

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of hypertension is increasing in various regions worldwide.1) High blood pressure (BP) increases the risk of cardiovascular disease (CVD), renal disease, BP-related disability and even death. Therefore, hypertension is an enormous burden not only on patients, but also on society as a whole.2)3) Fortunately, adequate treatment for hypertension can delay its downstream side effects and improve prognosis.4)5)
The optimal BP can be achieved using BP-lowering medications and/or lifestyle modifications, such as a healthy diet, sufficient physical activity, and avoiding tobacco use.6)7)8) Healthy lifestyles have advantages beyond that of BP reduction. In contrast, following an unhealthy diet can nullify the BP-lowering effects of powerful medications.9) Therefore, patients with hypertension are strongly recommended to combine dietary modifications with BP-lowering medications to optimize their treatment.6)10)
Successful dietary modifications depend on patients' sustained self-management, as is true in other chronic illnesses that require lifelong attention.11) Dietary non-adherence in hypertension can disturb BP control, and even decrease a patient's quality of life and increase the cost of their medical care.12) In order to improve the level of dietary adherence to the guidelines in hypertension, there is a need for studies that evaluate diet management and dietary adherence to the guidelines in adults with hypertension are necessary.13) We investigated how many patients with hypertension manage their diet, and how well these patients follow the dietary guidelines.
METHODS
Study populations
We used data from the Korea National Health and Nutrition Examination Survey (KNHANES). KNHANES involves a health interview, health examination, and nutrition survey.14) Among all adults aged from 30 to 79 (n=20,419) in the KNHANES 2013–2016 data, those who did not participate in the nutrition survey or the health interview survey (n=4,325) and those who were pregnant or breast-feeding (n=224) were excluded. Finally, 15,870 adults (4,162 with and 11,708 without physician-diagnosis of hypertension) were analyzed for this study.
Definition of diet management, dietary intake and diet quality
During the nutrition survey, each participant was asked whether or not they manage their diet for any special reason. Based on the answers, we classified participants into the diet-managing group and not-managing group.
Dietary food and nutrient intakes were assessed by a 24-hour dietary recall. Comprehensive diet quality was evaluated with Korean Healthy Eating Index (KHEI), which was developed to assess overall diet quality in Korean adults based on the 2010 Dietary Guidelines for Koreans.15) The KHEI consists of 8 components that one should consume often (breakfast, mixed grains, fruits, vegetables, meat/fish/eggs and beans, and milk and milk product); 3 components for which moderate consumption is recommended (saturated fatty acids, sodium, and sweets and beverages); and other 3 components for which balanced consumption is recommended (carbohydrates, total fat, and energy). The total score ranges from 0 to 100 and higher score means further healthier diet. Supplementary Table 1 shows components of and scoring standards for KHEI.
Other variables
Information regarding disease-related characteristics and lifestyle behaviors were also included in this study. The duration of hypertension was calculated based on the age at the time of (a physician's) diagnosis, and the patient's current age. Antihypertensive drug treatment was defined as taking an antihypertensive drug for more than 20 days per month. Comorbid status was defined based on patients' self-report of a previous diagnosis of stroke, myocardial infarction, angina pectoris, diabetes, dyslipidemia, etc. before the survey. Family history of hypertension was also based on self-report of any family member (father, mother, and siblings) with a diagnosis of hypertension. Body mass index (BMI) was calculated using the height and weight measured during the health examination survey. Obesity was defined by a BMI of >25.0 kg/m2. The following health-related lifestyle factors were also surveyed: smoking (yes: current smoking, no: non- or past smoking); alcohol intake (yes: drinking ≥1 unit per month during the previous year, no: non-drinking or drinking <1 unit per month); and walking or other physical activity (yes: ≥5 days per week and ≥30 minutes per day, no: non-walking or less than 5 days per week or <30 minutes per day).
Ethical aspects
The KNHANES protocols were approved by the Institutional Review Board (IRB) of Korea Centers for Disease Control and Prevention (KCDC; IRB No. 2013-07CON-03-4C, 2013-12-EXP-03-5C). Written informed consent was provided by all participants. All of the study procedures were in accordance with the ethical standards of the responsible Institutional Committee on human experimentation, and were in accordance with the Helsinki Declaration (of 1975 as revised in 2008).
Statistical analysis
Demographic and disease-related data were presented as mean±standard deviation or as frequencies (%). The differences of means and proportions between groups were evaluated using t-tests and χ2 tests. The dietary intakes and KHEI scores were adjusted for sex and age, and were presented as mean±standard error of mean. The differences of the adjusted means between the groups were tested using analysis of covariance. All analyses were performed using the statistical software package SAS (version 9.4; SAS institute, Cary, NC, USA). The p values<0.05 were considered statistically significant.
RESULTS
Characteristics of adults by self-reported dietary management
The proportion of diet-managing people was 22.6% (2,647 over 11,708) in those without hypertension and 28.0% (1,167 over 4,162) in those with hypertension (Table 1). In both adults with and without hypertension, diet management was more prevalent in women. Diet-managing adults were younger, had a higher income, longer duration of hypertension, more comorbid diseases and more frequent family history of hypertension than did those in the non-management group. Healthier lifestyle behaviors such as nonsmoking and nondrinking were prevalent in adults with hypertension than those without hypertension. But the prevalence of regular walking did not differ by the presence of hypertension. Regardless of the presence of hypertension, diet-managing adults tended to have healthier behaviors, such as smoking less, drinking less, and walking more than non-managing group. However, there was no difference in diet management by antihypertensive drug treatment among adults with hypertension.
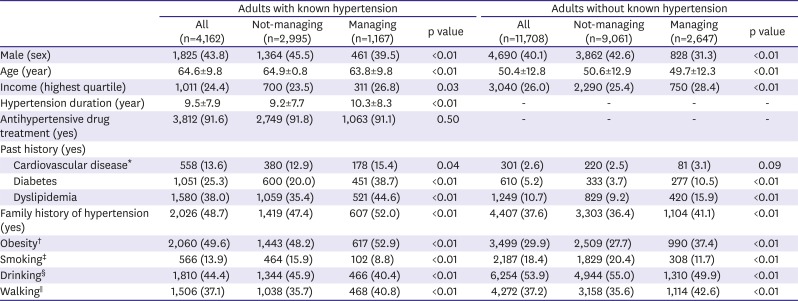
Table 1
Demographic and disease-related characteristics by self-reported dietary management
Values are presented as mean±standard deviation or number (%).
*Stroke, myocardial infarction, angina pectoris; †≥ 25.0 kg/m2; ‡Current smoking; §Drinking ≥1 unit per month during the previous year; ‖Walking ≥5 days/week and ≥30 minutes/day.
![]()
Dietary intake according to diet management
Compared to adults without hypertension, those with hypertension consumed less energy and dietary sodium and more vitamins (Table 2). However, there was no difference of sodium-to-potassium ratio between the groups, because potassium intake was also low in those with hypertension. Irrespective of the presence of hypertension, diet-managing adults had better diet than not-managing adults. Diet-managing adults consumed less energy and had more appropriate macronutrient proportions than did not-managing adults. They also significantly consumed less sodium and thus lower sodium-to-potassium ratio than non-diet-managing adults. In addition, diet-managing group consumed more calcium and vitamins than non-diet-managing group. However, despite diet management, mean dietary sodium intake of diet-managing adults with hypertension (3,354.5 mg) was still higher than the recommended guideline (≤2,400mg/day recommended by Korean Society of Hypertension [KSH]).16) The proportion of adults who consumed less than 2,400 mg of sodium was merely 28.8% in those with hypertension (data not shown).
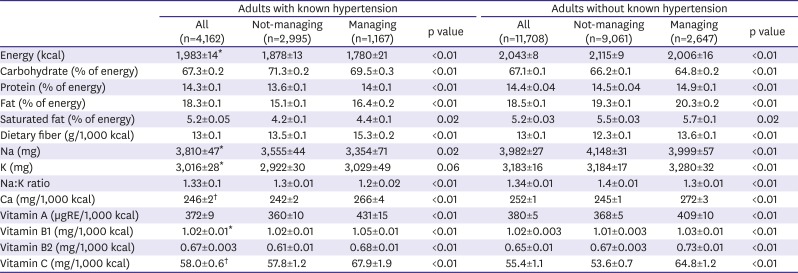
Table 2
Dietary intakes by self-reported dietary management
Values are presented as sex-, age-adjusted mean±standard error of mean.
*p value<0.01 for difference of adjusted mean dietary intakes between adult with and without known hypertension; †p value<0.05 for difference of adjusted mean dietary intakes between adult with and without known hypertension.
![]()
Dietary quality according to diet management
Table 3 shows total score of and each component score of KHEI. Diet-managing adults had higher scores for total KHEI and each component of KEHI than non-diet-managing adults, regardless of the presence of hypertension. However, total KHEI score was rather lower in adults with hypertension (62.9 score) than in adults without hypertension (63.4 score, p value<0.01), mainly because of the differences in consumption of fruit, vegetable, and dairy products. Supplementary Figure 1 shows additionally the distribution of adults who satisfied the reference of each component, and those who did not. On the whole, there was little difference in distribution between adults with hypertension and without. Of those with hypertension, more than half had lower intake of whole grain, fruits, vegetables, food rich in protein (including meat, fish, eggs, legumes), and dairy products, and had higher sodium consumption than the recommended level. Meals of hypertensive adults can be characterized as low in fat and high in carbohydrates.
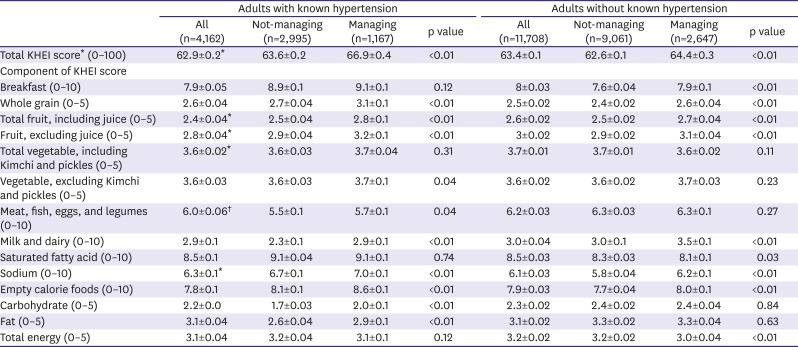
Table 3
KHEI by self-reported dietary management
Values are presented as sex-, age-adjusted mean±standard error of mean.
KHEI = Korean Healthy Eating Index.
*p value<0.01 for difference of adjusted mean dietary intakes between adult with and without known hypertension; †p value<0.05 for difference of adjusted mean dietary intakes between adult with and without known hypertension.
![]()
DISCUSSION
To the best of our knowledge, this is the first study to investigate how many hypertensive patients manage their diet in the real-world setting, and how well they satisfy the guidelines recommended by health professionals. The KSH recommends less than 6 g of daily salt consumption (equivalent to ≤2,400 mg of sodium), and balanced healthy diet which is characterized as high intake of fruits, vegetables, dietary fiber, vitamins, and minerals, and low fat intake.16) We found that only one-third of adults with hypertension were managing their diet. Although those who were managing their diet consumed less sodium and had a much healthier diet than did those who were not managing their diet, only a small fraction of actual diets satisfied the dietary guidelines for the management of hypertension. In addition, mean sodium intake of adults with hypertension was still over the recommended level.
In Korea, excessive sodium intake and the high prevalence of hypertension are major public health issues.17)18) Therefore, the Korean government has made a great effort to reduce sodium intake and its socioeconomic burden. The Ministry of Food and Drug Safety has implemented a sodium reduction policy and regulations for lower sodium consumption.17) The KCDC published a hypertension counseling manual and guidelines for use in various settings, including health care centers.19)20) The government has also allowed medical institutions to hire professionals (including doctors, nurses, and nutritionists) who are dedicated to patient education and counseling for hypertension management. These institutions receive expenses as non-payment items in order to increase patients' understanding of hypertension and to enhance BP management. Despite all of these efforts, however, our study revealed that many Korean adults with hypertension do not manage their diet in daily life, and do not have diets that meet the diet recommendations. Such poor diet management and low dietary adherence is not a unique problem to our study population. A study of Pakistani hypertensive patients investigated dietary adherence to recommendations using a self-report questionnaire.21) Among all patients (n=400), merely 22.5% reported that they followed the recommended diet that is low in fat and sodium intake. Another study of Finnish adults with hypertension (n=138) investigated dietary and lifestyle compliance and antihypertensive medications and follow-up visits using 27 survey questions.22) Patients had the best compliance with their medications (75%), followed by physical activity (54%) and alcohol intake (53%). The level of dietary compliance was lowest. Only 30% of the patients were compliant with recommendations for sodium, fat, and vegetables. Poor dietary compliance in patients with hypertension has been consistently mentioned as a barrier for adopting dietary changes even in intervention studies.13)21)
We suspect that patients may have poor dietary compliance because they cannot appreciate the immediate effects of dietary changes on their BP, and therefore they do not recognize its importance.23) Previous studies have also found that hypertensive patients on antihypertensive medications tend to smoke and drink more than those who are not treated with medications.24) Patients may feel that their antihypertensive medications overpower the harmful impact of an unhealthy lifestyle on BP management. However, an unhealthy lifestyle can actually nullify the BP-lowering effects of powerful medications.9) An optimal diet that is rich in fruits and vegetables and low in sodium, for instance, can reduce the need for medications, reduce drug costs, and even improve one's CVD risk factors.7)9)12) Therefore, more attention should be given to dietary management in hypertensive patients. Further studies which investigate patient's perception, willingness, and efficacy to dietary modification to control BP and which factors are associated with adopting dietary change are needed.21)25)
Our study has several strengths. First, we discriminated between diet management behavior and dietary adherence to recommendation. Previous studies have only evaluated dietary adherence using questionnaires that focused on diet management behaviors, such as reduction in fat or sodium reduction.13)21)22)25) Using only self-reported data on dietary modification makes it difficult to understand the gap between the individual’s subjective judgement on taking action (e.g., changing eating habits or cutting down salt intake) to control BP and actual food and nutrients consumption.25) However, we investigated whether or not they manage their diet and evaluated their actual dietary intakes to the recommendations for hypertension. This allowed us to find how many patients were managing their diet, and how well they were following dietary recommendations. We also found that most of the actual diets of those who responded that they were managing their diet did not meet the recommended guidelines. Another strength is that we used data from the KNHANES, which is a nationally representative cross-sectional survey. Thus, our study included Korean hypertensive adults with diverse socioeconomic backgrounds. There were several limitations to be considered. We used dietary intake assessed by a 1-day 24-hour diet recall. As well-known, single-day dietary assessment does not necessarily reflect one's usual intake due to day-to-day variation in dietary consumption.26) In order to overcome the influence of measurement error, we also analyzed only for adults who reported that their 24 hours recall day was typical for them, which the results remained unchanged (Supplementary Tables 2 and 3).
In conclusion, a large proportion of hypertensive patients do not manage their diets. Even those patients who do manage their diets did not satisfy the recommended guidelines for the dietary management of hypertension.
 XML Download
XML Download