

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In 2010, an estimated 14.9 million babies were born preterm, constituting 11.1% of all live births worldwide.1 In Korea, the preterm birth rate has steadily increased since 2006, with 7.2% of births occurring before 37 weeks of gestation in 2016.2 Complications due to premature birth are the leading cause of neonatal mortality, responsible for nearly 1 million deaths in 2013.3 Preterm infants are at a high risk for complications such as respiratory distress syndrome, necrotizing enterocolitis, intraventricular hemorrhage, and cerebral palsy.456 In the long-term, premature babies are at an increased risk for vision and hearing loss, intellectual disability, cognitive impairment and chronic conditions such as diabetes mellitus and cardiovascular diseases, even in adulthood.4789
Regarding the potential mechanisms of spontaneous preterm birth (sPTB), infection, uterine overdistension because of multiple gestation or hydramnios, decline in progesterone action, cervical diseases, decidual senescence, breakdown of maternal-fetal tolerance, and vascular diseases have been proposed.1011 It has been reported that the incidence of cervical incompetence in twin pregnancies was seven fold greater than in singleton pregnancies, which was associated with more advanced cervical change and preterm birth.12 A history of a sPTB is a well-known risk factor for subsequent spontaneous preterm delivery.131415
Although the recurrence risk for preterm birth after a preterm twin delivery has been questioned, recent studies support that women with a history of twin sPTB have an increased risk of preterm birth.161718 Few studies have investigated effective strategies for preventing preterm birth in singleton pregnancies after a twin sPTB, however.
The purpose of this study was to evaluate the effect of cervical cerclage on the recurrence risk for preterm birth in singleton pregnancies after a spontaneous preterm twin delivery.
Go to : 
METHODS
Subjects
This multicenter, retrospective study was conducted at 10 institutions in Korea: Ajou University Hospital, Asan Medical Center, Dongguk University Ilsan Hospital, Kangwon National University Hospital, Keimyung University Dongsan Medical Center, Konkuk University Medical Center, Korea University Anam Hospital, Kyung Hee University Hospital at Gangdong, Seoul National University Hospital, and Seoul St. Mary's Hospital. Medical records of all women with singleton pregnancies who had a prior preterm twin delivery and were referred to the departments of obstetrics and gynecology at the participating centers between January 2009 and December 2018 were collected in a dedicated merged database and included in the study. The inclusion criteria for this study were singleton pregnancies in women with a history of preterm twin birth due to spontaneous preterm labor, incompetent internal os of cervix (IIOC), or preterm premature rupture of membrane (PPROM). Spontaneous preterm labor was defined to be regular contractions before 37 weeks that are accompanied with cervical change. IIOC was diagnosed only when a patient showed cervical dilatation but did not have uterine contractions when she visited a hospital. In all participants, the estimated date of delivery was confirmed by a first-trimester ultrasound or a second-trimester ultrasound that was correlated with their menstrual dates.
Exclusion criteria
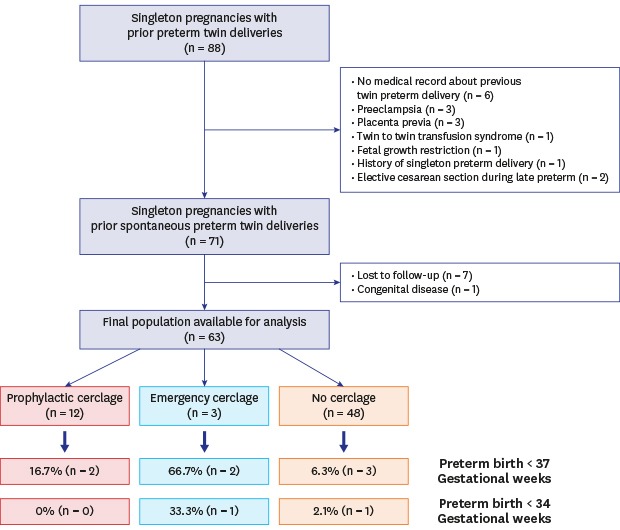
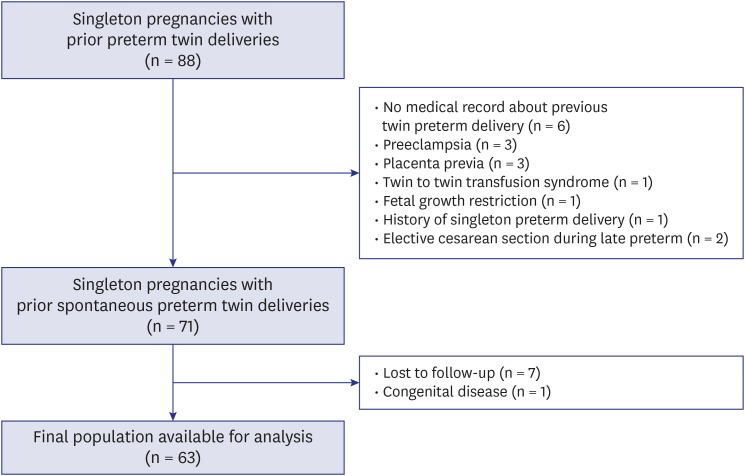
Exclusion criteria were previous preterm twin birth due to severe preeclampsia, placenta previa, twin-to-twin transfusion syndrome (TTTS), twin reversed arterial perfusion (TRAP), intrauterine fetal growth restriction, oligohydramnios, hydramnios, or non-reassuring fetal status; a history of preterm twin birth of unknown indication or unknown gestational age; an additional preterm delivery before the preterm twin birth; and elective cesarean section during the late preterm. Women who were lost to follow-up or whose pregnancy was complicated by Down syndrome with multiple anomalies in a fetus were excluded. Fig. 1 shows the study population framework, including the total number of pregnancies assessed.
Outcome measures
To investigate the effect of cervical cerclage on the recurrence risk for preterm birth in women with a prior preterm twin delivery, we compared the following perinatal and obstetric data between women who had preterm birth and those who had full-term births: maternal age, prepregnancy and predelivery body mass index (BMI) in kg/m2, gravidity, parity, number of spontaneous abortions, and pregnancy interval.
We also compared women who had cervical cerclage with those who did not. For these two groups, we examined demographic variables, baseline obstetric characteristics, and pregnancy outcomes like maternal age, pregnancy interval, gestational age at prior twin preterm birth, shortest cervical length during present pregnancy before 37 weeks of gestation, cesarean section for prior twin preterm delivery, use of progesterone during present pregnancy, indication of previous preterm birth (preterm labor, IIOC, or PPROM), and preterm birth at less than 37 and 34 weeks of gestation in the present pregnancy.
In women who received progesterone during pregnancy, daily 200 mg vaginal micronized natural progesterone or weekly intramuscular injection of 250 mg 17 alpha-hydroxyprogesterone caproate were used from 16 weeks' gestation to 36 weeks' gestation.
Cervical cerclage was classified as prophylactic cerclage and emergent cerclage. Prophylactic cervical cerclage was performed in asymptomatic pregnant women between 12 and 17 gestational weeks with cervical length more than or equal to 2 cm, by maternal-fetal medicine specialists in each hospital. Emergent cervical cerclage was performed as a salvage procedure in pregnant women with cervical length less than 2 cm and cervical dilatation or amniotic membrane bulging in mid-trimester. The McDonald technique was used in all the patients in the cerclage group.
Statistical analysis
Categorical data were presented as percentages (%) and compared using the χ2 test or Fisher's exact test. Continuous variables were presented as mean ± standard deviation (SD). We performed a multivariate logistic regression analysis to study the relationship between cervical cerclage and subsequent singleton preterm birth after adjusting for maternal age, pregnancy interval, progesterone use, fetal sex and gestational age at previous preterm twin birth. Statistical significance was defined by a P value < 0.05. Statistical calculations were performed using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
The Institutional Review Boards of all the participating institutions provided ethics approval (The Catholic University of Korea, Seoul St. Mary's Hospital, approval No. KC19RCDI0454). An informed consent was waived by the Institutional Review Boards of all the participating institutions.
Go to :
RESULTS
Baseline characteristics of groups with versus without cerclage
Among 88 singleton deliveries to women with a history of preterm twin birth, 63 deliveries were analyzed. Of those 63, 15 (23.8%) underwent cervical cerclage during their present pregnancies, and 48 (76.2%) did not. Table 1 summarizes the demographic and baseline characteristics of each group.
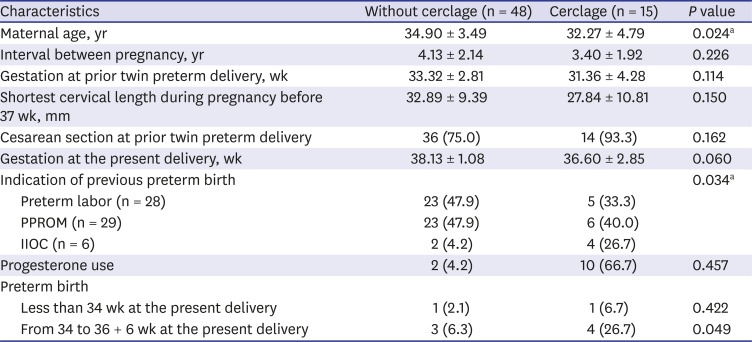
Table 1
Baseline characteristics of cerclage and without-cerclage group
Data are presented as mean ± standard deviation or number (%).
IIOC = incompetent internal os of the cervix, PPROM = preterm premature rupture of membranes.
aP < 0.05.
![]()
Maternal age was significantly older in the group of pregnancies without cerclage than in the group with cerclage (34.90 ± 3.49 vs. 32.27 ± 4.79 years, P = 0.024). The gestational age at prior preterm twin birth was more advanced in the group of pregnancies without cerclage than in the group with cerclage, although the difference was not significant (33.32 ± 2.81 vs. 31.36 ± 4.28 weeks, P = 0.114). Regarding the indication for previous preterm birth, the rate of IIOC was much higher in the cerclage group than in the no cerclage group (26.7 vs. 4.2%, P = 0.025), but the rates of preterm labor and PPROM did not significantly differ. The rate of preterm birth before 37 weeks of gestation in the present pregnancy was higher in the cerclage group than in the no cerclage group (26.7 vs. 6.3%, P = 0.049). However, the rate of preterm birth before 34 weeks of gestation was not significantly different. In addition, there was no significant difference in cervical lengths during the present pregnancy between women with cerclage and those without cerclage.
Baseline characteristics of preterm versus full-term births
Of 63 singleton pregnancies in women with a prior preterm twin birth, seven (11.1%) had preterm births and 56 (88.9%) had full-term births in the present pregnancy. Table 2 shows perinatal and obstetric data for each group.
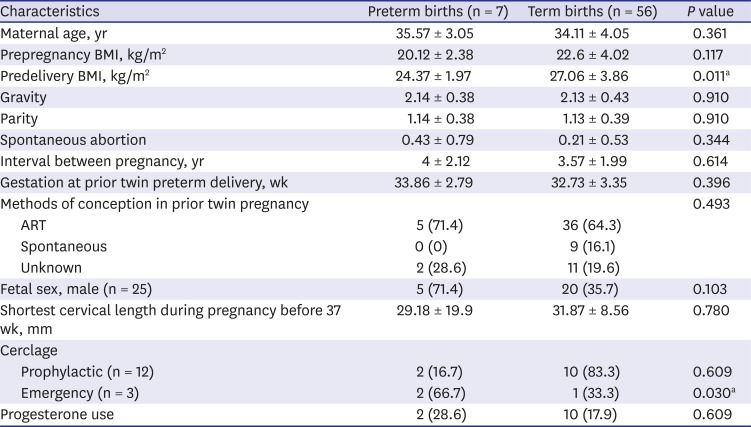
Table 2
Baseline characteristics of group of preterm birth and group of term birth in the present pregnancies
Data are presented as mean ± standard deviation or number (%).
BMI = body mass index, ART= assisted reproductive technology.
aP < 0.05.
![]()
Predelivery BMI was greater in the full-term delivery group than in the preterm delivery group (27.06 ± 3.86 vs. 24.37 ± 1.97 kg/m2, P = 0.011). There was a significantly higher rate of emergency cerclage in the preterm birth group than in the full-term birth group (66.7 vs. 33.3%, P = 0.03). However, the rates of prophylactic cerclage did not significantly differ between the two groups.
Multivariate logistic regression analysis for risk of recurrent preterm birth
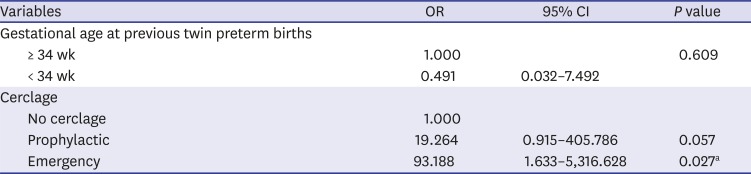
A multivariate logistic regression analysis demonstrated that the placement of emergency cerclage is an independent risk factor for recurrent singleton preterm birth in a subsequent pregnancy (odds ratio [OR], 93.188; 95% confidence interval [CI], 1.633–5,316.628; P = 0.027) (Table 3). However, prophylactic cervical cerclage did not significantly increase the risk of recurrent singleton preterm birth. Although the mean gestational age at delivery was significantly greater in the no cerclage group than in the prophylactic cerclage group (38.13 ± 1.08 vs. 37.25 ± 0.97, P = 0.013), none of the women who had prophylactic cervical cerclage, delivered before 35 weeks of gestation in the present singleton pregnancy (Fig. 2).
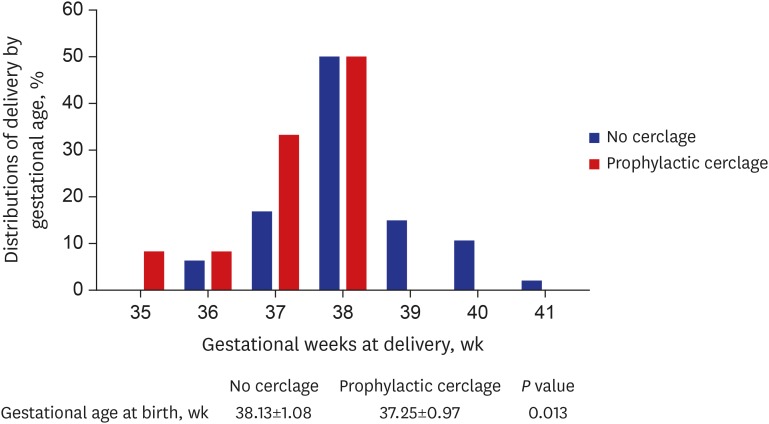 | Fig. 2Gestational age at birth of prophylactic cerclage and without-cerclage group.Data are mean ± standard deviation. Significant P value: P < 0.05.
|
Table 3
Multivariate logistic regression analysis for the risk of recurrent singleton preterm birth with prior preterm twin birth
![]()
Go to :
DISCUSSION
In this study, cerclage did not lower the risk of sPTB in a subsequent singleton pregnancy after a twin sPTB. Moreover, the emergency cerclage group had a higher risk of sPTB. However, preterm labor may have already progressed in women in the emergency cerclage group; therefore, it is unclear whether emergency cerclage is a risk factor or consequence of sPTB. Prophylactic cerclage did not significantly increase the risk of preterm birth. Although the mean gestational age at delivery was significantly greater in the no-cerclage group than in the prophylactic cerclage group, none of the women who had prophylactic cervical cerclage delivered a baby before 35 weeks of gestation in the subsequent singleton pregnancy (Fig. 2).
A recent meta-analysis reported that vaginal progesterone and cerclage are equally effective in preventing preterm birth in women with a previous sPTB.19 However, the existing evidence does not support the use of cerclage for the prevention of preterm birth in women with cervical conization, because the indications and results are inconsistent.2021 Suture materials in the uterine cervix can cause inflammation after cerclage; therefore, repeated trauma on the cervix from conization followed by cerclage might be related to an inflammatory response and increase the risk of preterm birth.21 The efficacy of cerclage in a subsequent singleton pregnancy after a twin sPTB is unknown.
In the present study, there was an 11.1% risk of preterm birth in a subsequent singleton pregnancy after a twin sPTB. Previous studies have reported a rate of 20%–30% for sPTB in women with a previous singleton sPTB.2223 Data about the risk of recurrent sPTB in the next singleton pregnancy after a twin sPTB is very limited, however; reported rates vary, from 7.3% to 18.5%.16171824 Some authors have suggested that the risk of a singleton preterm birth increases to 18.2% among women with a previous twin sPTB before 34 weeks' gestation; however this was not observed among women with a previous twin sPTB at 34 weeks' gestation or later.25 A common finding from the previous studies was an association between earlier gestational age at twin sPTB and higher risk of sPTB in the next singleton pregnancy.1617252627 However, we found no significant difference in the risk of preterm birth in the next singleton pregnancy as per the previous twin sPTB before or after 34 weeks' gestation.
According to the American College of Obstetricians and Gynecologists (ACOG) guideline for the prevention of preterm birth, a woman with a singleton gestation and a previous spontaneous preterm singleton birth should be offered progesterone supplementation starting at 16–24 weeks of gestation; moreover, cerclage should be considered if the cervical length is less than 25 mm before 24 weeks of gestation and the prior preterm birth occurred at less than 34 weeks of gestation.282930 To our knowledge, there are no data or guideline about singleton pregnancies after a preceding twin sPTB; therefore, we need to follow the general ACOG guideline regarding the prevention of preterm birth until a future study demonstrates the efficacy of specific strategies in this population.
Our study has certain limitations, mainly because of its retrospective nature and relatively small number of cases. However, given the infrequency of singleton pregnancy following twin sPTB, the feasibility of performing a sufficiently powered randomized trial in a single center is limited. Another limitation of the study may be the heterogeneity of ten nationwide centers that prevented us from conducting subgroup analyses according to the different variables that may have been clinically important, such as the cervical length and gestational week at cerclage, use of cerclage in combination with progesterone, as well as the suture material.
A major strength of our study is that to our knowledge, this is the first to evaluate the efficacy of cerclage in this specific population. Further, specialists in maternal-fetal medicine at the tertiary university hospitals routinely examine the prenatal care records and routine hospital documents before entering them into the patient's file, minimizing possibility of missing data. In addition, to our knowledge, this is the first study to evaluate the risk of preterm birth in a subsequent singleton pregnancy among Korean women with a preceding twin sPTB. Previously, the overall risk of preterm birth in a subsequent singleton pregnancy among Korean women with a preceding twin preterm birth was reported to be 3.2%.24 This percentage is much lower than that in our study (11.1%). It is noteworthy that 3.2% is much lower than the overall preterm birth rate in Korea; this may indicate that this specific population is at low-risk.
In this study, prophylactic cerclage did not decrease or increase the risk of preterm birth in women with prior twin sPTB. However, there was no case of preterm birth before 35 weeks' gestation among the prophylactic cerclage group. Our study employed a relatively smaller sample size; therefore, we could not find the relationship between the risk of sPTB in subsequent singleton pregnancies and the severity of prematurity in the prior twin pregnancy. However, as per previous studies, the risk of sPTB is related to the severity of prematurity in the prior twin pregnancy.161726 In particular, in the group of pregnant women who experienced twin sPTB at < 30 weeks' gestation, the risk of sPTB in the subsequent singleton pregnancy was about 6-fold higher than in the group of pregnant women with a history of twin delivery at term1726 and was about 2 fold higher than in the group of pregnant women who delivered a twin between 30 + 0 and 33 + 6 weeks' gestation. Therefore, considering that there was no case of preterm birth at < 35 weeks' gestation among the prophylactic cerclage group in this study, close monitoring of the cervical length and prophylactic cerclage might be considered in women who experienced sPTB at < 30 weeks, in a preceding twin pregnancy to avoid emergency cerclage after the onset of preterm labor or early preterm birth.
Although there was no significant difference, there was a tendency of higher preterm birth rate in the assisted reproductive technology (ART) group, compared to the spontaneous pregnancy group. Because a meta-analysis also reported that the risk of sPTB in singleton pregnancies resulting from ART is significantly greater than that in spontaneously conceived singletons, we might need to monitor high risk women more closely in pregnancies resulting from ART.31
Women with singleton pregnancies after preceding twin sPTB are at a high risk of sPTB, and an emergency cerclage was associated with a higher risk of preterm birth. Further investigations about management, including indications of prophylactic cerclage are required in women with singleton pregnancies after preceding twin sPTB. However, close monitoring of the cervical length and prophylactic cerclage might be considered in women who have experienced sPTB before 30 weeks' gestation in a preceding twin pregnancy in order to prevent recurrent preterm birth at extreme gestation during a subsequent singleton pregnancy.
Go to :
 XML Download
XML Download