

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Different types of sagittal skeletal malocclusions are categorized according to the relative anteroposterior positions of the maxilla and mandible.1 The dental arch is naturally adjusted to maintain functional occlusion, and tooth inclinations are generally compensated to overcome the skeletal discrepancy.2 This is also an important aspect to consider in orthodontic treatment of adults because dental alignment is corrected within the limits of skeletal disharmony. In other words, although a subject may seem to have good occlusion without apparent crossbite, the posterior teeth may be inclined and occlusal force may not be directed along the long axis of the teeth.
Cone beam computed tomography (CBCT) images can be used for evaluations of tooth inclinations on a consistent reference plane, and unlike dental casts or traditional two-dimensional (2D) radiographs, CBCT images are not prone to misjudgment caused by over-lapping structures. In assessing masticatory function, several studies have measured occlusal force and contact area, which serve as clinical records for evaluating the functional relationship of occlusion.345 One of the widely used methods is the Dental Prescale System, which can be simply applied in clinics by using a thin pressure-sensitive film.6 Previous studies have reported that this method yields objective results for occlusal force and contact area and is reliable when measuring the bite force at maximal clenching.47
The relationship between vertical facial patterns and occlusal force has been investigated, and the results have shown that long-faced adults have less occlusal force during maximum effort.8 However, limited information is available on occlusal force in subjects with different sagittal facial patterns. Three-dimensional (3D) investigations on posterior tooth inclinations as well as evaluations of occlusal function in subjects with different sagittal skeletal malocclusions would be meaningful for clinicians when delivering a sound treatment plan. Therefore, the objective of this study was to assess and compare the premolar and molar inclinations, occlusal force, and contact area in normodivergent adults with skeletal Class I, II, and III malocclusions for clinical significance in functional occlusion.
MATERIALS AND METHODS
A total of 124 subjects (61 males and 63 females) were enrolled in this study from January 2010 to March 2018. All subjects had CBCT scans (Pax-Zenith 3D; Vatech, Hwaseong, Korea) taken for diagnosing impacted third molars and masticatory function evaluated using the Dental Prescale System (Fuji Film Corp., Tokyo, Japan). The CBCT images were acquired in intercuspal occlusion with a scan time of 24 seconds, tube voltage of 105 kVp, and voxel size of 0.3 mm. The subjects were 17 to 40 years old, and the inclusion criteria were as follows: normodivergent facial pattern; dental crowding of less than 5 mm; no missing teeth excluding impacted third molars; no history of prosthetic treatment including onlays, crowns, bridges, or implants; no anterior or posterior crossbites or prior orthodontic treatment; and no temporomandibular joint disorders. Subjects were excluded if they had gingival recession causing a discrepancy between the cementoenamel junction and the alveolar crest level in the first molars. The normodivergent facial pattern was defined by an SN-MP (angle between Sella-Nasion to mandibular plane) angle between 28° and 38°, which represents about 1 standard deviation of normodivergent adults reported by Riedel,9 and was based on the findings of a previous study.2 This study was limited to subjects with normodivergent facial patterns in order to minimize factors related to vertical skeletal dimensions, as shown by the results of a prior study. A preliminary study was conducted on 144 adults with Class I malocclusions (72 males and 72 females) with hypodivergent (SN-MP < 27°), normodivergent (28° < SN-MP < 38°), and hyperdivergent (SN-MP > 39°) facial profiles, and the results showed that the mean occlusal force and contact area were significantly lower in the hyperdivergent group (Tables 1 and 2).

Table 1
Comparison of occlusal force and occlusal contact area in male subjects with Class I malocclusions according to vertical facial patterns
![]()

Transverse skeletal parameters and posterior tooth inclinations were measured using the coronal cross sections of the CBCT images by using the On-Demand 3D imaging software (CyberMed, Seoul, Korea). The following reference planes were used to ensure consistent orientation of the 2D coronal slices, based on the reference planes used in a previous study.2 (1) The axial plane was the plane passing through the bilateral orbitales and right porion, defined as the Frankfort horizontal (FH) plane. (2) The coronal planes were perpendicular to the axial plane and were set as follows for each posterior tooth. For the maxillary and mandibular first premolars, the coronal plane passed through the buccal cusp tips of the right maxillary and mandibular first premolars, respectively. For the maxillary and mandibular second premolars, the coronal plane passed the buccal cusp tips of the right maxillary and mandibular second premolars, respectively. For the maxillary first molars, the coronal plane passed through the buccal groove of the right maxillary first molar. For the mandibular first molars, the coronal plane passed the mesiobuccal groove of the right mandibular first molar. For the maxillary and mandibular second molars, the coronal plane passed through the buccal groove of the right maxillary and mandibular second molars, respectively. (3) The sagittal plane was perpendicular to the axial and coronal planes passing the midpoint of the medial rims of the orbits. On the coronal plane passing the buccal groove of the maxillary right first molar, the buccal maxillary and mandibular widths as well as alveolar widths were measured at the midroot level, which was set at 7 mm apical from the alveolar crest.2 Premolar and molar inclinations were evaluated on each specific coronal plane mentioned above. The FH plane was used as a reference to measure the inclination of the maxillary premolars and molars, and the lower border of the mandible was used to measure the inclinations of the mandibular premolars and molars.10 Additional premolar and molar inclinations were measured using the occlusal plane, which was defined as a line connecting the central sulci of the contralateral premolars or molars (Supplementary Table 1). Measurements used in this study are shown in Figure 1.
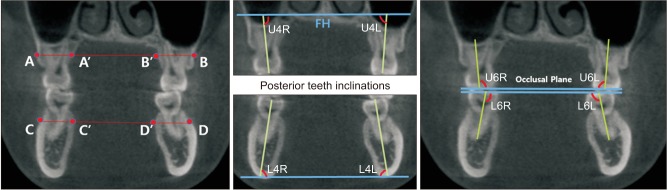
Figure 1
Transverse width and posterior inclination measurements.
A–B distance: buccal maxillary width at the midroot level. C–D distance: buccal mandibular width at the midroot level. Maxillary alveolar width: difference between A–B and A′–B′ width divided by 2. Mandibular alveolar width: difference between C–D and C′–D′ width divided by 2. Angle U4R and angle U6R: maxillary right premolar/molar inclination. Angle U4L and angle U6L: maxillary left premolar/molar inclination. Angle L4R and angle L6R: mandibular right premolar/molar inclination. Angle L4L and angle L6L: mandibular left premolar/molar inclination.
FH, Frankfort horizontal.
![]()
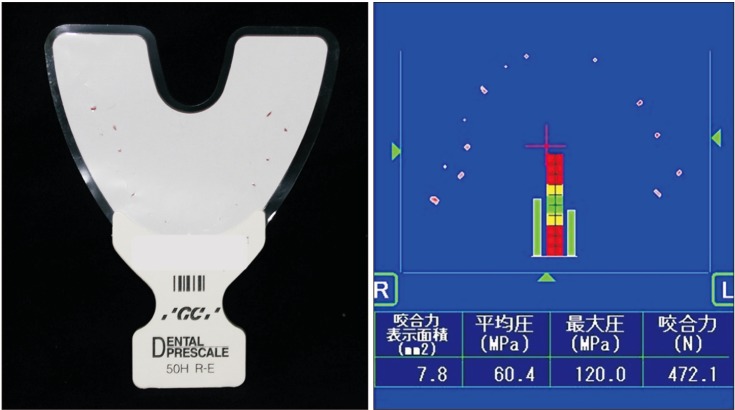
Occlusal force and occlusal contact area were evaluated using the Dental Prescale System (Figure 2). This system consists of pressure-sensitive films that include polyethylene terephthalate films and color-marking microcapsules, which collapse and chemically yield a red coloration during occlusion. The films (50H, Type R) were selected to fit the entire dental arch of each subject, and the subjects were asked to occlude on the film with maximal clenching force for 5 seconds in the natural head position. A CCD camera (Occluzer FPT 707; Fuji Film Corp.), which is a color image scanner, was used to analyze the occlusal force and contact area with a resolution of 0.1 N and 0.1 mm2, respectively.
A cephalogram was generated using the CBCT images, and the subjects were divided into the Class I, II, and III groups on the basis of the ANB angle (angle between A point, Nasion, and B point) followed by an examination of first molar relationships2: Class I group, 0° < ANB < 4° and Angle Class I molar relationship; Class II group, ANB > 4° and Angle Class II molar relationship; and Class III group, ANB < 0° and Angle Class III molar relationship. The demographic data of the subjects are shown in Table 3. This study was approved by the Institutional Review Board of Gangnam Severance Hospital, Yonsei University (IRB No. 3-2018-0038).

Statistical analysis
All measurements were performed by two examiners (S.J. and S.K.) with at least 2 years of experience analyzing CBCT images. For assessing intraexaminer and interexaminer reliability, 20 images were randomly selected at a 2-week interval and were assessed for a second time; these assessments showed high reliability coefficients (0.91 < r < 0.98).
Based on the findings of a previous study,11 a minimum sample size of 10 subjects per group was determined (G*Power 3; Heinrich-Heine-Universität Düsseldorf, Dusseldorf, Germany) at α = 0.05, power of 90%, and effect size of 0.8 to detect differences in occlusal force between the different malocclusion types by using analysis of variance (ANOVA). The normality of variables was tested using the Kolmogorov–Smirnov test. The mean and standard deviation of transverse skeletal parameters and dental inclinations were analyzed. A linear mixed model for a repeated-measures covariance pattern model with compound symmetry covariance within subjects was used to cluster the posterior teeth into four groups: maxillary premolar, maxillary molar, mandibular premolar, and mandibular molar groups. The variables were compared according to sex by using independent two-sample t-tests. Different sagittal skeletal malocclusion types (Class I, II, and III) were compared for premolar and molar inclinations, together with occlusal force and contact area, using the ANOVA test and the least significant difference post-hoc test. Correlations of posterior dental inclinations to occlusal force and contact area were analyzed using Pearson's correlation analysis. A p-value of less than 0.05 was considered statistically significant. Statistical analysis was conducted using SAS vers. 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Transverse widths, dental inclinations, occlusal force, and contact area of different malocclusions were evaluated in male and female subjects separately because significant sex difference existed in several parameters (Supplementary Table 2).
In male subjects, the buccal mandibular width was significantly smaller in the Class II group than in the Class I group, and the mandibular alveolar width was significantly smaller in the Class III group than in the Class I group. When evaluating the inclination of the clustered groups, Class II maxillary premolars had smaller inclinations than did the Class I and III groups; the maxillary molars had the greatest inclination in the Class III group and the smallest inclination in the Class II group; and the mandibular premolars in the Class I group had the smallest inclination (p < 0.05). Occlusal force and contact area did not show significant difference according to sagittal skeletal malocclusion groups in male subjects (Table 4, Supplementary Table 3).
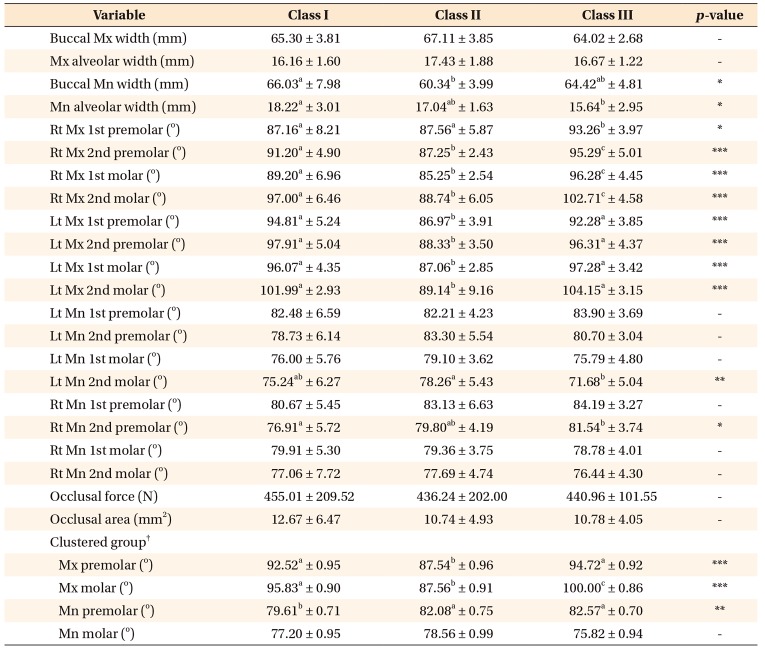
Table 4
Transverse widths, dental inclinations, and occlusal function of male subjects with Class I, II, and III malocclusions
Values are presented as mean ± standard deviation unless otherwise indicated.
Mx, Maxillary; Mn, mandibular; Rt, right; Lt, left.
a, b, c: Different superscript letters indicate statistical difference between the Class I, II, and III groups (*p < 0.05, **p < 0.01, ***p < 0.001).
†Values are presented as mean ± standard error.
![]()
In female subjects, the buccal mandibular width was significantly smaller in the Class II group than in the Class III group. Upon evaluation of inclinations of the clustered groups, Class III maxillary premolars had the greatest inclination among the groups; maxillary molars had the greatest inclination in the Class III group and the smallest inclination in the Class II group; Class III mandibular premolars showed the greatest inclination, while Class III mandibular molars had the smallest inclination among the other two groups (p < 0.05). No significant difference was observed in occlusal force and contact area when comparing different sagittal skeletal malocclusion groups in female subjects (Table 5, Supplementary Table 3).
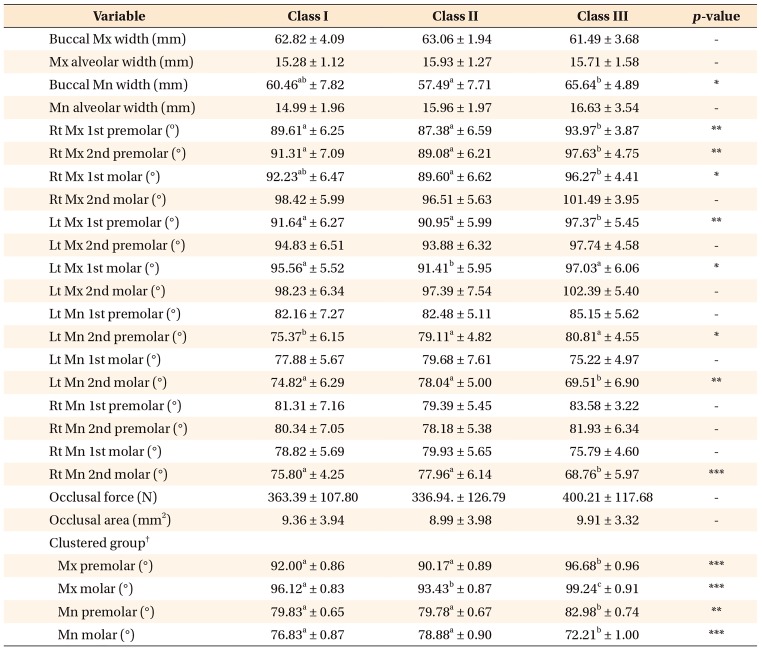
Table 5
Transverse widths, dental inclinations, and occlusal function of female subjects with Class I, II, and III malocclusions
Values are presented as mean ± standard deviation unless otherwise indicated.
Mx, Maxillary; Mn, mandibular; Rt, right; Lt, left.
a, b, c: Different superscript letters indicate statistical difference between the Class I, II, and III groups (*p < 0.05, **p < 0.01, ***p <0.001).
†Values are presented as mean ± standard error.
![]()
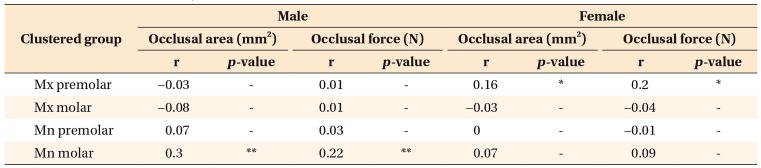
The subjects were combined regardless of the type of malocclusions, and posterior tooth inclinations of the clustered groups were analyzed for correlations with occlusal force and contact area. In male subjects, mandibular molar inclination weakly correlated with occlusal force and contact area (r < 0.3). In female subjects, maxillary premolar inclination weakly correlated with occlusal force and contact area (r < 0.2) (Table 6).
Supplementary data is available at https://doi.org/10.4041/kjod.2020.50.2.98.
DISCUSSION
When a subject does not have a balanced skeletal relationship, the posterior teeth may be compensated within the dental arch to display functional occlusion. This also occurs often in an iatrogenic manner during orthodontic treatment because teeth are aligned to accommodate the existing skeletal discrepancies, which may result in different posterior tooth inclinations depending on the treatment modality. Subjects with different sagittal skeletal malocclusions have underlying transverse discrepancies that require compensatory dental inclinations for masticatory function.2 Accordingly, a 3D evaluation of posterior tooth inclinations in subjects with Class II and III malocclusions and assessment of occlusal force and contact area would provide clinically useful information, because the force upon mastication is not directed along the long axis of the tooth, which could affect the quality of occlusal function and cause negative periodontal effects.12
Previous studies showed decreased occlusal force in long-faced individuals, indicating a close relationship between vertical facial patterns and occlusal function.813 These studies suggested that vertical facial patterns could be affected by muscular differences, which cause a difference in masticatory function. Therefore, prior to starting the current study, a preliminary study was conducted on 144 adults with Class I malocclusion and hypodivergent, normodivergent, and hyperdivergent facial profiles to explore the differences in occlusal force and contact area by using the Dental Prescale System. In both male and female subjects, the mean occlusal force and contact area increased in the order of hyperdivergent, normodivergent, and hypodivergent groups, with significantly lower values in the hyperdivergent group (Table 1, 2). Therefore, to minimize factors related to vertical skeletal dimensions and subsequent muscular influences, this study was limited to normodivergent subjects when evaluating posterior tooth inclinations and occlusal force values in different sagittal skeletal malocclusion groups.
CBCT coronal planes obtained at the location of premolars and molars were used to analyze the inclinations of each posterior tooth. Although the sample strictly followed the inclusion criteria, variations in individual tooth inclinations were observed in male and female subjects as well as within the Class I, II, and III groups. This may be considered a natural finding as it represents the diversity of subjects, but it is a limitation of this study. Therefore, posterior tooth inclinations were clustered into the maxillary premolar, maxillary molar, mandibular premolar, and mandibular molar groups to show the tendency of dental inclinations according to different sagittal skeletal patterns. The maxillomandibular widths were also evaluated, as previous studies suggested the occurrence of dental compensation to overcome the transverse skeletal discrepancy in different sagittal skeletal malocclusions.21415 In both male and female subjects, the buccal mandibular width was significantly narrower in the Class II group than in the other two groups, which was similar to the findings of previous reports.1516 This was caused by the relative posterior position of the mandible compared to that of the maxilla in the Class II group. To overcome the transverse skeletal discrepancy, the clustered maxillary premolars and molars in Class II males and the clustered maxillary molars in Class II females had significant lingual tipping compared to the other malocclusion groups. There was no significant difference in buccal maxillary width among the 3 malocclusion groups and the mandibular alveolar bone width was greater in Class I males compared to Class III males. This could be attributed to the exclusion of severe cases of skeletal sagittal malocclusion, by limiting the subjects to normodivergent adults without crossbites, as well as to individual variations. Nonetheless, dental compensation in adults with Class III malocclusion showed similar tendencies to those reported in previous studies showing narrow maxillary widths.217 The clustered maxillary molars in Class III males and both clustered maxillary premolars and molars in Class III females showed significant buccal flaring while the clustered mandibular molars in Class III females had greater lingual tipping with a similar tendency in males. When evaluating clustered dental inclinations according to the occlusal plane, the maxillary molars showed lingual tipping in the Class II and buccal flaring in the Class III groups. In male subjects, the mandibular molars were buccally flared in the Class II and lingually tipped in the Class III groups, with a similar trend in female subjects. In brief, adults with Class II and Class III malocclusions showed greater compensatory tipping of the maxillary and mandibular posterior teeth than did adults with good Class I occlusion.
Masticatory performance is correlated with occlusion, because subjects with better masticatory performance show good distribution of occlusal contact areas.1819 Therefore, several previous studies have evaluated occlusal force and contact area to ascertain occlusal function.1920 In this study, the Dental Prescale System was used because it was relatively simple to use in practice and did not require any specific measuring device other than a thin pressure-sensitive film to cover the occlusal surface.62122 Although a possibility of overestimation of bite force exists because of technical limitations of the color scanning system, bite force and occlusal contact area are comfortably measured close to the maximal intercuspal position with good reproducibility.23 This is an advantage over the rigid material used in the T-scan system,24 which may include unnecessary shift or displacement of the mandible due to the inadequate flexibility of the device. In the current study, the Dental Prescale System was applied in a consistent matter by examiners with at least 2 years of dental training to ensure that the subjects were seated in a natural head position, the pressure-sensitive films were fitted to include the entire dental arch, and care was taken to avoid interference of the buccal mucosa or tongue, so as not to deform the film during maximal clenching.
In this study, upon combining the results from the CBCT images the Dental Prescale System, although the posterior teeth showed significant compensatory inclinations in subjects with Class II and III malocclusions, neither occlusal force nor contact area was significantly different in the normodivergent Class I, II, and III malocclusion groups. Furthermore, the posterior dental inclinations of only two clustered groups were weakly correlated, at most, to occlusal function. It is reasonable to suggest that as long as the entire dentition is in functional contact and does not have any evident crossbite, adults with Class II and III malocclusions with normal vertical facial patterns may not experience more significant differences in occlusal force or contact area than would adults with good Class I occlusion. This would be beneficial in terms of occlusal function for subjects undergoing orthodontic treatment in normodivergent Class II or Class III cases as considerable amount of compensation in posterior tooth inclinations may occur to overcome the skeletal discrepancy.
The subjects included in this study were comprised of young adults who were 17 to 40 years old. This was because the maximum bite force has been reported to progressively increase between the age of 7 to 17 years and remain fairly constant until about 40 years of age before starting to decline.2526 Although the age range was restricted to minimize occlusal changes due to natural aging and occlusal wear, this was a limitation of this study. As mentioned before, to minimize the influence of muscle function from vertical facial patterns, subjects with extreme vertical dimensions were excluded from this study by limiting the inclusion criteria to subjects with normodivergent facial patterns. The findings of this study were also different from those of other reports using dynamic methods of mastication by quantifying median particle size after breakdown of food particles, which showed the negative effects of Class II and III malocclusions on masticatory performance.2728 Therefore, results of this study help provide a standard for occlusal force and contact area values in subjects with Class I, II, and III malocclusions with normal vertical dimensions in static occlusion of maximum closure.
The following limitations should be considered when interpreting the results of this study. First, severe cases of different sagittal skeletal malocclusions were excluded as the inclusion criteria were limited to normodivergent adults without crossbite. In addition, slight dental crowding could have influenced dental inclinations even though the crowding was limited to less than 5 mm. Second, despite the convenience and advantages of the Dental Prescale System, it has systematic limitations that should be considered. Although a relatively thin pressure-sensitive film of 97 µm was used, any contact below this value could not be assessed, and bite disturbing proprioception may be disturbed even with an aluminum foil as thin as 20 µm.23 Third, although agreement is lacking on the association between dynamic and static occlusions depending on the registration materials and protocols used, this method measured static occlusion, which does not consider jaw muscle activities or movements, such as lateral excursive or protrusive patterns.2930 Further studies including masticatory movements and muscular activity are needed for evaluating dynamic occlusion in adults with Class II and III malocclusions.
CONCLUSION
1. Premolars and molars showed significant compensatory inclinations in different sagittal skeletal malocclusions to overcome the transverse skeletal discrepancy on CBCT images.
2. The occlusal force or contact area was similar in normodivergent adults with Class I, II, and III malocclusions.
3. In normodivergent adults, the occlusal force or contact area is not significantly affected even though the posterior teeth may show inclination differences due to transverse discrepancies in different sagittal skeletal malocclusions.
 XML Download
XML Download