

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe fever with thrombocytopenia syndrome (SFTS) is an emerging infectious disease caused by the novel bunyavirus, called SFTS virus, which was first reported in China in 20111 and Korea and Japan in 2013.23 The virus is transmitted by ticks such as Haemaphysalis longicornis.1 The clinical manifestations of SFTS are nonspecific and include fever, myalgia, vomiting, and diarrhea. In critically ill patients, multi-organ failure may occur.4 There is no effective antiviral therapy, and the mortality ranges from 6.3% to 30%.56 Because SFTS is a disease with a rapidly progressive deterioration and high mortality rate, early diagnosis is important for survival of patients and preventing transmission of infection.67
Although the number of SFTS cases has increased steadily, with 259 patients with SFTS in 2018, other endemic zoonoses, such as scrub typhus (6,682 patients), hemorrhagic fever with renal syndrome (HFRS) (433), and leptospirosis (118) were more prevalent in Korea.8 Moreover, early clinical manifestations of SFTS are similar to those of other endemic zoonoses; therefore, SFTS needs to be differentiated from these diseases. Although the quantitative real-time reverse-transcriptase polymerase chain reaction (RT-PCR) assay is a reliable method for early diagnosis of SFTS,9 this test could not be performed by most primary care providers at local clinics.
Therefore, we aimed to derive a clinical prediction scoring system with initial symptoms and basic laboratory blood tests that could be useful for primary care providers to differentiate SFTS from other endemic zoonoses. We also evaluated the predictability of the score, reassessed 2 days after admission in patients with low probability of SFTS.
METHODS
Patients and data collection
Patients aged 18 years or older diagnosed with endemic zoonoses during the 3-year period from January 2015 to December 2017 were enrolled from 4 university hospitals in Korea: Seoul National University Bundang Hospital (1,300 beds), Boramae Medical Center (800 beds), Seoul National University Hospital (1,700 beds), and Kangwon National University Hospital (600 beds). Endemic zoonoses included SFTS, scrub typhus, HFRS, leptospirosis, Q fever, and human granulocytic anaplasmosis (HGA). All patients with a diagnosis code and/or confirmatory test results of endemic zoonoses were screened.
SFTS was confirmed by detecting the M segment gene of the viral ribonucleic acid (RNA) with RT-PCR as described in a previous study.10 Scrub typhus was diagnosed by a single titer ≥ 1:16011 or a ≥ 4-fold rise in indirect immunofluorescent assay (IFA) titer in paired serum samples. HFRS was diagnosed by a single titer ≥ 1:80, ≥ 4-fold rise in IFA titer in paired serum samples, or positive RT-PCR test. Considering the incidence and importance of these endemic zoonoses in Korea, we included only the patients with all three of the above results in this study. Leptospirosis was diagnosed by ≥ 4-fold rise in IFA titer in paired serum samples or an antibody titer ≥ 1:800 in one serum sample by the microscopic agglutination test. Q fever was diagnosed by ≥ 4-fold rise an antiphase II antigen immunoglobulin G titer in paired serum samples. HGA was diagnosed by ≥ 4-fold rise in IFA titer in paired serum samples or positive PCR test. We excluded patients with bacteremia or co-infections between endemic zoonoses.
We retrospectively reviewed the demographic and clinical data of the patients, including age, gender, occupation, comorbidities, presence of symptoms, and laboratory findings, to analyze the differentiating factors between SFTS and other endemic zoonoses.
Neurologic symptoms included altered mentality, for which Glasgow coma scale score is < 15, and tremor, motor weakness, and dysarthria, which were based on the information in the physician or nurse's medical records. Diarrhea was defined as three or more unformed stools per day, and we also considered that diarrhea was present when the attending physician described diarrhea symptoms in the patient's medical record. Leukopenia was defined as white blood cell count < 4,000/mm3. Thrombocytopenia was defined as blood platelet count < 150 × 103/mm3. Normal C-reactive protein (CRP) was defined as < 0.5 mg/dL.
Statistical analysis
Categorical variables were compared using χ2 or Fisher's exact tests, and continuous variables were compared using t-test or Mann-Whitney U test. Multivariate logistic regression analysis was performed using the significant differentiating factors (P < 0.05) between SFTS and other endemic zoonoses in univariate analysis and adjusted for the duration from the onset of illness to the initial presentation. We excluded some variables that could be influenced by recall bias or had insufficient description (e.g., insect bite wound) from the multivariate analysis. For possible overlapping variables (e.g., anemia and bleeding), we constructed separate models. Variables without all patients' data were excluded from multivariate regression model. The prediction score for SFTS was built based on the final multivariate regression model. The receiver operating characteristic (ROC) curve was constructed for scoring model. Statistical analyses were performed using SPSS for Windows (version 18 software package; SPSS, Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Bundang Hospital (B-1801/445-112), which waived the need to obtain informed consent from the patients. All the other institutions participating in this study also obtained approvals from their IRBs. All clinical investigations were conducted according to the principles expressed in the Declaration of Helsinki.
RESULTS
A total of 202 patients were diagnosed with endemic zoonoses clinically and/or by laboratory tests during the 3-year period including 49 patients with SFTS, 132 with scrub typhus, 18 with HFRS, 2 with Q fever, and 1 with leptospirosis. Of these, 118 patients (without the test results for the following three, SFTS, scrub typhus, and HFRS, or with other bacterial infection) were excluded. Finally, 84 patients including 35 with SFTS and 49 with other endemic zoonoses (40 scrub typhus and 9 HFRS) were enrolled in this study (Supplementary Fig. 1). None of the patients clinically diagnosed with leptospirosis, Q fever, or HGA met the enrollment criteria. Patients' demographic and clinical characteristics are described in Table 1. At the initial presentation, diarrhea and neurologic symptoms were more common in SFTS patients than in other endemic zoonoses patients. In the laboratory findings, the elevation of aspartate aminotransferase (AST), creatinine kinase, and ferritin were also more common in SFTS patients than in others. White blood cell (WBC), CRP, and procalcitonin were rarely elevated in SFTS. In addition, on comparing the three diseases, younger men were more common in the HFRS group, and no rash was observed. Diarrhea, neurologic symptoms, and normal CRP were more common in the SFTS group (Supplementary Table 1).
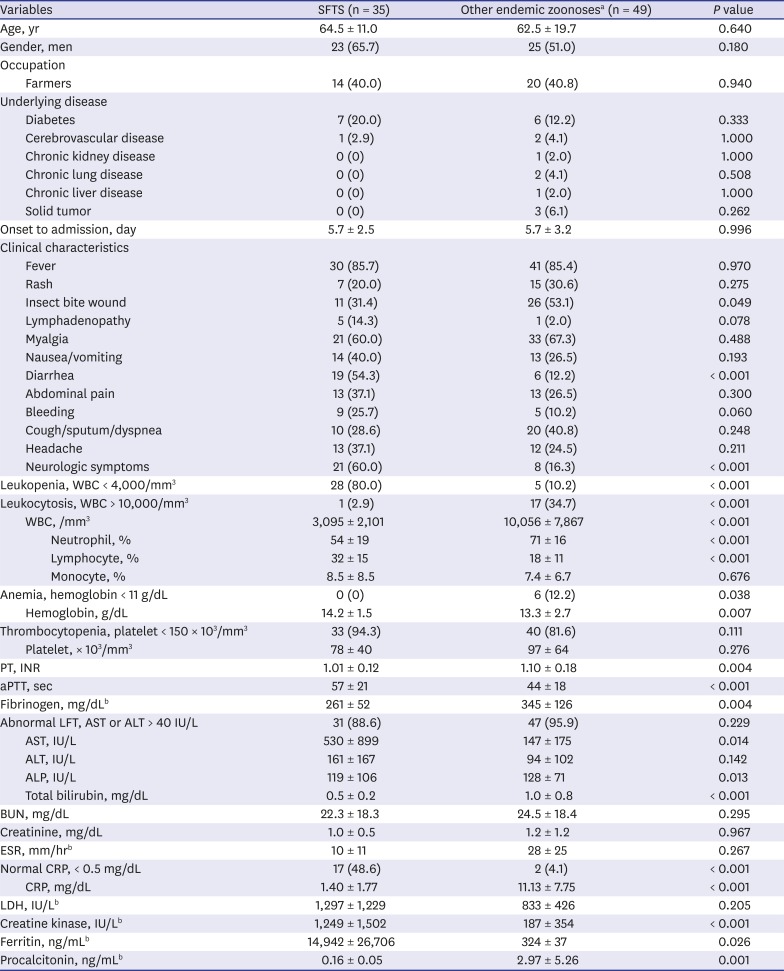
Table 1
Comparison of patients' baseline clinical characteristics and laboratory results between SFTS and other endemic zoonoses
Data are presented as mean ± standard deviation or number (%).
SFTS = severe fever with thrombocytopenia syndrome, WBC = white blood cell, PT = prothrombin time, INR = international normalized ratio, aPTT = activated partial thromboplastin time, LFT = liver function test, AST = aspartate aminotransferase, ALT = alanine aminotransferase, IU =international unit, ALP = alkaline phosphatase, BUN =blood urea nitrogen, ESR =erythrocyte sedimentation rate, CRP = C-reactive protein, LDH = lactate dehydrogenase.
aNumber of patients with other endemic zoonoses: scrub typhus 40, hemorrhagic fever with renal syndrome 9; bNumber of patients with the biomarkers results: Fibrinogen (SFTS 19, other endemic zoonoses 20), ESR (SFTS 2, other endemic zoonoses 4), LDH (SFTS 28, other endemic zoonoses 32), Creatinine kinase (SFTS 34, other endemic zoonoses 42), Ferritin (SFTS 11, other endemic zoonoses 2), and Procalcitonin (SFTS 4, other endemic zoonoses 11).
![]()
In the multivariate logistic regression analysis, neurologic symptoms, diarrhea, leukopenia, and normal CRP were significantly associated with SFTS rather than with other endemic zoonoses (Table 2).
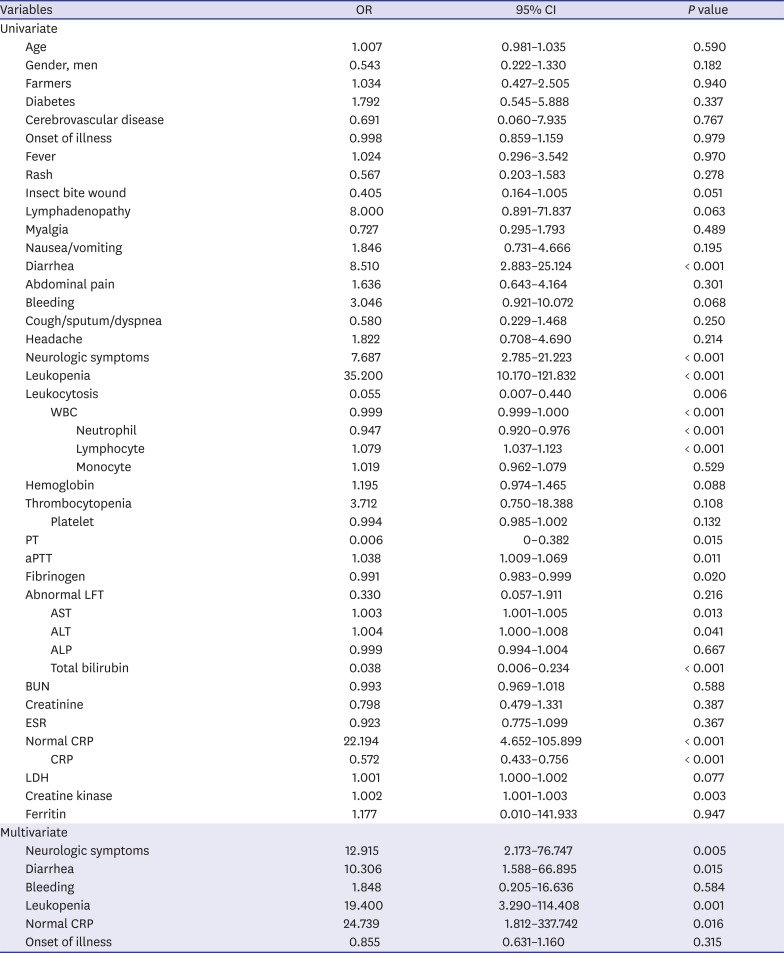
Table 2
Results of univariate and multivariate logistic regression analyses of the clinical and laboratory factors associated with SFTS
SFTS = severe fever with thrombocytopenia syndrome, OR = odds ratio, CI = confidence interval, WBC = white blood cell, PT = prothrombin time, aPTT = activated partial thromboplastin time, LFT = liver function test, AST = aspartate aminotransferase, ALT = alanine aminotransferase, ALP = alkaline phosphatase, BUN = blood urea nitrogen, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, LDH = lactate dehydrogenase.
![]()
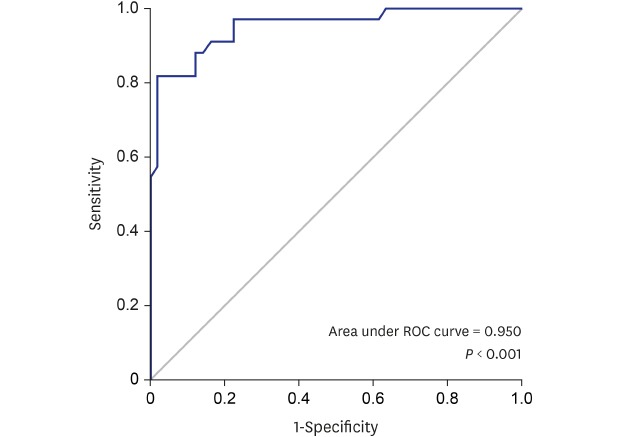
A prediction score for SFTS in comparison with other endemic zoonoses was generated using the combination of those 4 parameters (using 1 point each for neurologic symptoms, diarrhea, leukopenia, and normal CRP) and the total sum ranged from 0 to 4. On the ROC curve obtained for the model, the optimal cut-off was ≥ 2 points. A score of ≥ 2 had 82.9% sensitivity (95% confidence interval [CI], 71.7%–87.5%) and 95.9% specificity (95% CI, 88.0%–99.2%) for SFTS with ROC area under the curve of 0.950 (95% CI, 0.903–0.997) (Table 3 and Fig. 1).
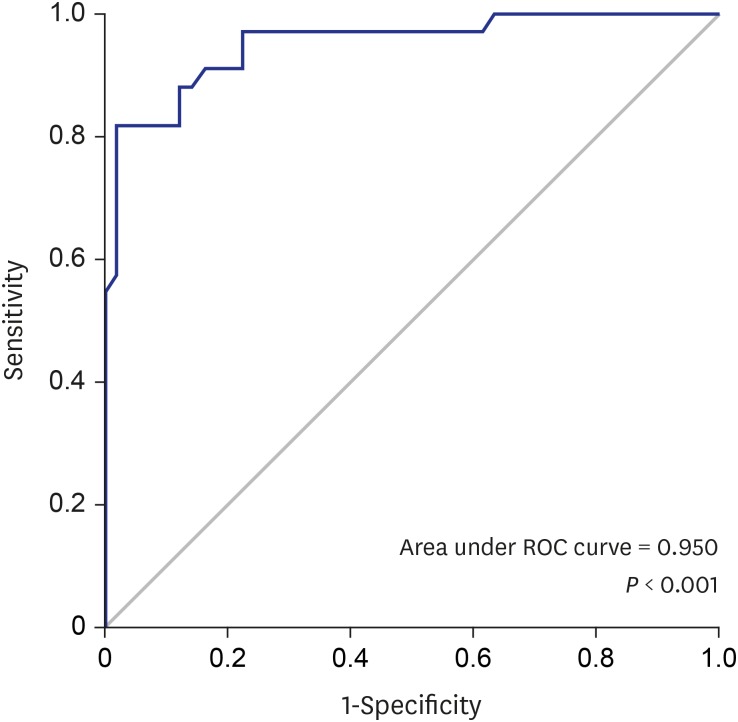

Fig. 1
ROC curve of the clinical prediction score for SFTS in patients with endemic zoonoses.
ROC = receiver operating characteristic, SFTS = severe fever with thrombocytopenia syndrome.
![]()
Table 3
Diagnostic performance of the SFTS prediction score systema
SFTS = severe fever with thrombocytopenia syndrome, CI = confidence interval, PPV = positive predictive value, NPV = negative predictive value, LR+ = positive likelihood ratio, LR− = negative likelihood ratio, NA = not available.
aPrediction score system = (1 × neurologic symptoms) + (1 × diarrhea) + (1 ×leukopenia) + (1 × normal CRP).
![]()
When we applied this prediction score according to the cut-off ≥ 2, 29 patients had SFTS and 2 patients had other endemic zoonoses (Supplementary Fig. 1). Among 53 patients with a prediction score of 0 or 1, 27 patients had clinical data on the 4 parameters 2 days after admission. Of the 22 patients with other endemic zoonoses and a score of 0 or 1, only 4 patients had diarrhea, and none had neurologic symptoms, leukopenia, or normal CRP. A score ≥ 2 had 100.0% positive predictive value (95% CI, 55.0%–100.0%) (Supplementary Table 2).
DISCUSSION
The present study identified the predictors of SFTS and suggested a clinical scoring system to distinguish SFTS patients from patients with other endemic zoonoses. This system consists of easily applicable clinical parameters, including neurologic symptoms, diarrhea, leukopenia, and normal CRP. This scoring system would be useful for early differentiation of SFTS from other endemic zoonoses.
SFTS is already an endemic disease in Korea. Han et al.12 reported an SFTS virus seroprevalence of 4.1% among residents of rural areas in Korea. Most SFTS cases occur from April to November in Korea.6 Scrub typhus and HFRS are common zoonotic diseases in Korea, and are prevalent during autumn. Most of the scrub typhus cases occur between October and November.13 Similarly, HFRS predominantly occurs during the last quarter of the calendar year.14 It is important to differentiate between SFTS and these endemic zoonoses because of their overlapping epidemic seasons.
Recently, two studies addressing the differentiation of SFTS from scrub typhus were published.1516 In particular, Park et al.16 proposed a prediction scoring tool to differentiate SFTS from eschar- or skin rash- negative scrub typhus, as it involves diagnostic uncertainty. Furthermore, there has been a report of the usefulness of ferritin as a diagnostic marker to distinguish between SFTS and bacteremia with thrombocytopenia.17 However, there was no previous study that has differentiated SFTS from other endemic zoonoses in Korea.
Our clinical score system to predict SFTS used four variables (neurologic symptoms, diarrhea, leukopenia, and normal CRP), which could easily be available in the primary care settings. Although no specific therapy is available for SFTS, and symptomatic and supportive care is the mainstay of treatment,5 several rescue therapies such as ribavirin and plasma exchange18 or intravenous immunoglobulin and corticosteroid19 may be effective in treating rapidly progressive SFTS. Our clinical score system could help clinicians to stratify the patients so that they can decide on whether to try these therapies or make an early referral, particularly in primary care settings.16
However, SFTS can spread via human-to-human transmission through blood contact, unlike other endemic zoonoses including scrub typhus.20 Kim et al.21 reported in Korea that of the 27 healthcare workers who had contact with a severely ill SFTS patient, the 4 who were involved in cardiopulmonary resuscitation were diagnosed with SFTS via seroconversion. Using our clinical score system could facilitate early referral of patients suspected of having SFTS to the tertiary hospital, with possible consideration of nosocomial transmission of SFTS, pending the availability of the confirmatory test result.
This study has several limitations. First, although this study included endemic zoonoses in Korea other than scrub typhus or HFRS, such as leptospirosis, Q fever, or HGA, no patient with these diseases met the enrollment criteria. We included 6 HFRS patients diagnosed with a single high titer. However, incorrect diagnosis was not probable as these patients not only had positive serologic results but also had clinical manifestations and an exposure history relevant to HFRS. Second, there have been recent reports of co-infection of SFTS with other zoonoses.2223 The patients with all three (SFTS, scrub typhus, and HFRS) test results were enrolled; thus, it is likely that co-infected cases occurred among those patients that were excluded from this study. We also excluded bacteremia from this study, but some types of bacteremia may be associated with endemic zoonoses. Although we excluded such co-infections to develop a clear predictive scoring system, further study is needed to determine how to distinguish co-infected cases from others. Third, the comparative group did not contain a homogenous population. However, clinicians need a prediction tool to differentiate severe disease among heterogenous populations, and the results of this study confirm the unique clinical findings of SFTS, which may be useful for primary care providers. Finally, we planned to re-evaluate for the likelihood of SFTS 2 days after admission in patients with low predictive scores at the time of admission. However, we could only apply the prediction score 2 days after admission in 27 patients; this was due to the lack of clinical information. Thus, we could not reach a conclusion from this study. Prospective validation study of this prediction score at the time of admission and a study to evaluate the usefulness of early reassessment for SFTS are warranted.
In summary, our study suggests a simple and useful scoring system to predict SFTS in patients suspected of having endemic zoonoses in Korea. We expect that this strategic approach would be helpful for primary care providers in early differentiation of SFTS from other endemic zoonoses and for improving the clinical outcomes in patients with SFTS.
 XML Download
XML Download