

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The lip-closing function or lip pursing is an essential initial movement during various functions of the stomatognathic system, including food intake, chewing, swallowing, speech, and facial expressions.12 According to the equilibrium theory, the force exerted by the lips and tongue could be an important component for stability of the dentition.34 In addition, lip competency without any strain in the mandibular rest position is crucial for an attractive facial appearance.5
With regard to the lip force, primarily in the rest position, static pressure may have a remarkable impact on the teeth and jaws.6 Tomiyama et al.7 reported that the electromyographic activity of the orbicularis oris muscle in the clinical rest position was greater in subjects with incompetent lips than in those with competent lips. In contrast, other study showed that the electromyographic activity of the orbicularis oris muscle at rest was similar in subjects with competent lips and those with incompetent lips.8 However, thus far, there is disagreement regarding the resting lip force.
The maximum strength of the lips is considered to reflect the forces from the lips.9 Some studies have reported a relationship between the lip-closing force and malocclusion or the facial morphology. Specifically, the lip-closing force was found to be weak in patients with bilateral cleft lip10 or mandibular asymmetry.11 Moreover, Doto and Yamada12 found that the lip-closing force was weaker in patients with skeletal Class II malocclusion than in those with skeletal Class III malocclusion. Meanwhile, Takehana et al.13 recently reported that the lip-closing force was correlated with the maxillary dental arch morphology, particularly the arch length and width, in patients with Class I malocclusion. Because orthodontic treatment changes the dental arch morphology, it could also alter the lip-closing force.
The lip position and other related features may be changed by orthodontic or orthopedic treatment. Orthodontic extraction in patients with Class II division 1 (II/1) malocclusion or bialveolar protrusion can help in relieving the lip protrusion by facilitating retraction of the maxillary and mandibular incisors, thus resolving the lip incompetence and improving the facial profile.1415 In addition to the enhancement of facial esthetics, an improvement in the lip-closing force after surgical-orthodontic approaches, such as orthognathic surgery1617 and surgically assisted rapid palatal expansion18 was recently reported. Considering the previous studies, there have been few studies on the changes in the lip-closing force after orthodontic treatment and their correlation with dentofacial and dental arch dimensional changes.
Therefore, the aims of this study were to evaluate the changes in the maximum lip-closing force (MLF) after orthodontic treatment with or without premolar extractions and verify the correlation of these changes with skeletal, dental, and soft tissue variables and the dental arch morphology. The null hypothesis was that there would be no significant difference in MLF between extraction and nonextraction orthodontic treatment.
Go to : 
MATERIALS AND METHODS
This retrospective cohort study was reviewed and approved by the Institutional Review Board at Seoul National University Bundang Hospital (B-1703-387-101). A total of 32 consecutive patients were selected from adult patients who underwent comprehensive orthodontic treatment performed by an experienced orthodontist at Seoul National University Bundang Hospital (Seongnam Korea) between April 2012 and July 2016. Specifically, women who underwent orthodontic treatment with or without extraction of the four first premolars for the resolution of dental crowding and/or protrusion were considered eligible. Other inclusion criteria were as follows: a Class I or Class II (< 1/2 Class II) molar relationship, absence of a posterior crossbite/scissor bite, and competent lips (interlabial gap < 3.0 mm). Patients were excluded if they exhibited a skeletal pattern where ANB was > 5° or < 0°, skeletal asymmetry (menton deviation > 1 mm), cleft lip/palate, other craniofacial syndromes, and/or multiple missing teeth.
The enrolled subjects were allocated to two groups. The extraction group comprised 15 women aged 24.6 ± 5.8 years who underwent extraction of the four first premolars. The nonextraction group comprised 17 women aged 28.6 ± 8.4 years who were treated without extraction. Lateral cephalograms were acquired and study models were fabricated before (T0) and after (T1) the treatment. All lateral cephalograms were traced and analyzed using V-ceph software ver. 6.0 (Osstem, Seoul, Korea) by an orthodontist (S.-H.K.) to evaluate the dentoskeletal and soft tissue changes in each subject (Figure 1). The same investigator evaluated changes in the dental arch morphology by measuring the study models using a digital caliper (Mitutoyo Corp., Kawasaki, Japan; Figure 2).
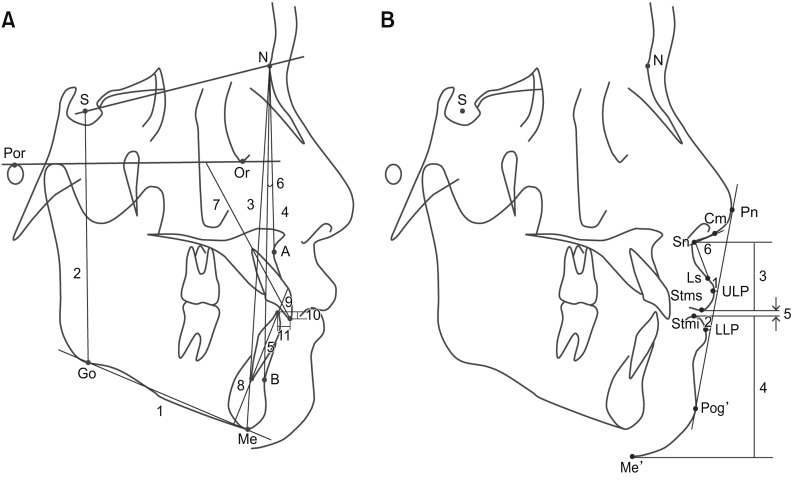 | Figure 1Landmarks, reference planes, and measurements in cephalometric analyses.
A, Dentoskeletal variables. S, Sella; N, nasion; Por, porion; Or, orbitale; Me, menton; Go, gonion; A, A point; B, B point; U1, upper central incisor; L1, lower central incisor; SN plane (S-N); FH plane, Frankfort horizontal plane (Or-Por); mandibular plane (Go-Me); 1, angle between FH plane and mandibular plane (FMA); 2, S to Go (posterior facial height, PFH); 3, N to Me (anterior facial height, AFH); 4, angle between the SN plane and N-A line (SNA); 5, angle between the SN plane and N-B line (SNB); 6, angle between the N-A line and N-B line (ANB); 7, angle between the long axis of U1 and the FH plane (U1-FH); 8, angle between the long axis of L1 and the mandibular plane (IMPA); 9, angle between the long axis of U1 and the long axis of L1 (interincisal angle); 10, overbite; 11, overjet. B, Soft tissue variables. Pn, Pronasale; Cm, columella; Sn, subnasale; Ls, labrale superius; ULP, upper lip point; LLP, lower lip point; Stms, lowest point on the upper lip; Stmi, highest point on the lower lip; Pog', soft tissue pogonion; Me', soft tissue menton; 1, Rickett's E line (Pn-Pog'; EL) to ULP; 2, EL to LLP; 3, Sn to Stms; 4, Stmi to Me’; 5, interlabial gap (distance from Stms to Stmi); 6, nasolabial angle (angle between the Sn-Cm line and the Sn-Ls line).
|
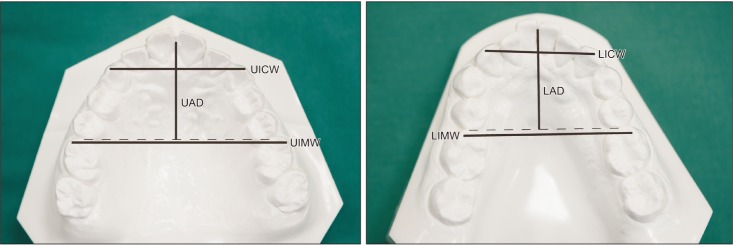 | Figure 2Measurements of the dental arch morphology on study models.UICW/LICW, Distance between both canine cusp tips in the maxillary/mandibular arch; UIMW/LIMW, distance between the mesiobuccal cusp tips of both first molars in the maxillary/mandibular arch; UAD/LAD, distance from the contact point between the central incisors perpendicular to a line connecting the mesial contact points of both first molars in the maxillary/mandibular arch.
|
MLF measurement
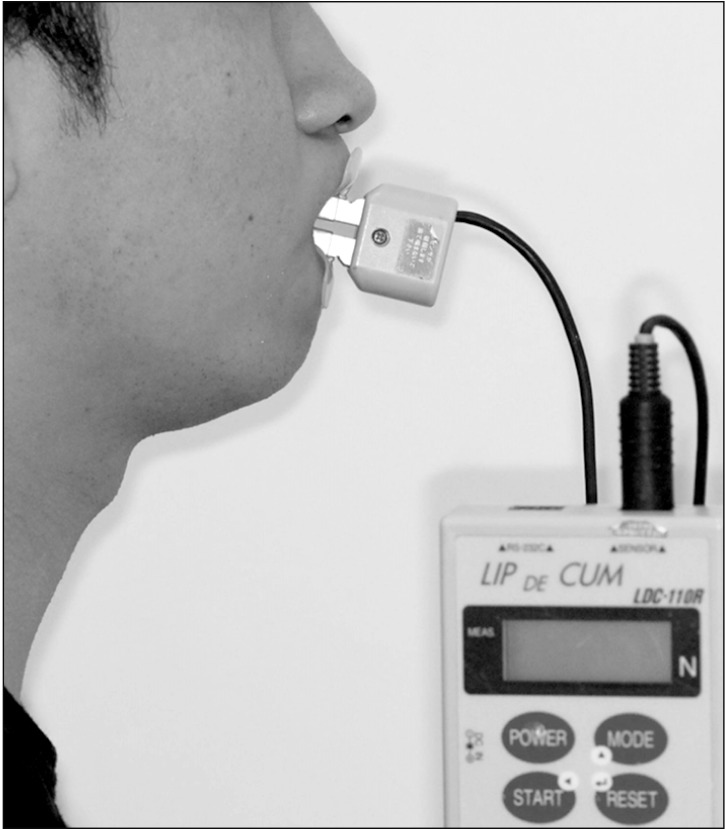
At both T0 and T1, MLF was measured using the Lip De Cum LDC-110R® device (Cosmos instruments Co. LTD, Tokyo, Japan). The lip-closure force indicator with the lip holder (Ducklings®) was connected to a sensor, and the measured value was converted to the SI unit for force (newton, N). All subjects were instructed to sit upright, position the lip holder between the lips, and close their lips with the maximum possible strength, while avoiding contact between the maxillary and mandibular teeth (Figure 3). MLF was measured twice by a single evaluator, with a 5-minute interval between measurements. Subsequently, the average value was calculated and analyzed.
Statistical analysis
The sample size was determined according to the changes in MLF observed in our preliminary study using PASS 11 (NCSS, Kaysville, UT, USA), with an α level of 0.05 and a power of 80%. The results revealed that a minimum of nine patients per group was required.
Depending on the normality of data as determined by the Shapiro–Wilk test, the paired t-test or the Wilcoxon signed-rank test was used to analyze changes (T1-T0) in the cephalometric and dental arch morphology measurements and MLF within each group. The independent t-test or the Mann–Whitney U test was used to compare pretreatment variables (T0) and changes (T1–T0) in the cephalometric and dental arch variables and MLF between the two groups. Pearson's correlation analysis was used to verify the associations between dentoskeletal changes and changes in MLF. All statistical analyses were performed using IBM SPSS Statistics ver. 22.0 for Windows (IBM Corp., Armonk, NY, USA). A p-value for < 0.05 was considered statistically significant.
A high degree of reliability was found for all measurements. The mean intraclass correlation coefficients (95% confidence interval) for the cephalometric measurements, arch depth, intercanine width, intermolar width, and MLF were 0.941 (0.781 to 0.999), 0.987 (0.979 to 0.992), 0.997 (0.995 to 0.998), 0.994 (0.989 to 0.996), and 0.932 (0.890 to 0.958), respectively (p < 0.001 for all).
Go to :
RESULTS
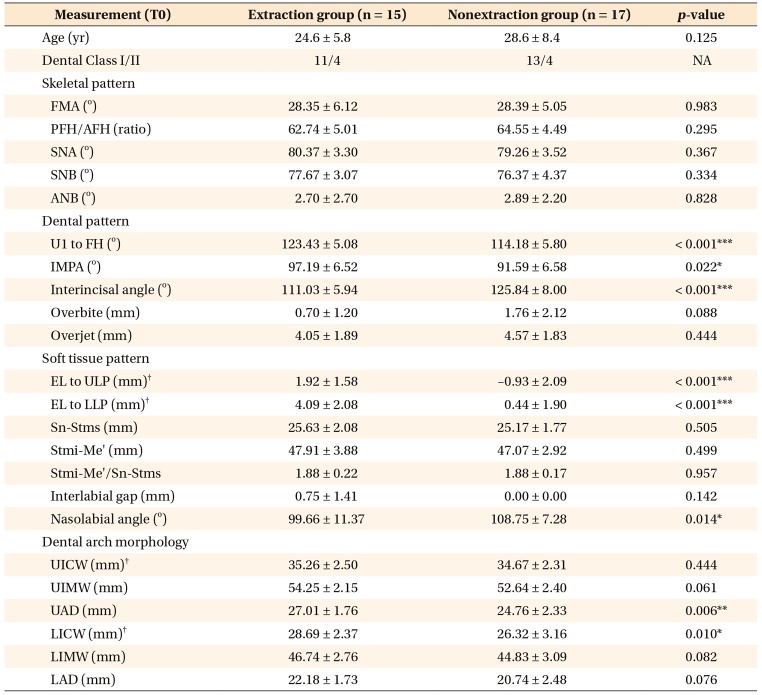
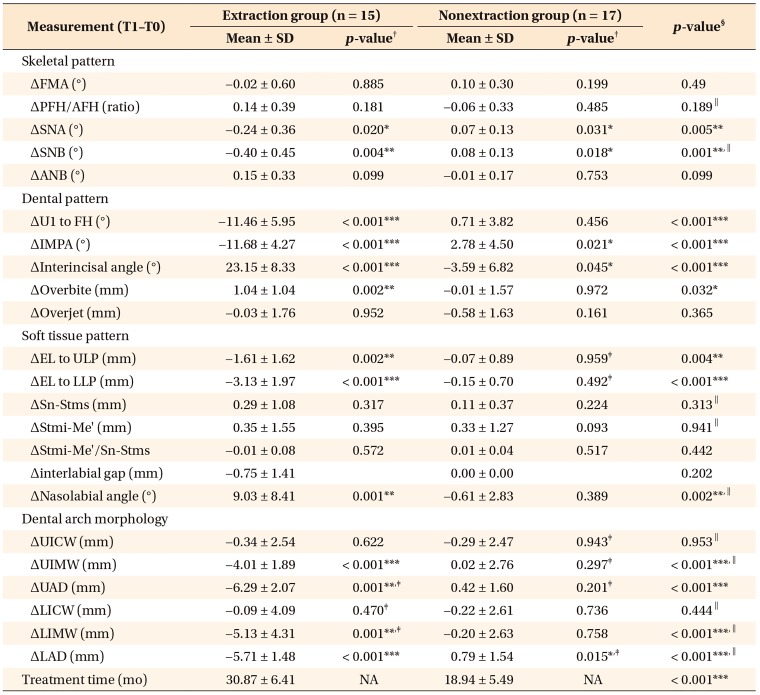
As presented in Table 1, the extraction and nonextraction groups showed no difference in the skeletal pattern at T0, although there were significant differences in the dental and soft tissue measurements. The extraction group exhibited significantly larger values for the angle between the long axis of the upper central incisor (U1) and the Frankfort horizontal (FH) plane (U1-FH; 123.43° vs. 114.18°), distance from Rickett's E line (EL) to the upper lip point (ULP; 1.92 mm vs. −0.93 mm), distance from EL to the lower lip point (LLP; 4.09 mm vs. 0.44 mm; p < 0.001 for all comparisons), the incisor–mandibular plane angle (IMPA; 97.19° vs. 91.59°; p < 0.05), the lower intercanine width (LICW; 28.69 mm vs. 26.32 mm; p < 0.05), and the upper arch depth (UAD; 27.01 mm vs. 24.76 mm; p < 0.01), while it showed smaller values for the interincisal angle (111.03° vs. 125.84°; p < 0.001) and nasolabial angle (99.66° vs. 108.75°; p < 0.05).
At T1, the extraction and nonextraction groups showed no significant differences in any cephalometric variable except IMPA (85.52° vs. 94.38°, respectively; p < 0.01), the interincisal angle (134.18° vs. 122.25°; p < 0.001), and EL to ULP (0.31 mm vs −1.00 mm; p < 0.05). Most dental arch-related variables showed significant differences between groups; these included (extraction vs. nonextraction) the upper intermolar width (UIMW; 50.24 mm vs. 52.65 mm; p < 0.01), UAD (20.71 mm vs. 25.19 mm; p < 0.001), LICW (28.61 mm vs. 26.11 mm; p < 0.01), the lower intermolar width (LIMW; 41.61 mm vs. 44.63 mm; p < 0.01), and the lower arch depth (LAD; 16.46 mm vs. 21.53 mm; p < 0.001).
From T0 to T1, the extraction group exhibited significant decreases in U1–FH (−11.46°), IMPA (−11.68°), EL to LLP (−3.13 mm; p < 0.001 for all), EL to ULP (−1.61 mm; p < 0.01), UIMW (−4.01 mm), UAD (−6.29 mm), LIMW (−5.13 mm), and LAD (−5.71 mm; p < 0.001 for all). Meanwhile, the interincisal angle (23.15°; p < 0.01), overbite (1.04 mm; p < 0.01), and nasolabial angle (9.03°; p < 0.01; Table 2) exhibited increases. The nonextraction group showed significant increases in IMPA (2.78°) and LAD (0.79 mm; p < 0.05 for both) and a decrease in the interincisal angle (−3.59°; p < 0.05; Table 2). The decreases in U1 to FH, IMPA, EL to LLP, UIMW, LIMW, LAD (p < 0.001 for all), EL to ULP (p < 0.01), and UAD (p < 0.01), as well as the increases in the interincisal angle (p < 0.001), treatment duration (p < 0.001), overbite (p < 0.05), and nasolabial angle (p < 0.01), were significantly greater in the extraction group than in the nonextraction group (Table 2).
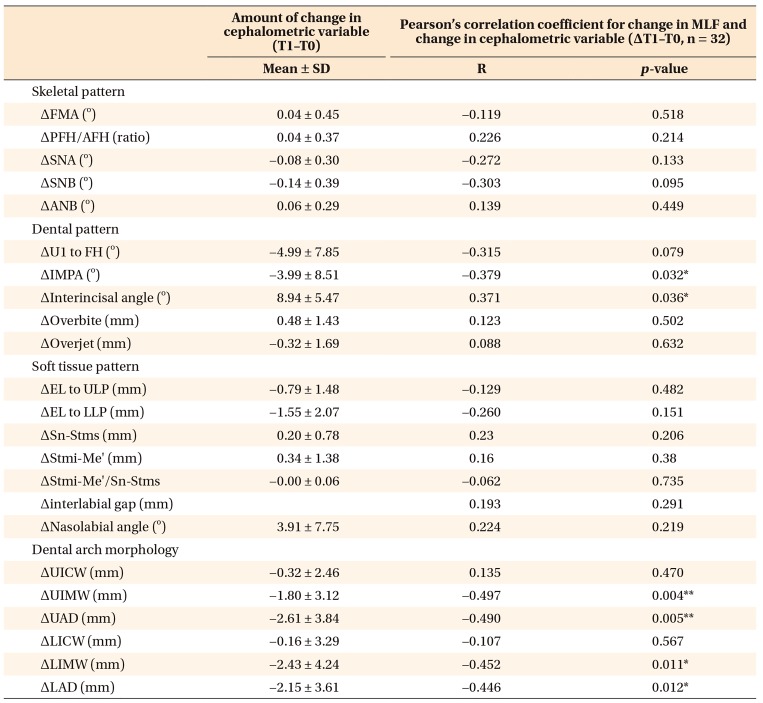
The extraction and nonextraction groups showed no significant difference in MLF at T0 (6.35 N vs. 7.92 N; Table 3). MLF significantly increased from T0 to T1 in the extraction group (3.25 N, p < 0.01), and this increase was significantly greater than that (0.69 N) in the nonextraction group (p < 0.05; Table 3). The increase in MLF was correlated with the decreases in IMPA (R = −0.379), LIMW (R = −0.452), LAD (R= −0.446; p < 0.05 for all), UIMW (R = −0.497; p < 0.01), and UAD (R = −0.490; p < 0.01) and the increase in the interincisal angle (R = 0.371; p < 0.05; Table 4).

Table 3
Comparison of the baseline and the amount of changes in the MLF in each group, between the groups and in all groups
MLF, Maximum lip-closing force; N, newton; SD, standard deviation; T0, before treatment; T1, after treatment; T1–T0, change from T0 to T1; NA, not applicable.
*p < 0.05, **p < 0.01.
†Paired t-tests were performed to compare differences between T0 and T1 in each group or total subjects.
‡Independent t-test was performed to compare intergroup difference between extraction and nonextraction groups.
![]()
Go to :
DISCUSSION
Orthodontic treatment involving premolar extraction is commonly used for the correction of dentoskeletal malocclusion, which may be accompanied by an imbalance in the perioral musculature. Orthodontic treatment with or without extraction causes morphological changes in the perioral soft tissue, including the lips. Thus, it has been of great interest to orthodontists from the perspective of facial esthetics.1415 However, research on lip function is lacking. A comparison of the lip-closing force before and after orthodontic treatment may provide insights into the recovery of stomatognathic functions and improvement of facial esthetics. Despite these considerations, changes in the lip-closing force after various orthodontic treatments have rarely been studied. Therefore, the present study evaluated the changes in MLF after orthodontic treatment with or without premolar extractions and determined the relationships between these changes and hard/soft tissue changes.
The voluntary MLF is used as a parameter for lip function evaluation,19 and an available measuring tool that noninvasively facilitates quantitative assessments has been reported for this purpose. Thus, MLF has been used as a functional indicator for the lip or perioral muscles in studies on the effects of the lips on the craniofacial structure or studies involving measurement of the lip strength after surgical–orthodontic treatment.16171820
The lip force can be affected by various factors, including age, gender, and skeletal and dental patterns;171821222324 therefore, we only included women with Class I and mild Class II malocclusion in the present study. At T0, the extraction and nonextraction groups exhibited no significant differences in the vertical and sagittal skeletal measurements (Table 1), which indicated a similar skeletal pattern in the two groups. However, with regard to the dental and soft tissue patterns and dental arch morphology, the extraction group exhibited greater incisor proclination, lip protrusion, UAD, and LICW than did the nonextraction group (Table 1). While MLF at T0 was lower in the extraction group than in the nonextraction group (6.35 N vs. 7.92 N), the difference was not significantly different (Table 3). This result was consistent with the findings of Ingervall and Janson,25 who reported that the lip strength did not correlate with the dentoalveolar cephalometric variables in patients with Class I or Class II malocclusion. Partal and Aksu26 also found that the vertical lip pressure did not differ between subjects with Class I malocclusion and those with Class II division 2 (II/2) malocclusion. In contrast, some studies suggested that the lip strength in individuals with Class II/1 malocclusion was lower than that in individuals with Class I malocclusion.2127 Posen9 reported that subjects with bimaxillary protrusion exhibited a low lip strength while those with Class II/2 malocclusion exhibited high lip strength. Jung et al.20 reported that maxillary incisor proclination was related to the closing force of the upper lips. These inconsistent results could be attributed to differences in the area of measurement and methodology according to the measuring tools used during voluntary lip closing.
In the present study, the extraction group showed significantly decreased lip protrusion and incisor retraction relative to those in the nonextraction group from T0 to T1; this was because of closure of the extraction space (Table 2). Similar results were reported in previous studies on facial profile changes after extraction treatment.1528 In addition, the decreases in the arch depth and molar width in both the maxilla and mandible were more pronounced in the extraction group than in the nonextraction group. This finding is consistent with those of Aksu and Kocadereli29 and Herzog et al.,30 who found that the maxillary and mandibular intermolar and perimeter measurements after treatment involving premolar extraction were decreased relative to those after nonextraction treatment in patients with Class I malocclusion.
We found that the increase in MLF after treatment was significantly greater in the extraction group than in the nonextraction group (Table 3). Moreover, cephalometric variables, namely IMPA and the interincisal angle, as well as most dental arch-related variables (UIMW, UAD, LICW, LIMW, and LAD) exhibited differences between the two groups at T1; this was not observed at T0. We also found significant correlations between the change in MLF and the changes in UIMW, UAD, LIMW, LAD, IMPA, and the interincisal angle at T1. These results imply that the increase in MLF could be associated with the decrease in not only the incisor inclination but also the anteroposterior and transverse arch dimensions in the maxilla and mandible. A decrease in the arch depth and width after extraction orthodontic treatment might influence the function of the buccinator and orbicularis oris muscles during lip closure. A previous cross-sectional study involving untreated patients with Class I malocclusion suggested that the function of the buccinator and orbicularis oris muscles affects the arch morphology.13 However, it remains unclear whether a change in form may affect muscle function, or vice versa.
The present study has some limitations. The tool used for MLF measurement cannot differentiate the effects of the upper and lower orbicularis oris muscles. In addition, the lip-closing force may be associated with the tongue force,27 which was not considered in this study. Considering that muscles adapt to changed circumstances, further investigations are needed to evaluate long-term or time-course changes in the perioral muscle activity or lip-closing force after different types of orthodontic or surgical–orthodontic treatments.
Go to :
CONCLUSION
In conclusion, the null hypothesis for this study was rejected. The findings suggest that MLF increases to a greater extent during extraction orthodontic treatment than during nonextraction orthodontic treatment. This increase may be correlated with the changes in the maxillary and mandibular arch depths and intermolar widths as well as incisor inclination.
Go to :
 XML Download
XML Download