

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Reflex and spontaneous movements are not uncommon during the process of determining brain death. The frequency of such movements ranges from 19.2%–75% among all brain dead cases but the reported frequencies widely vary from one study to another.123456 Recently, organ donations from brain dead patients have become common and thus knowledge about such movements is necessary for accurate diagnoses of brain death. Sufficient evidence on how many brain dead patients exhibit reflex or spontaneous movements and whether there are differences in the incidence of these movements according to cause of brain death will aid physicians in correctly diagnosing brain death. Although many studies have investigated the body movements of patients with suspected brain death, few have applied verified tools and neurological tests as a standard protocol for diagnosis.345 In Korea, only a single prospective study of 26 adult brain dead patients at a single tertiary medical center was published in 2006.5 Further studies will enhance the current awareness of these movements and might prevent delays and misinterpretations associated with brain death diagnoses. Therefore, the present study assessed 436 brain dead patients in Korea to determine the frequency, characteristics, and factors associated with the presence of reflex and spontaneous movements.
Go to : 
METHODS
Study design
Brain dead patients who were admitted to 15 hospitals in the Yeongnam region (Southeast) of Korea were recruited prospectively from January 2013 to September 2016 (Fig. 1). Brain death was confirmed by a trained and experienced neurologist, neurosurgeon, or pediatric neurologist according to the guidelines of the Korea Medical Association.7 When a physician was making a brain death diagnosis, the organ procurement team (Korea Organ Donation Agency [KODA]) attended the examination and evaluated the patient for reflex and spontaneous movements. If such movements were observed during diagnosis, the patient was enrolled in the present study. All patients included in this study were diagnosed with brain death and completed the organ donation.
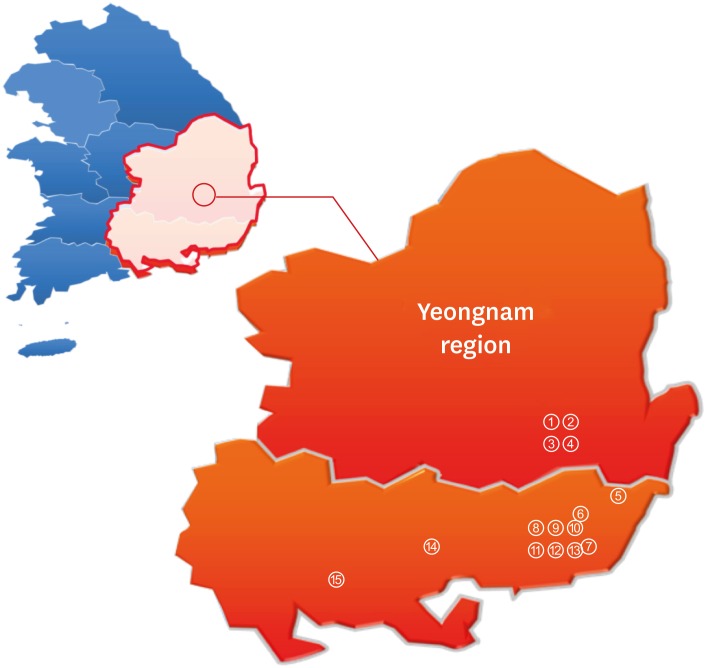 | Fig. 1Yeongnam (Southeast) region and location of the 15 hospitals in Korea. ① Keimyung University Dongsan Medical Center, ② Kyungpook National University Hospital, ③ Yeungnam University Medical Center, ④ Daegu Catholic University Medical Center, ⑤ Ulsan University Hospital, ⑥ Pusan National University Yangsan Hospital, ⑦ Inje University Haeundae Paik Hospital, ⑧ Pusan National University Hospital, ⑨ Kosin University Gospel Hospital, ⑩ Inje University Busan Paik Hospital, ⑪ Bong Seng Memorial Hospital, ⑫ Dong-A University Hospital, ⑬ Changwon Fatima Hospital, ⑭ Samsung Changwon Hospital, ⑮ Gyeongsang National University Hospital.
|
Brain death diagnosis and movement provocation protocol
Brain death was determined based on the following guidelines of the Korea Medical Association7: complete clinical neurological examination including documentation of coma, the absence of brainstem reflexes, and apnea; exclusion of hypothermia, drug intoxication, and other metabolic causes of coma; and demonstration of electrical inactivity by electroencephalography (EEG) performed after the second examination. The following protocol was performed to provoke movements: painful stimuli applied to the supraorbital area, sternum, and nail beds of the four limbs; neck flexion; tactile stimulation of the palmar and plantar areas; and an apnea test.348 If any movement repeatedly appeared during the process of diagnosis, medical staff members recorded it on video.
Video analyses
Two neurologists described and classified patients' movements by observing video recordings based on previous analyses of known movements.6910 Movement was categorized into three groups: reflex movement, which was stimulus-induced only; spontaneous movement, which was present without provocation; and both. The number of movement patterns and the areas where the movements appeared were identified for each patient and categorized as head, neck, body, arm, and leg. Subsequently, the frequency of the movements in the area where they appeared were described.
Analyses of movements without video
A total of 21 cases that lacked video recordings were analyzed based on the physicians' medical records for brain death.
Statistical analyses
SPSS software (version 25.0 for Windows; SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Demographic and clinical characteristics including cause of brain death, hemodynamic parameters, arterial blood gas concentrations, and various medical conditions were compared between the groups. To compare the demographic and characteristic data between the groups, categorical variables were assessed using χ2 tests and continuous variables were assessed using Student’s t-tests; P values < 0.05 were considered to indicate statistical significance. Forward analyses were applied to significant variables (P < 0.05), which were then included in a multiple logistic regression model that controlled for simultaneous interaction factors to generate odds ratios (ORs) and 95% confidence intervals (CIs).
Ethics statement
The study was approved by the Institutional Review Board (IRB) of Gyeongsang National University Hospital (2016-12-018). As the study was a postmortem analysis of data on brain-dead patients, the IRB waived the need for informed consent.
Go to :
RESULTS
During the study period, 436 adult patients met the criteria for brain death. The demographic and clinical characteristics of the enrolled patients are summarized in Table 1.
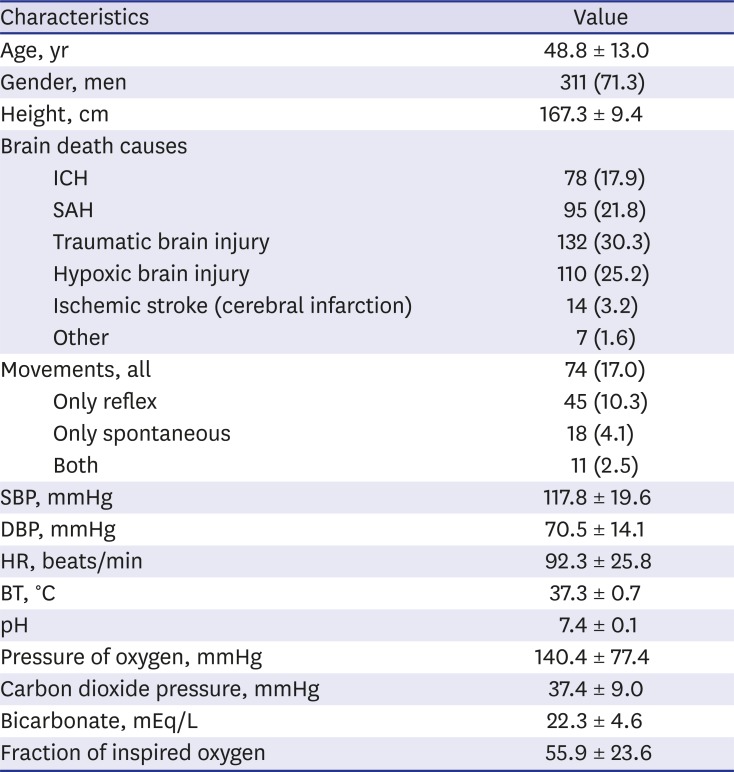
Table 1
Demographics and clinical characteristics of the 436 patients with impending brain death
Data are presented as mean ± standard deviation or number (%).
ICH = intracerebral hemorrhage, SAH = subarachnoid hemorrhage, SBP = systolic blood pressure, DBP = diastolic blood pressure, HR = heart rate, BT = body temperature.
![]()
Causes of brain death
Of the 436 patients enrolled, 132 (30.3%) had traumatic brain injury, 110 (25.2%) had hypoxic brain injury, 95 (21.8%) had subarachnoid hemorrhage, 78 (17.9%) had intracerebral hemorrhage, 14 (3.2%) had ischemic stroke, and 7 (1.6%) had other causes of brain death, including brain tumor, arteriovenous malformation, encephalopathy, and osmotic myelinolysis (Fig. 2). Of the 74 (17.0%) patients who exhibited reflex or spontaneous movements, the causes of brain death were as follows: 30 (40.5%) had hypoxic brain injury, 23 (31.1%) had traumatic brain injury, 12 (16.2%) had intracerebral hemorrhage, 8 (10.8%) had subarachnoid hemorrhage, and 1 (1.4%) had ischemic stroke. The causes of brain death in the 362 patients who did not exhibit movement were somewhat consistent with the distribution of the causes of brain death for all patients (Fig. 2). However, hypoxic brain injury was more likely to be the cause of brain death among patients with movement than those without movement (univariate analyses, P = 0.001; multivariate analyses, P = 0.001) (Fig. 2, Tables 2 and 3).

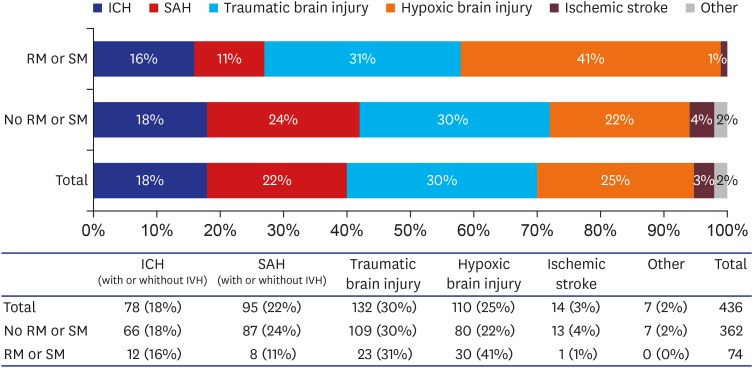 | Fig. 2Causes of brain death across all patients and with or without movement. Other etiologies include brain tumor, arteriovenous malformation, encephalopathy, osmotic myelinolysis.RM = reflex movement, SM = spontaneous movement, ICH = intracerebral hemorrhage, SAH = subarachnoid hemorrhage.
|
Table 2
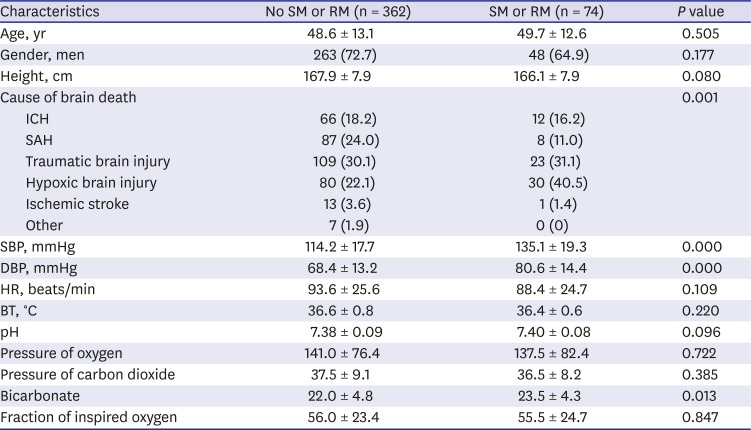
Univariate analyses of reflex or spontaneous movements during the diagnosis of brain death
Data are presented as mean ± standard deviation or number (%).
RM = reflex movement, SM = spontaneous movement, ICH = intracerebral hemorrhage, SAH = subarachnoid hemorrhage, SBP = systolic blood pressure, DBP = diastolic blood pressure, HR = heart rate, BT = body temperature.
![]()
Table 3
Logistic regression analyses of reflex or spontaneous movements during the diagnosis of brain death
| Characteristics | OR | 95% CI | P value |
|---|---|---|---|
| Age | 1.022 | 0.997–1.047 | 0.085 |
| Hypoxic brain damage | 2.928 | 1.560–5.496 | 0.001 |
| SBP | 1.050 | 1.028–1.072 | 0.000 |
| DBP | 1.018 | 0.991–1.046 | 0.200 |
| Bicarbonate | 1.059 | 0.994–1.128 | 0.076 |
OR = odds ratio, CI = confidence interval, SBP = systolic blood pressure, DBP = diastolic blood pressure.
![]()
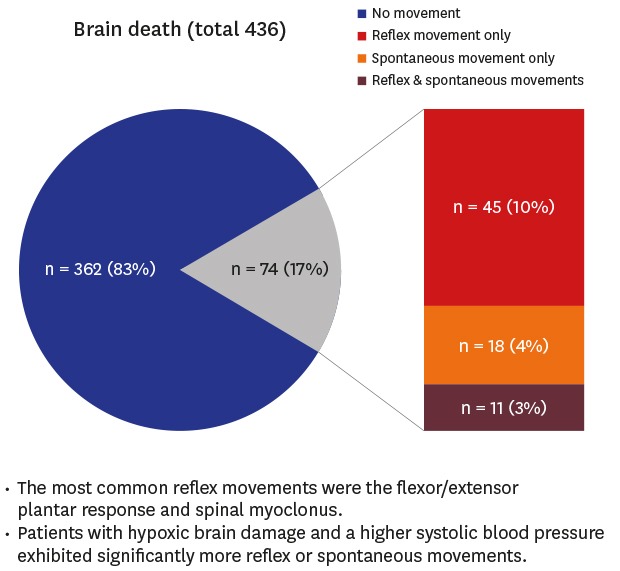
Reflex and spontaneous movements
Of the 436 brain dead patients, 74 (17.0%) exhibited reflex or spontaneous movements. Of these, 45 (60.8%) exhibited reflex movements only, 18 (24.3%) exhibited spontaneous movements only, and 11 (14.9%) exhibited both. Of the same 74 patients, 53 (71.6%) were analyzed by video recordings and 21 (28.4%) did not have video recordings and were analyzed based on physicians' medical records. In addition, 52 (70.3%) patients exhibited one movement of the same pattern and 22 (29.7%) exhibited two or more different movement patterns; a total of 106 movements were observed in the 74 patients. The frequencies and characteristics of the movements are summarized in Table 4. The most common reflex movement (n = 30, 28.3%) was the flexor/extensor plantar response. Of the 74 patients, 45 (60.8%) exhibited movements only in a limited area of the body with the leg being the most common (n = 26, 57.8%) whereas 29 (39.2%) exhibited these movements in multiple areas.
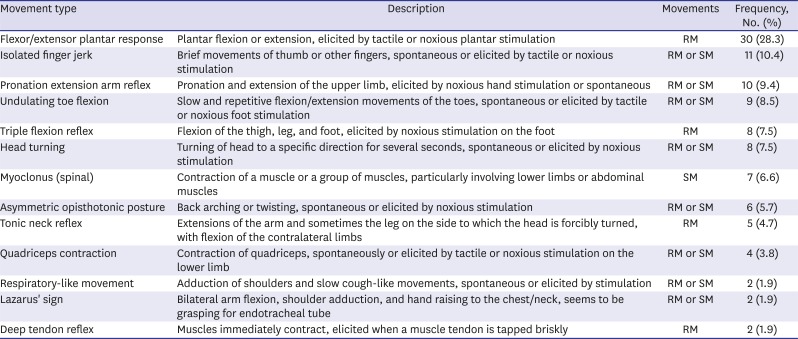
Table 4
Frequencies and descriptions of common reflex or spontaneous movements in patients during the process of determining brain death
![]()
Comparisons of the demographic and clinical characteristics
Univariate analyses revealed that systolic blood pressure (SBP), diastolic blood pressure, and bicarbonate levels and cause of brain death were significantly higher in patients with reflex and spontaneous movements (Table 2). Subsequently, multivariate analyses revealed that hypoxic brain damage and a higher SBP were significantly associated with developing reflex and/or spontaneous movements (Table 3). There were no significant differences in terms of age, gender, heart rate, body temperature, blood pH, oxygen and carbon dioxide pressure levels, fraction of inspired oxygen or height.
Go to :
DISCUSSION
Reflex and spontaneous movements associated with brain death have been evaluated in more than 130 studies of various designs ranging from animal studies to cohort studies.10 However, only a few have employed verified neurological examination and laboratory tests as a standard protocol when diagnosing brain death.3456 The frequencies of reflex and spontaneous movements differ widely among studies and the most commonly reported movements vary as well. In Korea, a single prospective study of 26 adult patients at a single tertiary medical center in 2006 has been published.5 To the best of our knowledge, the present study included the largest sample of cases that has been used to investigate movements in brain dead patients.
We defined movements induced by stimulation as reflex movements, whereas self-appearing movements in the absence of stimulation were defined as spontaneous movements. These terms are clinically useful because all movements associated with brain death are divided into these two categories.9 Except for anecdotal reports, it was possible to confirm the frequency results of two initial retrospective studies published in 1973 that investigated these movements.12 Ivan1 reported that reflex or spontaneous movements were present in 39 of 54 brain dead patients (72.2%) and Jorgensen2 observed these movements in 50 of 63 such patients (79.4%). Both studies found the frequency of such movements to be more than 70%, which is higher than the rates reported by recent studies. These two initial studies had some limitations in that the enrolled patients had not been diagnosed according to the brain death criteria of the American Academy of Neurology (AAN) and the protocols that elicited these movements were not standardized. Subsequently, Dösemeci et al.3 and Saposnik et al.4 reported that reflex or spontaneous movements were present in 18 of 134 (13.4%) and 47 of 107 brain dead patients (43.9%), respectively. These studies were prospective, met the AAN criteria for brain death, and performed standardized protocols to elicit movements. Most recently, Hosseini et al.6 reported reflex or spontaneous movements in 40 of 122 (32.8%) brain dead patients in a 1-year cross-sectional study conducted in a single organ procurement unit. The frequency of movements observed in these studies ranged from 13.4% to 43.9%, which is highly variable. In 2006, a total of 26 adult brain dead patients at a single Korean tertiary medical center were enrolled in a study.5 Five (19.2%) exhibited reflex or spontaneous body movements during the process of determining brain death. Our results are in line with their reported frequency.
The most frequent movements or common movements are mentioned as important outcomes in previous reports but differ from study to study.123456 In the present study, the most common movement was flexor/extensor plantar response (Table 4), which is consistent with the findings of Hosseini et al.6 Eleven (14.9%) patients exhibited both reflex and spontaneous movements and 25 (33.8%) patients exhibited more than two movement patterns in each patient. The greatest number of accompanied movement patterns are 4. Also, 29 (39.2%) patients exhibited these movements on multiple body areas. These results suggest that reflex and spontaneous movements can appear together in a single patient, and either a single or various movement patterns can occur on several body parts. Han et al.5 conducted the only previous study on this topic in Korea. They observed these movements in 19.2% of their patients, a similar rate to our findings (17.0%). However, the most common movement and distribution of brain death etiology differed between their study and ours. Han et al.5 reported that the most common movement was a pronation-extension reflex. In addition, there were no identified factors that were associated with these movements.
In 2005, Saposnik et al.4 reported that reflex and spontaneous movements were significantly more common when the cause of brain death was focal lesions and that brain dead patients had a high average BP. In addition, Hosseini et al.6 reported that the mean SBP was significantly higher in a group of brain dead patients that exhibited movement. We found that brain death was more frequent in patients with hypoxic brain damage than in those who sustained focal lesions, contrary to the findings of Saposnik et al.4 That study included 107 brain dead patients but only 9 had suffered from hypoxic brain injury and thus it was likely difficult to perform statistical analyses. In contrast to Saposnik et al.,4 we included 436 brain dead patients and 110 (25.2%) had hypoxic brain injury. Of these patients, 80 of 362 (22.0%) patients who did not exhibit movement and 30 of 74 (40.5%) who did exhibit movement had hypoxic brain injury. Although multivariate analyses revealed significant differences between these groups (OR, 2.928; 95% CI, 1.560–5.496; P = 0.001) (Table 3), it would be difficult to explain why patients with hypoxic brain injury were more likely to display movements than those with focal brain injuries. Likewise, Saposnik et al.4 could not provide an explanation regarding why there were more movements in brain dead patients with a focal injury.
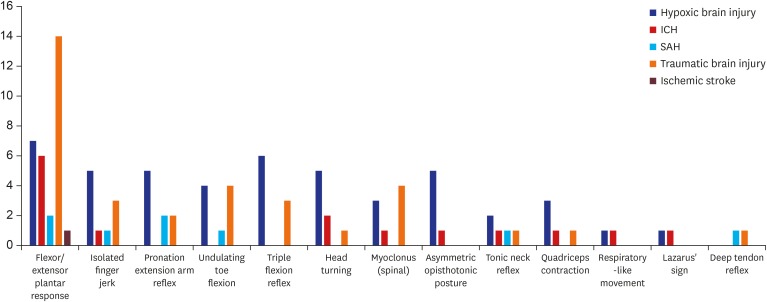
A previous study suggested that different types of myoclonus can be observed in the posthypoxic state.11 We examined whether the significantly higher occurrence of these movements in hypoxic brain injury was associated with posthypoxic myoclonus. Of the 436 brain-dead patients, 110 had hypoxic brain injury. Of these, 30 had reflex or spontaneous movements. We examined the detailed reflex or spontaneous movements of the hypoxic brain injury patients. Myoclonus was observed only in three patients (two spinal myoclonus, one abdominal reflex). The most common movement found was flexor/extensor plantar response, not myoclonus, followed by a triple flexion reflex. The proportion of patients who had myoclonus was relatively small among hypoxic brain injury patients compared with other etiologies of brain death. In addition, myoclonus was observed in 8 of 74 patients with reflex or spontaneous movements and myoclonus appeared more often in patients with traumatic brain injury than in those with hypoxic brain injury (Fig. 3).
In conclusion, we analyzed reflex and spontaneous movements using a large sample of brain dead patients in Korea and found that 17.0% of patients exhibited these movements during the process of brain death diagnosis; the observed frequency is lower than that reported by previous studies. The occurrence of reflex and spontaneous movements in brain dead patients is not rare but previous studies of this phenomenon that employed relatively similar designs showed different results. In the present study, the flexor/extensor plantar response and isolated finger jerks were the most common movements and more movements were observed in patients with hypoxic brain injury and a higher SBP. If medical staff have sufficient knowledge of the frequency and patterns of these movements in patients with impending brain death, they may be better able to reduce delays in the diagnosis of brain death.
Go to :
 XML Download
XML Download