

 PDF
PDF ePub
ePub Citation
Citation Print
Print



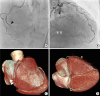
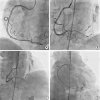
A 65-year-old female with stable angina presented with chronic total occlusion (CTO) of the distal right coronary artery (RCA) (Figure 1 and Supplementary Video 1). Coronary intervention of the distal RCA-CTO was performed via the antegrade approach. After successful crossing the CTO lesion gently with a soft guide wire (NEO's Sion black; Asahi, Aichi, Japan), the leakage of contrast media through multiple tiny channels at the posterior descending coronary artery was noted (Figure 2 and Supplementary Video 2). It was initially misinterpreted as coronary perforation, leading to prolonged ballooning of the leakage site without changes in leakage appearance. She was stable without evidence of pericardial effusion by echocardiography, indicating coronary arteriovenous fistulas. The RCA lesions were treated with two drug-eluting stents (Orsiro 2.5×40 mm; Biotronic, Bulach, Switzerland). Final angiogram showed arteriovenous fistulas between RCA and coronary sinus, which mimicked coronary perforation (Figure 3 and Supplementary Video 3).
Coronary artery fistulas can occur from any of the three major coronary arteries, and coronary artery dilatation is common because the fistulas drain into the low-pressure structures. However, when the fistulous communication arises in the distal part of a coronary artery, the artery diameter may remain small.1) In our case, the fistulas before CTO intervention were not recognized probably due to the insufficient driving pressure of collateral flow across tiny fistulas, but seen after restoration of brisk antegrade flow. We report an interesting image of arteriovenous fistulas with multiple tiny channels that can be mistaken for coronary artery perforation after CTO recanalization.


 XML Download
XML Download