

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In this article, I would like to update a review article published in 2018 by presenting the findings of some additional studies that have been published subsequently [1].
Before 2013, there had been no nationwide studies on serum thyroid stimulating hormone (TSH) levels, free thyroxine (fT4) levels, and urinary iodine concentration (UIC) in the Korean population. Between 2013 and 2015, the Korea Centers for Disease Control and Prevention, in conjunction with the Korean Thyroid Association, conducted a project to gather and analyze nationwide data on serum TSH levels, serum fT4 levels, and UIC in the healthy Korean population as part of the Korea National Health and Nutrition Examination Survey (KNHANES) VI (2013 to 2015). The KNHANES VI was a Korean nationwide, cross-sectional study that used stratified, multistage, clustered probability sampling to select a representative sample of the civilian, non-institutionalized Korean population. Approximately 2,400 individuals were selected each year between 2013 and 2015 using stratified subsampling and underwent measurements of serum TSH, fT4, and thyroid peroxidase antibody (TPOAb). The final participants consisted of 7,061 individuals over 10 years old. UIC was measured in a spot urine sample in 6,564 individuals. All participants answered a number of detailed questions.
Go to : 
MEAN VALUES AND REFERENCE INTERVALS OF TSH AND fT4 IN THE KOREAN POPULATION
Serum TSH levels might vary according to age, sex, smoking, TPOAb positivity, genetic determinants, and the assay method [23]. Therefore, serum TSH reference intervals should be established using specimens from TPOAb-negative, ambulatory, euthyroid subjects who have no personal or family history of thyroid dysfunction, no visible goiter, and are taking no medications [4]. Serum TSH levels measured in a euthyroid reference population show a left-skewed distribution with a long tail towards the higher levels. The values become more normally distributed when they are log-transformed. It is standard practice to log-transform serum TSH levels to calculate the 95% confidence limits.
The serum mean values and reference intervals of serum TSH and fT4 were defined using 5,987 individuals based on the KNHANES VI [56]. The reference individuals were selected from TPOAb-negative (<34.0 IU/mL), ambulatory, euthyroid subjects who had no personal or family history of thyroid dysfunction, no visible goiter, and were taking no medications. The geometric mean value was defined as the nth root of the product of n numbers. The geometric mean serum TSH level was 2.16 mIU/L, and it was lower in the age group of 40 to 49 years and higher in the age groups of 10 to 19 years and 70 years or older [7]. Therefore, a U-shaped association was observed between serum TSH levels and age (Fig. 1). The mean TSH value was significantly higher in women than in men (2.24 mIU/L vs. 2.09 mIU/L, P<0.001). The reference intervals were calculated from the 95% confidence limits of the log-transformed values. The serum TSH reference interval was 0.59 to 7.03 mIU/L (women, 0.56 to 7.43 mIU/L vs. men, 0.62 to 6.57 mIU/L), which was right-shifted, but not correlated with age [8]. The mean serum fT4 level was 1.25 ng/dL, and its reference interval was 0.92 to 1.60 ng/dL. The mean fT4 level in men was significantly higher than that in women (1.29 ng/dL vs. 1.20 ng/dL, P<0.0001), and serum fT4 levels significantly decreased with age after 20 years old (P for trend <0.0001) (Fig. 1).
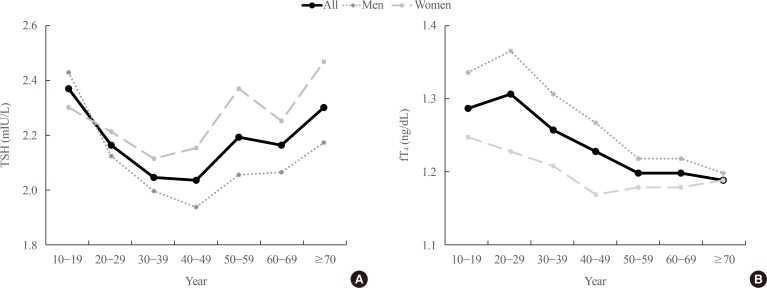 | Fig. 1Serum thyroid stimulating hormone (TSH) and free thyroxine (fT4) levels by age and sex. (A) Geometric mean TSH levels (mIU/L) by age. (B) Mean fT4 levels (ng/dL) by age. A U-shaped association was found between serum TSH levels and age. TSH levels were significantly higher in women than in men (P<0.001). Serum fT4 levels significantly decreased with age (P for trend <0.0001), and were significantly higher in men than in women (P<0.0001). Adapted from Park et al. [6].
|
A few clear differences exist between the results from Korea (KNHANES VI) and those of previously published Western reports. First, the serum TSH levels in the Korean population were markedly higher than those in Western reports. For example, the mean value and upper reference limit of serum TSH in a report from the USA (National Health and Nutrition Examination Survey [NHANES] III) were 1.40 and 4.12 mIU/L, respectively, whereas the corresponding Korean results were 2.16 and 7.03 mIU/L, respectively [2]. All Korean values were right-shifted, and these differences might be related to excessive iodine intake in the Korean population [9]. Genetic differences regarding the set-point of thyroid hormone have been proposed, and such differences might be another reason for the higher TSH levels found in Koreans [310]. Second, a U-shaped curve between age and serum TSH levels, with lower levels in middle-aged adults and higher levels in younger and older age groups, was only found in the Korean results (Fig. 2). Most studies reported that serum TSH levels gradually increased with age. However, a recent result from the Rotterdam Study reported that TSH levels remained stable with age [3]. A U-shaped curve was also found between age and UIC. Therefore, changes in serum TSH levels with age were influenced by changes in the UIC (reflecting iodine intake) in the Korean population [911].
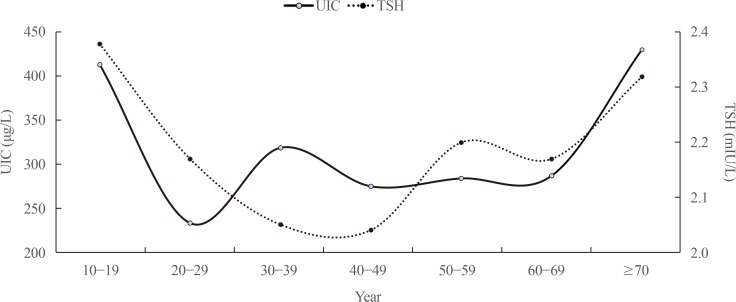 | Fig. 2Relationship of urinary iodine concentration (UIC) with serum thyroid stimulating hormone (TSH) levels. A U-shaped curve was found between age and serum TSH levels, with lower levels in middle-aged adults and higher levels in younger and older age groups. A U-shaped curve was also detected for the relationship between age and UIC. Therefore, changes in serum TSH levels with age may be influenced by changes in UIC in the Korean population. Adapted from Park et al. [6].
|
Go to :
PREVALENCE OF TPOAb IN THE KOREAN POPULATION
TPOAb positivity was defined as a level of ≥34.0 IU/mL. Serum TPOAb was detected in 7.30% of subjects (men 4.33%, women 10.62%). TPOAb titers tended to increase with age, but decreased after age 70. They were higher in women than in men (Table 1). Previous studies have generally reported that TPOAb increased TSH level, while smoking decreased it. Park et al. [12] recently evaluated the associations of smoking with TSH levels, TPOAb, and UIC using the KNHANES VI. They reported that a smoking-induced decrease in TSH levels was evident in individuals with iodine deficiency, and that the TPOAb positivity rate was high in non-smokers. Therefore, they concluded that smoking might be not associated with the presence of TPOAb or iodine intake, and that smoking may have a direct effect on thyroid function that is not mediated by autoimmune processes.
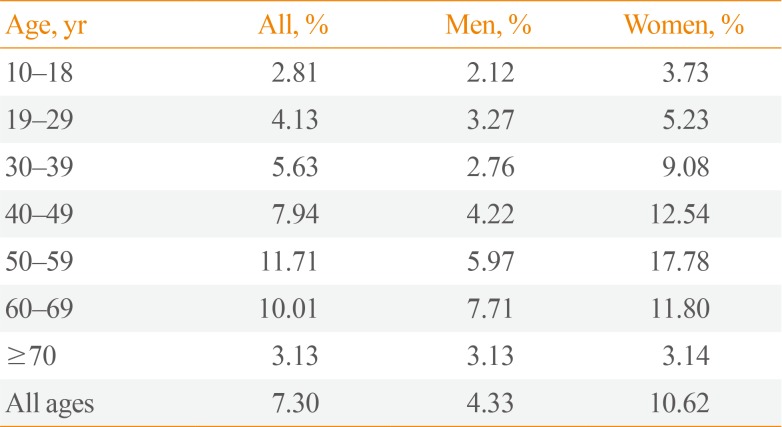
Table 1
Prevalence of TPOAb in the Korean Population According to Age and Sex
Adapted from Kim et al. [5]. TPOAb positivity was defined as >34.0 IU/mL. Serum TPOAb titers tended to increase with age, but decreased after age 70. They were higher in women than in men.
TPOAb, thyroid peroxidase antibody.
![]()
Go to :
MEAN VALUES AND REFERENCE INTERVALS OF UIC IN THE KOREAN POPULATION
Most Koreans have been reported to have sufficient iodine intake [91314]. However, no nationwide survey had investigated iodine intake in a representative sample of the entire Korean population before 2013. In non-pregnant, non-lactating women, a UIC of 100 µg/L corresponds roughly to a daily iodine intake of approximately 150 µg under steady-state conditions [1516]. Kim et al. [17] published results on the UIC in Koreans based on the KNHANES VI, which was the first nationwide report on this topic. They reported that the median UIC in the Korean population was 294 µg/L, corresponding to a level of iodine intake that is above requirements according to the World Health Organization (WHO) recommendations. The unique eating habits of Koreans, including the consumption of basic ingredients made from sea tangle or kelp and seaweed soup, are considered to be a major cause of these trends [91819]. According to the WHO recommendations, only 23% of participants were in the adequate range (UIC, 100 to 199 µg/L), and 65% were classified as having an intake that was above requirements (UIC, 200 to 299 µg/L) or excessive (UIC ≥300 µg/L). However, 12% of participants had insufficient iodine intake (UIC <100 µg/L). The median UIC was higher among school-aged children (6 to 12 years, 511 µg/L) and in those above 70 years of age than in other age groups (Fig. 3). After adjusting for age, sex, body mass index, and smoking status, serum TSH levels were significantly correlated with UIC (r=0.154, P<0.0001). The changes in UIC with age showed a U-shape (Fig. 2). The median UIC increased with household income level (P for trend <0.001). Individuals living in seaside or urban areas had higher UIC values than those in inland or rural areas. This trend is consistent with the findings of previous studies [2021]. Choi et al. [22] analyzed UIC in adolescents aged 10 to 18 years and their parents using the KNHANES VI. They reported that the prevalence of iodine deficiency exceeded 10% in several regions of Korea, and that iodine intake status in Korean adolescents was primarily affected by their families' eating habits and household income.
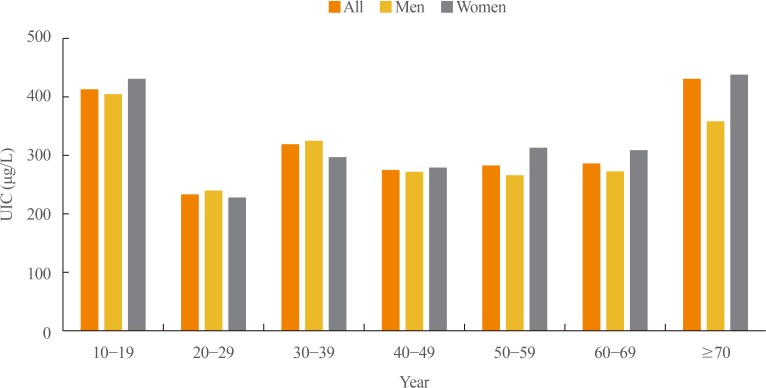 | Fig. 3Urinary iodine concentration (UIC, µg/L) by age and sex. According to the World Health Organization recommendations, only 23% of subjects were in the adequate range (UIC, 100 to 199 µg/L), and 65% were classified as having an intake that was above requirements (UIC 200 to 299 µg/L) or excessive (UIC ≥300 µg/L). However, 12% had insufficient iodine intake (UIC <100 µg/L). The median UIC was higher in school-aged children (6 to 12 years) and in the above 70 years age group than in other age groups. Adapted from Park et al. [6].
|
Go to :
PREVALENCE OF OVERT HYPERTHYROIDISM AND HYPOTHYROIDISM
Kim et al. [5] investigated the prevalence of thyroid dysfunction in the Korean population based on the KNHANES VI, and reported that the prevalence of overt and subclinical hyperthyroidism was 0.54% (men, 0.30%; women, 0.81%) and 2.98% (men, 2.43%; women, 3.59%), respectively. They also reported that the prevalence of overt and subclinical hypothyroidism (SCH) was 0.73% (men, 0.40%; women, 1.10%) and 3.10% (men, 2.26%; women, 4.04%), respectively, and its prevalence increased with age until the age group of 50 to 59 years. Seo et al. [2324] published results on the prevalence of overt hyperthy-roidism and overt hypothyroidism using National Health Insurance claims data provided by the Health Insurance Review and Assessment Service (HIRA) in 2013 and 2015, respectively. They reported that the prevalence of overt hyperthyroidism and overt hypothyroidism was 0.34% (men, 0.20%; women, 0.47%) and 1.43% (men, 0.44%; women, 2.40%), respectively. The prevalence derived from the KNHANES VI data included individuals who were not receiving treatment, but excluded well-controlled euthyroid patients with treatment, while the prevalence derived from the HIRA data may have included subclinical patients receiving overtreatment, while excluding individuals who were not receiving treatment. Therefore, these two sets of results should not be compared without adjustment. Ha et al. [25] investigated the risk factors for SCH according to sex using KNHANES VI data. They reported that TPOAb positivity significantly increased the risk of SCH in both men and women, but smoking reduced it in men. The risk of SCH increased as UIC increased, and this trend was more marked in men than in women. The odds ratio for SCH for urban (vs. rural) residence was 1.78.
When jointly evaluating these two nationwide sets of results, the prevalence of overt hyperthyroidism and overt hypothyroidism in the Korean population may be 0.34% to 0.54% (men, 0.20% to 0.30%; women, 0.47% to 0.81%) and 0.73% to 1.43% (men, 0.40% to 0.44%; women, 1.10% to 2.40%), respectively (Table 2).
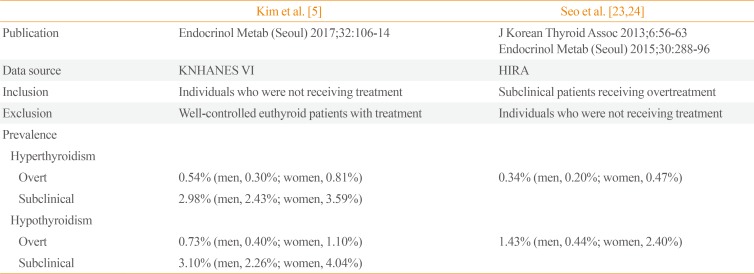
Table 2
Prevalence of Hyperthyroidism and Hypothyroidism in Korea: Comparison of KNHANES VI Data with HIRA Data
| Kim et al. [5] | Seo et al. [2324] | |
|---|---|---|
| Publication | Endocrinol Metab (Seoul) 2017;32:106-14 | J Korean Thyroid Assoc 2013;6:56-63 |
| Endocrinol Metab (Seoul) 2015;30:288-96 | ||
| Data source | KNHANES VI | HIRA |
| Inclusion | Individuals who were not receiving treatment | Subclinical patients receiving overtreatment |
| Exclusion | Well-controlled euthyroid patients with treatment | Individuals who were not receiving treatment |
| Prevalence | ||
| Hyperthyroidism | ||
| Overt | 0.54% (men, 0.30%; women, 0.81%) | 0.34% (men, 0.20%; women, 0.47%) |
| Subclinical | 2.98% (men, 2.43%; women, 3.59%) | |
| Hypothyroidism | ||
| Overt | 0.73% (men, 0.40%; women, 1.10%) | 1.43% (men, 0.44%; women, 2.40%) |
| Subclinical | 3.10% (men, 2.26%; women, 4.04%) |
![]()
Go to :
CONCLUSIONS
Based on the KNHANES VI, the mean TSH level in the Korean population was 2.16 mIU/L, and its reference interval was 0.59 to 7.03 mIU/L. A U-shaped association was found between serum TSH levels and age. Serum TSH levels were significantly higher in women than men. The mean fT4 level was 1.25 ng/dL, with a reference interval of 0.92 to 1.60 ng/dL. Serum fT4 levels significantly decreased with age, and were significantly higher in men than in women. Serum TPOAb was detected in 7.30% of subjects, a proportion that tended to increase with age. The median UIC was 294 µg/L, and a U-shaped relationship of UIC with age was evident. Only 23% of subjects had an adequate iodine intake according to the WHO criteria, and 65% were classified as having an intake that was above requirements or excessive. However, 12% had insufficient iodine intake. The prevalence of overt hyperthyroidism and overt hypothyroidism in the Korean population was 0.34% to 0.54% and 0.73% to 1.43%, respectively.
Go to :
 XML Download
XML Download