

 PDF
PDF ePub
ePub Citation
Citation Print
Print


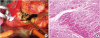
A 46-year-old male underwent mitral valve (MV) repair because of anteriorly directed severe eccentric mitral regurgitation (MR) from posterior leaflet fail (Figure 1A, Supplementary Videos 1, 2, 3). Five months later, he was readmitted complaining recurrent syncope caused by newly discovered dynamic left ventricular outflow tract (LVOT) obstruction (Figure 1B). His echo also showed systolic anterior motion of the chordae tendineae and this time, posteriorly directed MR was observed (Figure 1B, Supplementary Videos 4, 5, 6) which were not observed before the surgery. Hypertrophied septum, presence of elongated MV and abnormal insertion of the secondary chordae were indicative of hypertrophic cardiomyopathy (HCM) (Supplementary Video 7). His HCM was not diagnosed at the time of surgery and his current dynamic LVOT obstruction was absent back then, by chronic left ventricular (LV) remodeling due to the coexistence of chronic severe MR, which was unmasked after LV cavity decreased after successful MV repair (preoperative LV end-diastolic dimension (EDD)/end-systolic dimension (ESD): 56/32 mm, postoperative LV EDD/ESD: 43/26 mm). Despite optimal medication, he had to underwent endocardial muscle resection (3 cm depth, 0.5–0.8 cm thickness, a total of 3 grams) and resection of the abnormal chordae attached at the A2 portion of the anterior mitral leaflet (Figure 2A). The histopathology of the resected myocardium revealed hypertrophy and disarray of the myocytes with interstitial fibrosis (Figure 2B). The patient recovered well, with significant relief of the dynamic LVOT obstruction (Figure 1C, Supplementary Videos 8, 9, 10). MV prolapse occasionally presents in association with myocardial disease. Although incidence of coexisting MV prolapse with HCM is not frequent, when associated with unusual LV hypertrophy, one need to vigilantly search for possible associated cardiomyopathy. Assessment of the myocardial abnormalities is as important as assessment of the MV structure, given the possibility of the combined presence of HCM and MV prolapse.1)2)
Darae Kim, MD, PhD1 , Chi Young Shim, MD, PhD2, Geu-Ru Hong, MD, PhD2, Byung-Chul Chang, MD, PhD3
, Chi Young Shim, MD, PhD2, Geu-Ru Hong, MD, PhD2, Byung-Chul Chang, MD, PhD3
, Chi Young Shim, MD, PhD2, Geu-Ru Hong, MD, PhD2, Byung-Chul Chang, MD, PhD3
Figures and Tables

References
1. Maron MS, Olivotto I, Harrigan C, et al. Mitral valve abnormalities identified by cardiovascular magnetic resonance represent a primary phenotypic expression of hypertrophic cardiomyopathy. Circulation. 2011; 124:40–47.

2. Petrone RK, Klues HG, Panza JA, Peterson EE, Maron BJ. Coexistence of mitral valve prolapse in a consecutive group of 528 patients with hypertrophic cardiomyopathy assessed with echocardiography. J Am Coll Cardiol. 1992; 20:55–61.
SUPPLEMENTARY MATERIALS
Supplementary Video 3
Flail of posterior mitral leaflet is observed with elongated mitral valve leaflets and abnormal insertion of secondary chordae to anterior mitral leaflet.
Supplementary Video 4
LV dimensions were normalized (LV end-diastolic dimension/end-systolic dimension: 43/26 mm) as a course of LV reverse remodeling. Systolic anterior motion of the chordae tendineae with asymmetric hypertrophy of septum was noted.
Supplementary Video 6
Systolic anterior motion of the chordae tendineae with dynamic LVOT obstruction was observed.
Supplementary Video 7
Cardiac magnetic resonance imaging also showed asymmetric septal hypertrophy (19 mm), systolic anterior motion of abnormally inserted chordae, and patchy late gadolinium enhancement in the hypertrophied myocardium, compatible with obstructive hypertrophic cardiomyopathy.
 XML Download
XML Download