed that among PLHIV with HAND, 88% developed abnormality in >3 domains as shown in Table 3. It is interesting to observe that in spite of being diagnosed as cognitively normal (on total MoCA score), 31.6% and 52.7% of PLHIV without HAND developed abnormality in 2 and 3 domains respectively. Therefore, our study results suggest that an assumption of having abnormality in >3 cognitive domains must be considered among PLHIV with HAND.

Table 3
The frequency of abnormal score in cognitive domain among the study population
| Abnormal scores in | PLHIV with HAND (n=84) | PLHIV without HAND (n=76) |
|---|---|---|
| 1 domain | 0 | 10 (13.2) |
| 2 domains | 0 | 24 (31.6) |
| 3 domains | 12 (14.3) | 40 (52.7) |
| 4 domains | 41 (48.8) | 2 (2.6) |
| ≥5 domains | 33 (39.2) | 0 |
Values are presented as number (%).
HAND: human immunodeficiency virus associated neurocognitive disorder, PLHIV: patient living with human immunodeficiency virus.
![]()
It was shown that subjects with HAND performed poorly in all the domains on neurocognitive assessment with MoCA compared to those without HAND except for the domain of orientation (Table 4). A univariate logistic regression analysis was performed for all domains of MoCA. It showed that memory (odds ratio [OR], 35.500; p<0.001), visuospatial function (OR, 22.28; p<0.001), language (OR, 9.258; p=0.001), calculation (OR, 7.808; p<0.001), naming (OR, 4.419; p= 0.001) and abstraction (OR, 4.440; p=0.044) were significantly associated with the presence of HAND. This implied that impairment in memory and visuospatial functions on the MoCA had the most predictive power for the presence of HAND.
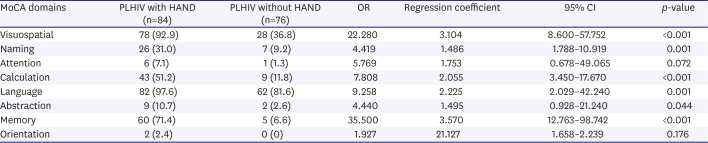
Table 4
Frequency of abnormal scores and logistic regression results showing predictive power of individual cognitive domains on MoCA testing for HAND
Values are presented as number (%).
MoCA: Montreal Cognitive Assessment, HAND: HIV associated neurocognitive disorder, PLHIV: patient living with human immunodeficiency virus, OR: odds ratio, CI: confidence interval.
![]()
Depression is considered to be a potential confounder for the presence of HAND among PLHIV. In our study, no association between HAND and depression was found. Our study findings are similar to the findings of Chan et al.27, who also did not find a significant association between HAND and depression.
Even a milder form of HAND could still hamper the quality of life of HIV infected patients. Since our study design is a onetime observational study, we cannot comment upon the impact of HAND on treatment adherence, morbidity, progression of existing cognitive dysfunction and mortality among PLHIV with HAND.
The present study had several limitations. As majority of the study subjects were enrolled from the outpatient setting, there was a chance of missing a patient with severe cognitive impairment and severe impairment in ADL. Another limitation is exclusion of subjects with substance abuse and CNS opportunistic infections which were found associated with HAND. Some of the risk factors observed in other studies like serum viral load and CSF viral load were not performed in this study due to non-availability of the test in our setup.
Go to :
 XML Download
XML Download