

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Long-term survival outcomes following liver transplantation (LT) have improved, however hepatocellular carcinoma (HCC) recurrence and development of de novo malignancy (DNM) become the major causes of late recipient death.1 Because the majority of patients with posttransplant HCC recurrence have died due to disease progression, special attention has been paid to surveillance of HCC recurrence as well as prudent pretransplant selection of LT candidates.234 However, surveillance for DNM has not been considered as a serious matter of concern.
Immunosuppressive therapy for a long period has been reported to increase the risk of DNM, with these cancers also being one of the leading causes of late mortality after LT.56 Development of posttransplant DNM has been ascribed to a multifactorial combination of individual and regional predispositions to malignancy, pretransplant disease states, types of immunosuppressive agents, and time elapsed after LT.
Because the number of LT cases was much higher in Western countries than in Asian countries, most studies regarding DNM after LT have been performed in Western countries.78910 Consequently, the epidemiologic features in Western countries must be reflected in the incidence of DNM. In contrast, the epidemiologic features in Asian countries must be different from those of Western countries. Therefore, the analysis on the features of DNM in Korea should be based on Korean data.111213
In Korea, a half of adult patients undergoing LT, particularly living donor liver transplantation (LDLT), had been diagnosed as having HCC before LT operation. This unique feature raised a question whether precedent hepatic malignancy can increase the risk of metachronous development of second primary malignancy under the condition of prolonged immunosuppression. Therefore, we analyzed the incidence of DNM following LT according to the status of pretransplant hepatic malignancy.
Go to : 
METHODS
Study design and patient selection
This was a retrospective double-arm study regarding the incidence of DNMs after LDLT. Because the actual incidence of de novo HCC and other primary hepatic malignancies is extremely rare, such hepatic DNMs were not taken into this study. The LT database at our institution was searched to identify adult patients who underwent primary LDLT during 7 years from January 2010 to December 2016. We excluded perioperative mortality cases with less than 3 months of survival after LT. Foreign patients were also excluded because they were not followed up regularly for long periods. We finally identified 2,076 adult LDLT recipients. These study patients were followed up until June 2019 or patient death, making the observation period 30 months or longer.
Primary liver malignancy before LT included HCC and other incidentally detected hepatic malignancies in the explant livers (HCC, combined HCC-cholangiocarcinoma and intrahepatic cholangiocarcinoma).1415 Patients showing complete pathological response after pretransplant HCC treatment were included in the HCC category. The study patients were divided into pretransplant malignancy group and no malignancy group according to the status of pretransplant hepatic malignancy.
Institutional immunosuppressive regimens
Primary immunosuppressive protocols used for adult LT recipients at our institution comprised interleukin-2 receptor inhibitor, intraoperative steroid bolus (5–10 mg/kg), intravenous or oral calcineurin inhibitor (CNI) and corticosteroid recycling beginning on day 1, and adjunctive mycophenolate mofetil for patients showing CNI-associated adverse effects or for immunosuppression augmentation. There were no differences in immunosuppressive regimens between LDLT and deceased donor LT. Corticosteroid was rapidly tapered off within the first 3 months.161718 The indications of mammalian target of rapamycin (mTOR) inhibitors were HCC recurrence, DNM, and renal dysfunction. Because everolimus is covered by social health insurance since early 2016 in Korea and is not included as a primary immunosuppressant in our institution, only a small number of patients were administered everolimus before development of HCC recurrence or DNM. Thus, the anti-tumor effect of mTOR inhibitors was not taken into account in this study.
Pretransplant evaluation for malignancy
According to the guidelines of the Korean Association for the Study of the Liver, Korean individuals with chronic liver disease are regularly followed-up to detect HCC.19 Routine pretransplant evaluations for HCC and other malignancies include abdomino-pelvic and chest computed tomography (CT) scans, abdominal magnetic resonance imaging, 2-18F-fluoro-2-deoxy-D-glucose positron emission tomography, upper gastrointestinal endoscopy, and sigmoidoscopy. Full endoscopic evaluation of the colon and rectum is performed in selected patients owing to the risk of procedure-related complications. The details of this preoperative evaluation process were described previously.21319
Posttransplant patient surveillance
Our institutional posttransplant surveillance protocols for adult recipients includes HCC surveillance with imaging and tumor marker studies as well as DNM surveillance with imaging and endoscopic studies.231319
Routine follow-up protocols for all adult recipients include abdomen-pelvis and chest CT scans every 6 months during the first 3 years, once per year during 4–5 years, and every 2 years after 5 years. Patients with high risk of liver tumor recurrence, which include HCC beyond the Milan criteria, combined HCC-cholangiocarcinoma and intrahepatic cholangiocarcinoma, are indicated for more frequent cancer surveillance follow-ups, particularly during the first 2 years.
Our institutional surveillance protocols for extrahepatic DNM include gastroscopy every 2 years, colonoscopy every 4–5 years, breast cancer examinations every year, prostate-specific antigen testing every year, chest X-rays every year, and cervical cancer smears every year. If metaplastic changes of the gastric mucosa are detected, we suggest performing gastroscopy annually. If colonic adenomas are resected, the interval to the next colonoscopy is shortened to 1–3 years.13
Statistical analysis
Continuous variables are reported as means with standard deviation and compared using Student's t-test. Categorical variables were compared using the χ2 test. Survival rates were determined using the Kaplan-Meier method and compared using log-rank test. A P value of < 0.05 was considered to indicate a statistically significant difference. Statistical analyses were performed using SPSS (version 22; IBM, New York, NY, USA).
Ethics statement
The Institutional Review Board of Asan Medical Center approved this study protocol (2019-1347).
Go to :
RESULTS
Stratification of patients according to pretransplant diagnosis of hepatic malignancy
The study cohort included 2,076 adult LDLT recipients. Primary hepatic malignancy was diagnosed in 1,012 patients (48.7%) before LT operation or at the explant liver pathology, including HCC in 991 patients, combined HCC-cholangiocarcinoma in 11 patients, and intrahepatic cholangiocarcinoma in 10 patients. These patients were selected as the pretransplant hepatic malignancy group (n = 1,012). Thus, the remaining 1,064 patients (51.3%) became the pretransplant no hepatic malignancy group.
The clinical profiles of these two groups are summarized in Table 1. The pretransplant hepatic malignancy group had lower patient age at LT operation, higher proportion of men patients, higher proportion of hepatitis B virus infection, lower model for end-stage liver disease score, lower graft-recipient weight ratio, and higher proportion of ABO-incompatible LDLT compared with the pretransplant no hepatic malignancy group.
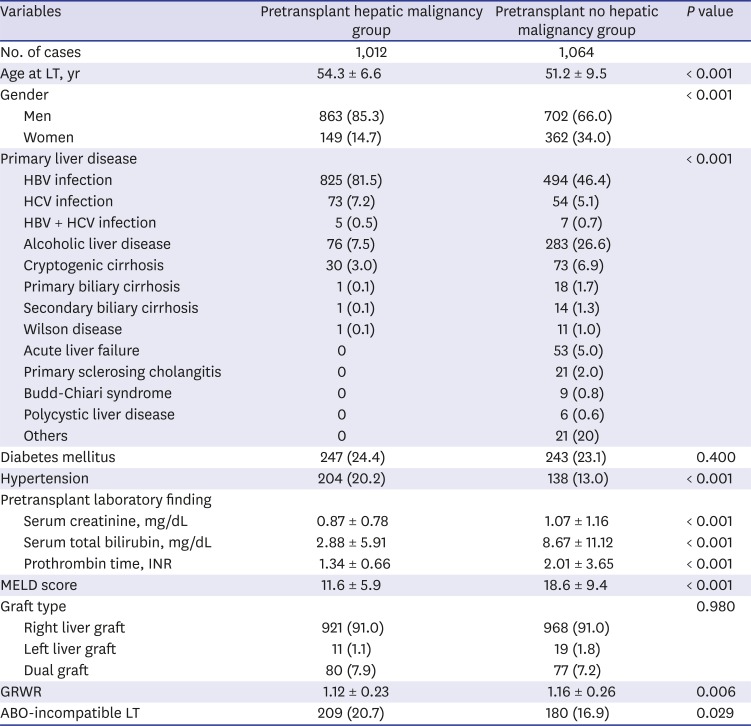
Table 1
Comparison of the patient profiles according to the status of pretransplant hepatic malignancy
Data are presented as mean ± standard deviation or number (%).
LT = liver transplantation, HBV = hepatitis B virus, HCV = hepatitis C virus, INR = international normalized ratio, MELD = model for end-stage liver disease, GRWR = graft-recipient weight ratio.
![]()
Comparison of the curatively treated extrahepatic malignancies precedent to LDLT operation
Precedent to LDLT operation, 76 patients (3.6%) had a past medical history of various extrahepatic malignancies, which were diagnosed 2–15 years before LDLT operation. Decision to perform LDLT operation was made after we confirming that these malignancies were curatively or potentially-curatively treated.
These precedent extrahepatic malignancies were diagnosed in 38 patients (3.8%) in the pretransplant hepatic malignancy group and were as follows: colorectal cancer in 8 patients (0.8%), thyroid cancer in 6 patients (0.6%), renal cell cancer in 5 patients (0.5%), stomach cancer in 5 patients (0.5%), breast cancer in 4 patients (0.4%), lung cancer in 2 patients (0.2%), pharyngeal cancer in 2 patients (0.2%), prostate cancer in 2 patients (0.2%), esophageal cancer in 1 patient (0.1%), thymus cancer in 1 patient (0.1%), cervix cancer in 1 patient (0.1%), and endometrial cancer in 1 patient (0.1%).
In the pretransplant no hepatic malignancy group, precedent extrahepatic malignancies were also diagnosed in 38 patients (3.6%) and were as follows: stomach cancer in 10 patients (0.9%), thyroid cancer in 8 patients (0.8%), lymphoma in 6 patients (0.6%), colorectal cancer in 5 patients (0.5%), breast cancer in 3 patients (0.3%), laryngeal cancer in 1 patient (0.1%), lung cancer in 1 patient (0.1%), renal cell cancer in 1 patient (0.1%), urinary bladder cancer in 1 patient (0.1%), endometrial cancer in 1 patient (0.1%), and skin cancer in 1 patient (0.1%).
There was no statistical difference in the incidences of precedent treated extrahepatic malignancies before LDLT between the two groups (P = 0.82). At the time of writing this manuscript, all patients have passed 5 years or more after treatment of the precedent extrahepatic malignancy. None of these patients have experienced recurrence of the same extrahepatic malignancies after LDLT operation.
Incidence of posttransplant DNMs according to pretransplant status of hepatic malignancy
In the pretransplant hepatic malignancy group, extrahepatic DNMs after LDLT developed in 45 patients (4.4%). Common malignancies were posttransplant lymphoproliferative disease (PTLD) in 10 patients (1.0%), lung cancer in 10 patients (1.0%), stomach cancer in 6 patients (0.6%), colorectal cancer in 5 patients (0.5%), bladder cancer in 3 patients (0.3%), and other cancers in 11 patients (1.1%) (Table 2). Among these patients, 11 patients died due to progression of DNM (n = 10) and concurrent HCC recurrence (n = 1). Another 71 patients died due to primary hepatic malignancy recurrence without DNM development.
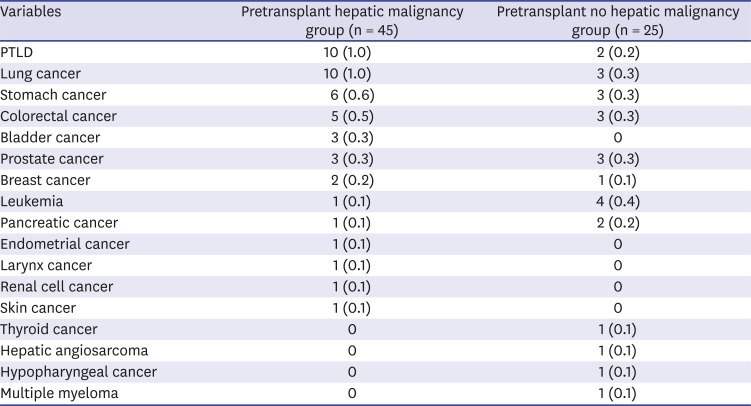
Table 2
Types and incidences of posttransplant de novo malignancies according to the status of pretransplant hepatic malignancy
![]()
Conversely, in the pretransplant no hepatic malignancy group, posttransplant extrahepatic DNMs developed in 25 patients (2.3%). Common malignancies were colorectal cancer in 3 patients (0.3%), stomach cancer in 3 patients (0.3%), leukemia in 3 patients (0.3%), lung cancer in 3 patients (0.3%), PTLD in 2 patients (0.2%), prostate cancer in 2 patients (0.2%), and other cancers in 9 patients (0.9%) (Table 2). Among these patients, 4 patients died due to DNM progression.
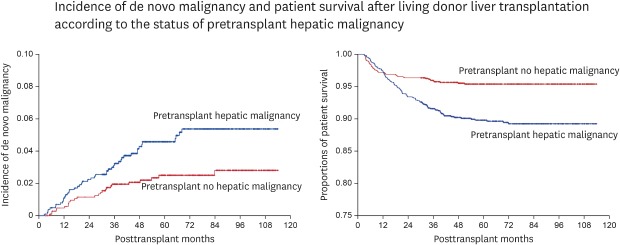
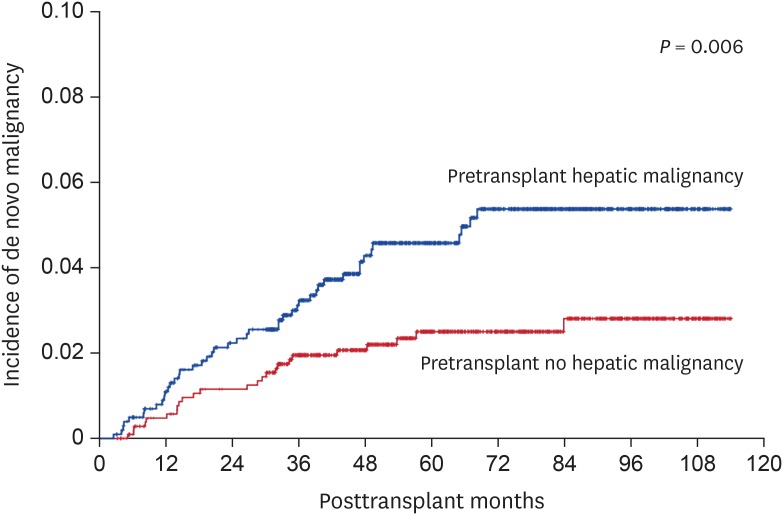
The pretransplant hepatic malignancy group showed a higher overall incidence of extrahepatic DNM compared with the pretransplant no malignancy group (P = 0.008). The incidence rates of extrahepatic DNMs in the pretransplant hepatic malignancy and no hepatic malignancy groups were 1.1% and 0.5% at 1 year, 3.2% and 2.0% at 3 years, 4.6% and 2.5% at 5 years, and 5.4% and 2.8% at 8 years, respectively (P = 0.006) (Fig. 1).
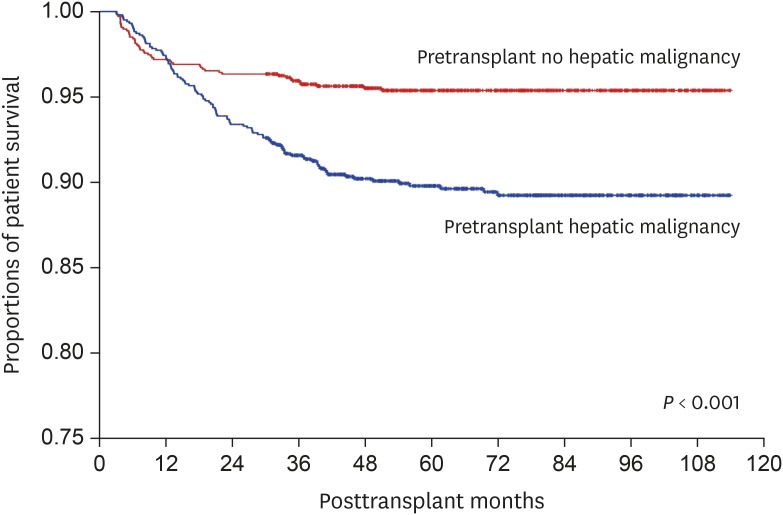
The survival curves in these two groups are shown in Fig. 2. The overall patient survival rates in the pretransplant malignancy and no malignancy groups were 97.3% and 97.2% at 1 year, 91.6% and 95.9% at 3 years, 89.8% and 95.4% at 5 years, and 89.2% and 95.4% at 8 years, respectively (P < 0.001). The pretransplant hepatic malignancy group showed inferior outcomes because 97 patients showed posttransplant recurrence of the primary hepatic malignancy and 71 of them died due to tumor progression.
Risk factor analysis for incidence of posttransplant extrahepatic DNMs
Considering that the pretransplant patient characteristics were significantly different between the pretransplant hepatic malignancy and no hepatic malignancy groups, further analysis was necessary to find out other risk factors for posttransplant extrahepatic DNM.
Univariate analysis with the status of pretransplant hepatic malignancy, gender, primary liver disease and ABO blood group-compatibility showed that pretransplant hepatic malignancy was the only significant risk factor for posttransplant extrahepatic DNM (Table 3).
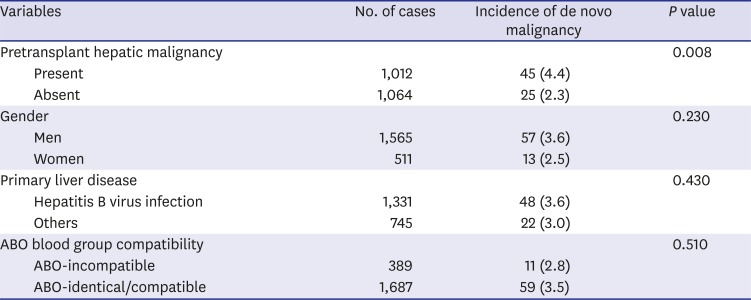
Table 3
Univariate analysis on risk factor for posttransplant de novo malignancy
![]()
Go to :
DISCUSSION
The incidence of DNMs after LT is reported to be 4%–16%, depending on the length of the observation period, recipient age and immunosuppressive regimens.678910 We previously reported that the incidence of DNM was 2.3% with a mean observation period of 42 months.12 In this study, it was 3.4% with a mean observation period of 67.5 ± 27.2 months.
The results of this study revealed that pretransplant hepatic malignancy was the only significant risk factor for development of posttransplant DNMs. To our knowledge, this is the first report on the relationship between pretransplant hepatic malignancy and posttransplant DNM. If a DNM develops in a LT recipient with pretransplant hepatic malignancy, these tumors are metachronous double primary malignancies. We presume that patients with such metachronous double primary malignancies may have potential problems in the natural immune surveillance for cancer cells.2223
The types of DNMs after LT appear to be different in Western and Asian countries because the development of a new malignancy is influenced by various racial and social factors, including endemic circumstances. LT recipients are indicated for periodic screening for malignancies commonly in the general population, which must be helpful for early detection of DNMs in LT patients.12132021
PTLD is one of the most common DNMs after LT and accounted for 17.1% of all DNMs in this study. The spectrum of PTLD after LT ranges from polymorphic lymphoproliferation to high-grade monoclonal lymphoma. Risk factors for PTLD include Epstein-Barr virus-seronegativity of the recipient, young age, intensity of immunosuppression, and the posttransplant first year. Management of PTLD includes reduction of immunosuppression, rituximab, combination chemotherapy, and adoptive immunotherapy.242526
Lung cancer is also one of the most common solid organ DNMs after LT and accounted for 18.6% of all DNMs in this study. A Japanese national survey of DNM after solid organ transplantation revealed that the common malignancies were PTLD (n = 87), kidney cancer (n = 43), stomach cancer (n = 41), colorectal cancer (n = 41), and lung cancer (n = 36).27 Most patients with de novo lung cancer had no pulmonary symptoms. Thus, early diagnosis is important for effective treatment, making routine surveillance through regular visits to the outpatient clinic necessary. Simple chest X-rays are relatively insensitive in detecting small pulmonary nodules suitable for resection. In contrast, routine chest CT is accurate and effective in detecting small lung masses.28 Although chest X-rays do not readily detect small lung nodules, their clinical role in LT recipients should not be underestimated because they still remain the best screening tool in LT recipients who take life-long immunosuppressive therapy. Surgical treatment for de novo lung cancer is feasible and may prolong survival.29
The incidence of stomach cancer is very high in the Korean general population; thus, biannual endoscopic screening for stomach cancer is highly recommended for all individuals over the age of 40 years.1120 Incidental detection of early stomach cancer enables to perform minimally invasive endoscopic mucosal resection. We previously reported that 26 cases of stomach cancer were detected at 60.2 ± 29.8 months after LT.13 Among the 18 patients who regularly underwent endoscopic screening, early stomach cancer was diagnosed in 14 and their 2-year survival rate after diagnosis of stomach cancer was as high as 93.1%. In contrast, advanced stomach cancer was detected in 8 patients who did not receive regular screening, and their 2-year survival rate after diagnosis of stomach cancer was only 33.3%.
The incidence of colorectal cancer has been gradually increasing in Korea; thus, LT recipients should be periodically assessed for early detection of colorectal cancer.1321 We previously reported that 22 cases of colorectal cancer were detected at 54.3 ± 38.0 months after LT.13 Among 19 patients who regularly underwent endoscopic screening, early colorectal cancer was diagnosed in 12 and their 2-year survival rate after colorectal cancer diagnosis was 92.3%. In contrast, advanced colorectal cancer was detected in 3 patients who did not receive regular screening, and their 2-year survival rate after colorectal cancer diagnosis was only 33.3%.
The survival outcomes of patients with less aggressive cancers, such as thyroid and breast cancers, are also more favorable when tumors are detected in routine screening. We highly recommend observing our institutional surveillance protocols for detection of DNMs as above mentioned. Because our surveillance guidelines are identical to the general recommendations of the Korean nationwide social health program, most of these examinations are charge-free for LT recipients and the general population in Korea.20
HCC surveillance after LT is different from that after hepatic resection or non-surgical HCC treatment because of different risk of HCC recurrence. For patients with minimal risk for HCC recurrence such as super-selection criteria, they do not require additional imaging studies besides routine regular surveillance and regular measurement of HCC tumor markers.2 In contrast, patients with HCC exceeding the Milan criteria or Asan criteria require frequent imaging studies for strict surveillance, particularly during the first 2 years. Regardless of HCC tumor stage at the time of LT operation, if HCC recurrence did not develop within 5 years, the surveillance protocol with imaging studies is nearly the same as in patients without HCC because the risk of HCC recurrence is very low. However, posttransplant HCC recurrence can develop even after 10 years; thus, recurrence risk-adjusted lifelong surveillance is mandatory.234
It is presumed that long-term immunosuppression increases the risk of recurrence of pretransplant malignancies and the risk of DNM.5630 The Consensus on Managing Modifiable Risk in Transplantation group described the main risk factors for graft loss in kidney and liver transplant recipients and provided useful recommendations to extend the long-term graft survival and to decrease the chances of DNM development.31 Immunosuppressive agents activate different pathways in the immune system and need to be carefully selected. CNIs seem to have a cancer-promoting influence that might be related to their blood level concentration. Association of multiple agents in lifelong immunosuppression regimens might be responsible for a substantially higher risk of DNMs.32
Introduction of mTOR inhibitors in Korea has made some noticeable changes in immunosuppressive regimens. Everolimus has been covered by social health insurance since early 2016 in Korea. Thus far, we do not consider this agent to be a primary immunosuppressive agent for LT; thus, it has not been frequently used in our institution yet. The most common indication of everolimus in our institution is conversion to everolimus after development of HCC recurrence or DNM because mTOR inhibitors are known to be the only immunosuppressive agent with anti-tumor effects.33 Our previous study presented that the overall administration rate of everolimus is not high, but its use is gradually increasing with the expansion of indications.16 Everolimus monotherapy has also been adopted, particularly in patients with overt presentation of HCC recurrence or DNM because CNI medication may be not beneficial for tumor control. We also attempted to concurrently use mTOR inhibitor and sorafenib with an expectation of synergistic effect against HCC recurrence, but their synergistic effect was not proven.4
This study has several limitations. This is a retrospective single-center study. We did not analyze the effect of immunosuppressive regimens on the development of extrahepatic DNM. Further studies with a larger number of patients and longer observation periods are required to reveal the real-world incidence and risk factors of posttransplant DNM. A small number of patients who had a diagnosis of precedent extrahepatic malignancy have passed less than 5 years after its treatment at the time of LDLT operation, thus a further follow-up period is necessary although they passed 5 years or more at the time of writing this manuscript.
In conclusion, our findings suggest that lifelong surveillance for all types of malignancy is necessary after LT. We suggest patients having pretransplant hepatic malignancy be followed up more strictly because they are at risk of hepatic malignancy recurrence and a higher risk of extrahepatic DNM compared with the patients without pretransplant hepatic malignancy.
Go to :
 XML Download
XML Download