

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although the causality of this relationship is uncertain, vitamin D deficiency is associated with type 2 diabetes and metabolic syndrome [1234]. Vitamin D is fat-soluble and is essential for bone and calcium metabolism [56]. It is also well-known that vitamin D is involved in glucose homeostasis by facilitating the action and secretion in insulin [78]. Many studies have shown that either insulin release and insulin sensitivity could be improved or type 2 diabetes could be prevented by vitamin D suf recent meta-analyses have reported that such anpplements [91011]. However, randomized clinical trials for vitamin D supplements have shown inconsistent results [1213].
Gestational diabetes mellitus (GDM) is diabetes that is newly diagnosed in the second or third trimester of pregnancy that is not clearly either preexisting type 1 or type 2 diabetes and its prevalence has been increasing worldwide [141516]. Vitamin D deficiency is common in pregnant women and is recognized as an emerging issue in global health [171819]. Recently gathered evidence suggests that vitamin D deficiency in the two first trimesters of pregnancy increase the risk of insulin resistance and developing GDM [202122]. GDM is characterized by compensatory failure of insulin secretion in response to increased insulin resistance during pregnancy. In addition, increased insulin resistance and decreased insulin secretion due to vitamin D deficiency during mid-pregnancy might continuously influence on postpartum glucose intolerance [232425]. Nowadays, postpartum monitoring for glucose intolerance has been increasing in importance, because GDM is associated with an increased risk for developing type 2 diabetes after delivery [2526]. However, there are few studies that have examined the effect of vitamin D deficiency at mid-pregnancy on postpartum glucose intolerance in patients with GDM. The aim of this study was to evaluate the association between serum 25-hydroxyvitamin D (25(OH)D) at mid-pregnancy and postpartum glucose intolerance in women with GDM.
Go to : 
METHODS
Participants and design
We conducted this observational study in CHA Bundang Medical Center (Seongnam, Korea) from August 2012 to October 2016, enrolling 348 pregnant women diagnosed with GDM and aged ≥20 years. We used a ‘two-step’ approach for diagnosis of GDM. First, we used a 1-hour 50-g glucose load test as screening at 24 to 28 weeks of gestation. We offered a 3-hour 100-g oral glucose tolerance test (OGTT) to woman who had a 1-hour post-load plasma glucose level >140 mg/dL. According to the Carpenter and Coustan criteria, the diagnosis of GDM can be made if at least two of the four plasma glucose levels (measured fasting and 1, 2, and 3 hours after the 100-g OGTT) were met or exceeded. We excluded women who were known to have had type 1 or type 2 diabetes before pregnancy, thyroid disorders, twin pregnancy, and a history of taking vitamin D supplements during pregnancy.
At 24 to 32 weeks of gestation (baseline visit), we carried out anthropometric assessments, measured blood pressure, and did laboratory tests, including fasting glucose, hemoglobin A1c (HbA1c), lipid profiles, and serum 25(OH)D level for all study participants. We collected medical histories from medical records. These women were given medical nutrition therapy and/or insulin treatment during their antenatal follow-up. We evaluated postpartum glycemic status by 75-g OGTT at 6 to 12 weeks after delivery. We defined glucose intolerance as fasting plasma glucose (FPG) ≥100 mg/dL or 2-hour plasma glucose ≥140 mg/dL. This study was approved by the Institutional Review Board of CHA Bundang Medical Center at CHA University School of Medicine (2017-08-004), and we obtained informed consent from all study participants.
Clinical and laboratory measurements
Height and weight were measured for all subjects when they were wearing minimal clothing and no shoes. We measured blood pressure by trained nurses using automatic sphygmomanometer while the participants were seated for 10 minutes. Serum 25(OH)D levels were measured by the chemiluminescence immunoassay (ADVIA Centaur XP, Siemens Healthcare, Tarrytown, NY, USA). We measured plasma glucose, total cholesterol, triglyceride, and high density lipoprotein cholesterol (HDL-C) using a Hitachi 7600 analyzer (Hitachi, Tokyo, Japan). We measured HbA1c using high-performance liquid chromatography (before May 2013, Bio-Rad Variant II, Hercules, CA, USA; after May 2013, Tosoh G8, San Francisco, CA, USA). We assessed C-peptide and insulin by the chemiluminescence immunoassay (Roche Diagnostic GmbH, Mannheim, Germany). We carried out the homeostasis model assessment of insulin resistance (HOMA-IR) and β-cell function (HOMA-β) according to suggested formulas [27].
Statistical analysis
Data for categorical factors are reported as percentages, and continuous variables are presented as the mean±SD. Vitamin D deficiency was defined as serum 25(OH)D <20 ng/mL. We grouped seasons depending on the date of sample collection for serum 25(OH)D analysis (spring, March to May; summer, June to August; autumn, September to November; winter, December to February). All statistical analyses were done using SPSS version 19.0 software (IBM Co., Armonk, NY, USA).
Go to :
RESULTS
Table 1 shows the baseline characteristics of the women with GDM at mid-pregnancy. The mean age was 33.1 years and the gestational weeks were 27.8 weeks. Among the 348 women with GDM, 267 women (76.7%) were vitamin D deficiency at baseline. Women with vitamin D deficiency had higher pre-pregnancy body mass index (BMI), pre-pregnancy weight, mid-pregnancy weight, weight gain, blood pressure (systolic and diastolic), HbA1c, triglyceride, fasting insulin, and HOMA-β than did those without vitamin D deficiency. There were no significant differences in age, history of GDM, family history of diabetes, parity, gestational weeks, season, FPG, total cholesterol, HDL-C, albumin, fasting C-peptide, HOMA-IR, and the results of 50-g and 100-g OGTT between women with and without vitamin D deficiency.
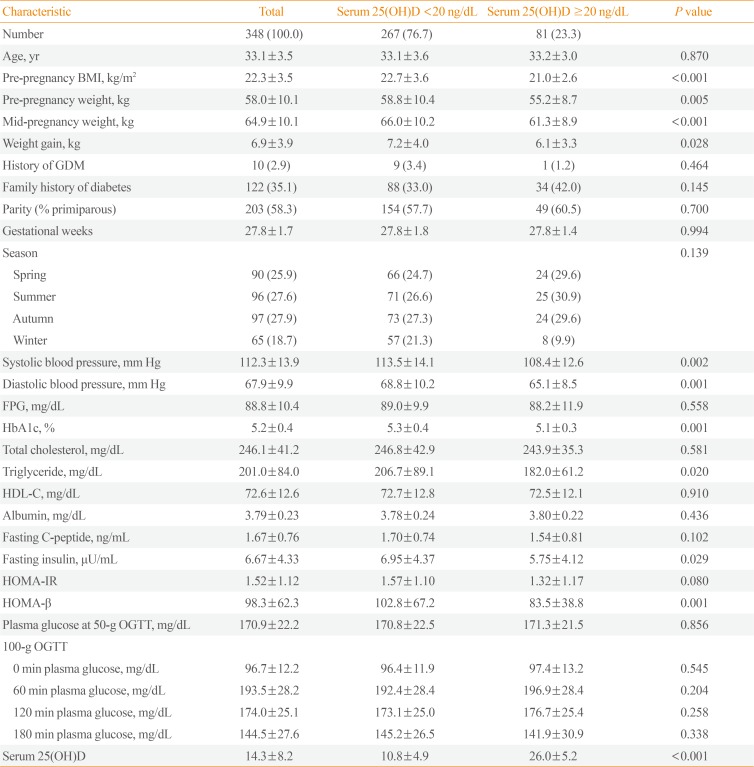
Table 1
Baseline Characteristics of Women with Gestational Diabetes Mellitus According to Serum 25(OH)D Level at Mid-Pregnancy
Values are expressed as number (%) or mean±standard deviation.
25(OH)D, 25-hydroxyvitamin D; BMI, body mass index; GDM, gestational diabetes mellitus; FPG, fasting plasma glucose; HbA1c, hemoglobin A1c; HDL-C, high density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-β, homeostasis model assessment of β-cell function; OGTT, oral glucose tolerance test.
![]()
Pregnancy outcomes such as preterm delivery, Cesarean section, and baby weight were not different regardless of vitamin D deficiency (Table 2). Women with vitamin D deficiency tended to use insulin more frequently than those without vitamin D deficiency but the difference was not statistically significant.
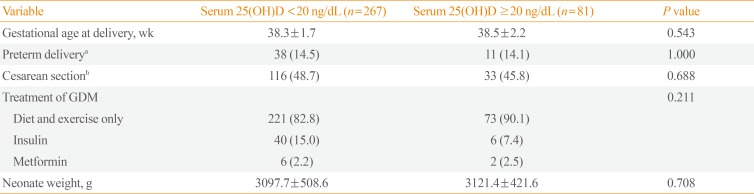
Table 2
Pregnancy Outcomes of Women with Gestational Diabetes Mellitus According to Serum 25(OH)D Level
![]()
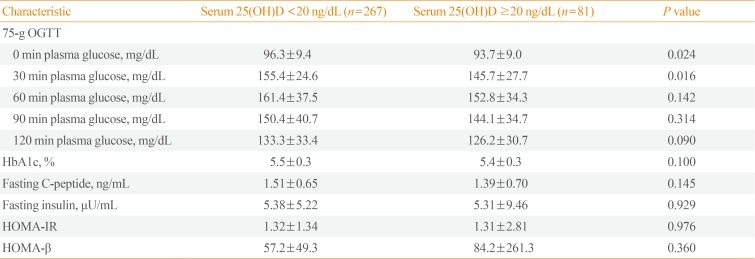
The prevalence of postpartum glucose intolerance and overt diabetes was 44.8% and 4.9%, respectively. Women with vitamin D deficiency at mid-pregnancy had a higher prevalence of postpartum glucose intolerance than did those without vitamin D deficiency (48.7% vs. 32.1%, P=0.011) (Fig. 1). After postpartum 6 to 12 weeks, 0 and 30 minutes plasma glucose levels during 75-g OGTT were higher in women with vitamin D deficiency than in those without vitamin D deficiency but 60, 90, and 120 minutes plasma glucose levels were not different (Table 3). HbA1c, fasting C-peptide, fasting insulin, HOMA-IR, and HOMA-β were not different between the two groups, although HOMA-β showed a low tendency in women with vitamin D deficiency.
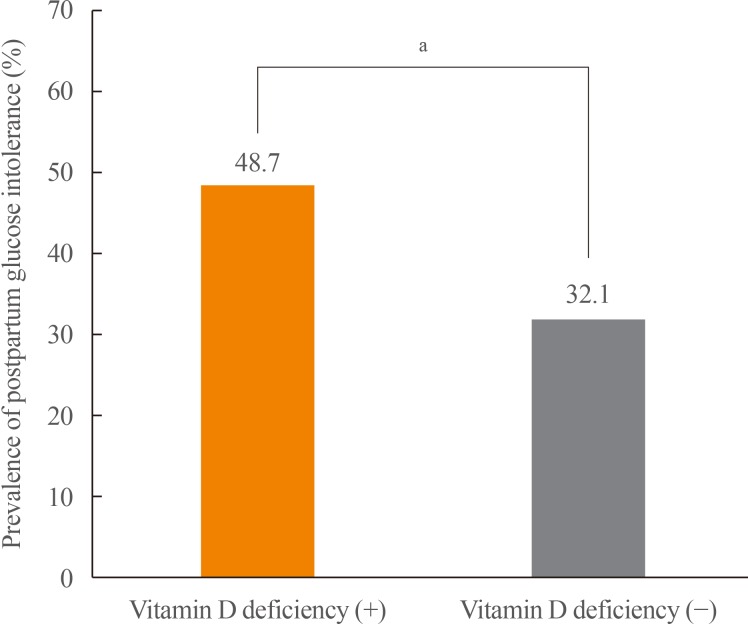 | Fig. 1Prevalence of postpartum glucose intolerance in women with gestational diabetes mellitus according to the status of serum 25-hydroxyvitamin D level. aP<0.05.
|
Table 3
Clinical Characteristics of Women with Gestational Diabetes Mellitus According to Serum 25(OH)D Level at Postpartum 6 to 12 Weeks
![]()
Serum 25(OH)D level was negatively correlated with HbA1c antepartum and postpartum after being adjusted for maternal age, pre-pregnancy BMI, weight gain, blood pressure (systolic and diastolic), family history of diabetes, and season (antepartum: r=−0.186, P=0.001; postpartum: r=−0.129, P=0.047) (Table 4). No correlation was noted between serum 25(OH)D and HOMA-IR. Interestingly, after adjustment for the aforementioned factors, HOMA-β was positively correlated with serum 25(OH)D level only postpartum (r=0.138, P=0.035).
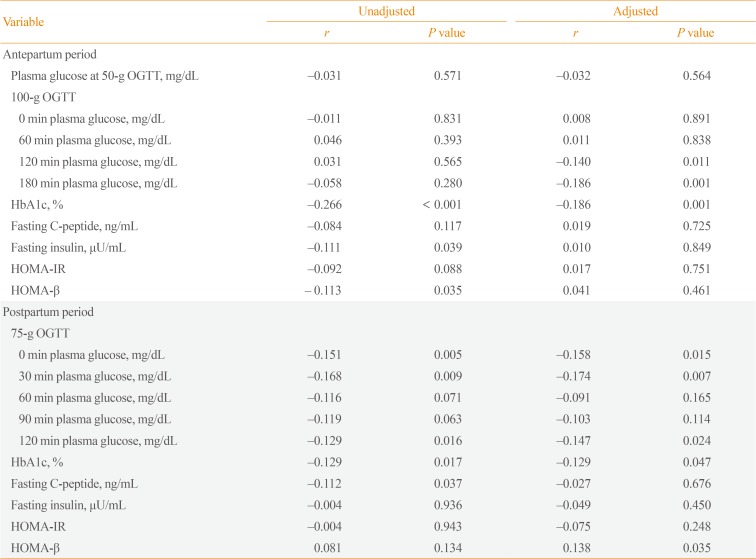
Table 4
Correlations between Serum 25-Hydroxyvitamin D Levels and Glycemic Parameters
0.035Adjusted for maternal age, pre-pregnancy body mass index, weight gain, family history of diabetes, blood pressure (systolic and diastolic), and season.
OGTT, oral glucose tolerance test; HbA1c, hemoglobin A1c; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-β, homeostasis model assessment of β-cell function.
![]()
The risk of postpartum glucose intolerance was about twofold as high in women with vitamin D deficiency (Table 5). Even after adjustment for the aforementioned factors, the risk of postpartum glucose intolerance was still 2.00 times (95% confidence interval [CI], 1.13 to 3.55) higher in women with vitamin D deficiency than in those without vitamin D deficiency (P=0.018).

Go to :
DISCUSSION
Vitamin D deficiency is common in pregnant women and is a well-known risk factor for developing GDM [171819202122]. Because women with GDM have an increased risk of conversion to type 2 diabetes over time, we should manage them carefully and appropriately after delivery. However, few studies have examined the effect of vitamin D deficiency at mid-pregnancy on postpartum glucose intolerance in women with GDM. We have found that vitamin D deficiency at mid-pregnancy is very common and is associated with an elevated risk of postpartum glucose intolerance in women with GDM.
Because many studies have shown that vitamin D deficiency has been associated with type 2 diabetes and metabolic syndrome, we could presume it might also be associated with GDM. Although there are still many conflicting results for the association between vitamin D deficiency and development of GDM [28], recent meta-analyses have reported that such an association indeed exists [29303132]. A meta-analysis of 26 studies found that vitamin D deficiency may be associated with an increased risk of GDM (odds ratio, 1.18; 95% CI, 1.01 to 1.35; P<0.001) [32]. Clinicians should focus on preventing postpartum diabetes as well as preventing GDM development, since women with previous GDM have a more than seven-fold higher risk of developing postpartum diabetes than do those without GDM [33]. Until now, there was limited data about whether vitamin D deficiency is a risk factor for postpartum glucose intolerance in women with GDM. Although our study patients were neither many nor representative of the Korean population, they still could have shown that vitamin D deficiency increased the risk of developing postpartum glucose intolerance by 2-fold in women with GDM.
Several studies have shown that vitamin D supplementation during pregnancy is effective in preventing GDM as well as improving pregnancy outcomes [3435]. Vitamin D co-supplementation with calcium or omega-3 fatty acids in women with GDM had beneficial effects on metabolic parameters such as FPG, HOMA-IR, quantitative insulin sensitivity check index, and lipid profiles [3637]. However, the effect of prenatal vitamin D supplements on postpartum glucose metabolism has rarely been studied. A study by Valizadeh et al. [38] reported that vitamin D3 (700,000 IU total) safely increased the serum 25(OH)D but had no influence in the plasma glucose level or insulin resistance at postpartum, perhaps because the treatment period was relatively short due to pregnancy. In a non-pregnant population, vitamin D3 supplementation (4,000 IU daily) for 6 months (720,000 IU total) improved insulin resistance even though there was no difference in the first 3 months [39]. To prevent postpartum glucose intolerance, vitamin D supplementation during the entire pregnancy period may be necessary. It is not conclusive yet whether vitamin D supplementation is helpful to women with GDM because there is no large randomized controlled trial.
In a normal non-pregnant individual, approximately 85% of serum 25(OH)D is bound to vitamin D binding protein (DBP), 15% is bound to albumin, only 0.03% is free [40]. During pregnancy, DBP is almost 2-fold increases between the second and third trimesters like other globulins. However, mean free 25(OH)D may be the same as or only slightly lower than in non-pregnant women despite these marked DBP changes through decreasing affinity of DBP for vitamin D [4142]. Consequently, there would be no differences of vitamin D activity for insulin resistance and insulin secretion between pregnant and non-pregnant women. Furthermore, in this study, serum albumin concentration was not different between GDM women with and without vitamin D deficiency. We could assume that albumin or other globulins were not influenced to the results of this study.
In this study, HOMA-β was positively correlated with serum 25(OH)D level only postpartum. One possible mechanism is that vitamin D has a direct effect on the performance of the β-cells of the pancreas [743], so that vitamin D might enhance insulin secretion. The other possible mechanism is that vitamin D may affect intracellular calcium regulation which plays an important role in the insulin-mediated intracellular processes of insulin-receptor tissue [324445]. Interestingly, HOMA-β at mid-pregnancy was significantly higher in women with vitamin D deficiency than those without vitamin D deficiency. This might be compensatory hypersecretion of insulin to overcome elevated insulin resistance in GDM women with vitamin D deficiency [232425]. At postpartum period, HOMA-β was not different although it was numerically low in women with vitamin D deficiency than those without vitamin D deficiency.
Some limitations need to be considered in the interpretation of our findings. First, we cannot generalize these results to other ethnic populations. In Korea, approximately 90% of women are not vitamin D sufficient [19]. Second, we did not measure serum 25(OH)D postpartum. Third, dietary vitamin D intake could not be adjusted because we had no food frequency questionnaire data. Finally, the study population was neither large nor representative of the Korean population, so large prospective studies are needed to confirm these results. This study, however, might be valuable because it evaluated the association between vitamin D status in mid-pregnancy and postpartum glucose intolerance in women with GDM.
In conclusion, vitamin D deficiency at mid-pregnancy is associated with an elevated risk of postpartum glucose intolerance in women with GDM. Consequently, we should try to figure out postpartum glucose intolerance if women with GDM have vitamin D deficiency at mid-pregnancy.
Go to :
 XML Download
XML Download