

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Survival rate of preterm infants has been improved in the past several decades because of advances in neonatal and perinatal care.12 The survival rate of extremely preterm infants who are at the limit of viability is also improved. Consequently, there are growing concerns of more survivors with major morbidities who were born extremely premature.3 However, improved survival of preterm infants is associated with improved survival of those without major morbidity, namely intact survival.4 Improved survival of infants with gestational age (GA) of 23–24 weeks is associated with improved survival of infants with GA of 25–26 weeks without major morbidity.5 Improved survival rates of very low birth weight infants (VLBWIs) are in parallel with general improvements of maternal, prenatal, perinatal, and neonatal care.6 Hence, improved survival rates with improved intact survival can be explained. However, whether decreased mortality rate is associated with increased survival without major morbidities remains controversial. In Korea, survival rate of VLBWIs had increased from 77.5% in 2002 to 85.7% in 2009. Survival rate of extremely low birth weight infants (ELBWIs) had also markedly increased from 56.1% in 2002 to 71.8% in 2009.7 The Korean Neonatal Network (KNN) database registration system was launched in 2013. Seventy neonatal intensive care units (NICUs) are participating in KNN registry now.8 Based on KNN data, Chung and Bae9 reported that survival rates of VLBWIs and ELBWIs had increased from 83.4% in 2014 (55 NICUs) to 86.4% in 2015 (60 NICUs) and from 67.1% in 2014 (55 NICUs) to 70.9% in 2015 (60 NICUs), respectively. Survival rates of VLBWIs in registration systems of other neonatal networks were higher than those in KNN data: 95.0% in Neonatal Research Network of Japan (NRNJ), 91.5% in Australian and New Zealand Neonatal Network (ANZNN), 90.4% in Canadian Neonatal Network, 89.8% in Swiss Neonatal Network (SwissNeoNet), 89.7% in United Kingdom Neonatal Collaborative, and 86.1% in Israel Neonatal Network (INN) between 2007 and 2010.10
In contrast, the survival rate of VLBWIs is not improved recently. It might have reached a plateau. It was 85% between 1997 and 2002 based on data from Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Neonatal Research Network (NRN).11 Mortality rate of preterm infants is an important indicator of overall quality of NICU. Mortality rate of preterm infants accounts for a large proportion of neonatal mortality rate.12 We can reduce neonatal mortality by reducing preterm mortality which is an important issue for social health. Data according to birth weight can be distorted by growth restricted infants and small for GA infants because they are more mature than those with the same birth weight. Hence, this study was conducted to evaluate the mortality rate of preterm infants with GA <30 weeks according to era and GA in a single center over 10 years. Time of death and causes of death were also evaluated.
Methods
This study was approved by the Institutional Review Board of Inje University Busan Paik Hospital (identification code: 19-0154) in accordance with the Declaration of Helsinki, including a waiver of parental consent for this retrospective chart review. Preterm infants with GA <30 weeks who were admitted to Busan Paik Hospital between January 2009 and December 2018 were enrolled.
Demographic factors which can affect mortality rate were compared between survived infants and dead infants. GA, birth weight, gender, Apgar scores at 1 and 5 minutes, maternal gestational diabetes mellitus, maternal pregnancy-induced hypertension (PIH), antenatal steroids therapy, and histologically confirmed chorioamnionitis were included. Early postnatal factors such as respiratory distress syndrome (RDS), need of surfactant re-dosing, and patent ductus arteriosus (PDA) were compared between survived infants and dead infants.
Mortality rates were evaluated according to birth year (from 2009 to 2018) and GA (from GA of 22 weeks to 29 weeks). GA-specific mortality rates according to time of death were also compared (time of death: <24 hours, 1–3 days, 4–7 days, 8–28 days, >28 days). Causes of death were categorized according to the International Classification of Diseases and Related Health Problems 10th revision.13 Cardiorespiratory causes included massive pulmonary hemorrhage, RDS, air leak, pulmonary hypoplasia, bronchopulmonary dysplasia (BPD), and PDA. Neurologic causes included high grade intraventricular hemorrhage (IVH) (grade 3 or 4) and perinatal asphyxia. Gastrointestinal causes included necrotizing enterocolitis (NEC) and spontaneous bowel perforation. Death due to extreme immaturity refers to death immediately after birth. It means death at delivery room despite active resuscitation. Active resuscitation included endotracheal intubation, surfactant instillation, positive pressure ventilation, chest compressions, epinephrine, or volume expander.14
PDA was limited to hemodynamically significant ductus arteriosus. Echocardiography was performed in the patient with symptoms of patent ductus arteriosus. After confirmed by echocardiography, fluid restriction, medical treatment, or surgical ligation was done according to the symptoms of ductus arteriosus. Massive pulmonary hemorrhage was diagnosed when bright red blood was spouted out of the endotracheal tube with typical chest radiographic findings and rapid deterioration of the patient. Pulmonary hypoplasia was diagnosed by antenatal ultrasonography as a mediastinal shift in the absence of diaphragmatic hernia, absence of pulmonary artery or one of its branches on the affected side, and decreased lung volume. Perinatal asphyxia was defined as acidosis with pH <7.0 by cord blood gas analysis and Apgar score <3 at 5 minutes with neurologic symptoms including seizure, hypotonia, or decreased mentality.
Chi-square test or Fisher's exact test was performed for nominal variables. For continuous variables with a normal distribution and homogeneous variance, t-test was performed. The Mann-Whitney U test was performed for variables without a normal distribution or without homogeneous variance such as GA. All statistical analyses were performed using IBM SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Data are given as mean±standard deviation. Statistical significance was considered at P-value <0.05.
Results
1. Mortality rate according to birth year
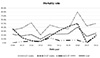
The overall mortality rate of preterm infants with GA <30 weeks was 20.8% (131/629) between January 2009 and December 2018. Mortality rate decreased from 21.9% in 2009 to 9.2% in 2012. It then increased, reaching a plateau at about 20% except in 2016. In 2016, mortality rates were at peak with peak mortality rates of infants with GA ≤25 weeks and GA of 26–27 weeks (Fig. 1).
2. Mortality rate according to GA
Mortality rate decreased as infants matured. It was 80.0% in infants with GA of 22 weeks. It then decreased with increasing GA. It was 2.9% in those with GA of 29 weeks (Fig. 2). Logistic regression analysis revealed that the risk of death decreased by 0.573 times (P<0.001, 95% confidence interval: 0.511–0.642) when GA increased by 1 week.
3. GA-specific mortality rate according to time of death
Death within 24 hours after birth was high in infants with GA of 22 (four cases), 23 (three cases), and 24 (three cases) weeks. Death immediately after birth at delivery room despite active resuscitation was the most common in infants with GA of 22 weeks because of extreme immaturity (three of four cases with GA of 22 weeks, one of three cases with GA of 23 weeks, and one of three cases in with GA of 24 weeks among those with death within 24 hours after birth). However, it was rare in infants with GA ≥25 weeks. Death within 1 week of birth was also high in infants with GA ≤24 weeks. It then decreased with increase GA: 9/12 deaths in those with GA of 22 weeks, 11/26 deaths in GA of 23 weeks, and 11/24 deaths in GA of 24 weeks (Table 1).
4. Causes of death according to GA
Sepsis was the leading cause of death (39 cases/131 deaths). High grade IVH (grade 3 or 4) was the second common cause of death (29 cases/131 deaths), especially in preterm infants with GA ≤24 weeks. Pulmonary hemorrhage, RDS, tension pneumothorax, and PDA were main causes of early death. BPD and NEC were main causes of death after 28 days of life. Death due to congenital anomaly was associated with relatively large GA: one case of double outlet right ventricle with pulmonary stenosis in GA of 26 weeks, one case of lethal atelosteogenesis type 1 in GA of 27 weeks, two cases of Edward syndrome in GA of 28 weeks, two cases of multiple anomalies in GA of 28 weeks and GA of 29 weeks, each (Table 2). Two cases with GA of 28 weeks had sudden onset of circulatory collapse with refractory hypotension.
5. Demographic variables
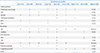
GA and birth weight were smaller in the dead group compared to those in the survived group (GA: 27.5±1.8 vs. 25.4±2.0 weeks, P<0.001; birth weight: 1,038.2±291.3 vs. 725.0±231.8 g, P<0.001). Apgar scores at 1 and 5 minutes were lower in the dead group than those in the survived group. Maternal PIH, antenatal steroids therapy, and histologically confirmed chorioamnionitis were similar between the two groups. RDS and surfactant re-dosing were also similar between the two groups. However, PDA was more frequent in the dead group than that in the survived group (60.4% vs. 72.2%, P=0.030) (Table 3).
Discussion
Between January 2009 and December 2018, there was no significant improvement in survival rate. The overall mortality rate of infants with GA <30 weeks was 20.8%. Mortality rate decreased from 2009 to 2012. It then increased, reaching a plateau at 20%. In 2016, mortality rates of infants with GA ≤25 weeks and GA of 26–27 weeks peaked. Among 15 infants who were dead in 2016, eight infants were dead ≤7 days after birth. Three of these eight infants were dead at delivery room and one of these eight infants was dead as soon as admission to NICU. These four infants who were dead <24 hours were delivered precipitately immediately after the mother was transferred to Busan Paik Hospital even in the emergency room or in the ambulance while the mother was transferring. Mortality rates of infants with GA of 26 weeks and 28 weeks in this study were higher than those in the KNN report of 20159 (26.5% vs. 19.2% in GA of 26 weeks, and 11.8% vs. 6.4% in GA of 28 weeks). However, mortality rates of infants with GA of 24, 25, and 29 weeks in this study were lower than those in the KNN report of 2015 (39.3% vs. 45.5% in GA of 24 weeks, 20.8% vs. 26.8% in GA of 25 weeks, 2.9% vs. 6.2% in GA of 29 weeks). The mortality rate of infants with GA of 22 weeks in this study was 80%, which was also lower than that (89.5%) in the KNN report of 2015.
Mortality rates of infants with GA ≤25 weeks were lower than those in the NICHD NRN data between 2003 and 2007 (80%, 66.7%, 39.3%, and 20.8% in this study vs. 94%, 74%, 45.4%, and 28% in the NICHD NRN data for GA of 22, 23, 24, and 25 weeks, respectively).15 On the contrary, the mortality rate of infants with GA ≥26 weeks in the NICHD NRN data was much lower than that in the present study (26.5%, 13.6%, and 11.8% in this study vs. 16.3%, 12%, and 7.7% in NICHD NRN data for GA of 26, 27, and 28 weeks, respectively). The survival of extreme preterm infants was better in our data. However, survival of infants with GA ≥26 weeks in the present study was not so good as those in other studies. This might be due to inter-center variations of resuscitation guidelines of periviable extreme preterm infants at the limit of viability such as active treatment or no intubation. Willingness to provide active treatment to these preterm infants decreases with decreasing GA.15 Among preterm infants with birth weight <400 g, 85% of those with GA of 22 weeks and 51% of those with GA of 23 weeks did not receive active resuscitation in Brumbaugh et al.'s study.16 However, only 2% of those with GA of 24 weeks did not receive active resuscitation.16
The primary mode of death in very preterm infants when medical treatment was useless was withdrawal (52.7%) or withholding (21.3%) of care compared to full resuscitation (26%).17 Withdrawal or withholding of life support discussion occurred in 27% of infants with GA of 22–24 weeks compared to only 5.6% in infant with GA of 27–28 weeks by NICHD NRN report.18 End-of-life decision is very sensitive in Korea. People are unwilling to mention it legally or ethically. Some decreased mortality rate of extreme preterm infants in this study might be due to active resuscitation in our NICU compared to NICHD NRN or other studies. The decision to provide active obstetric care and initiate active resuscitation for extreme preterm infants remains controversial. Prenatal counseling with parents is required. Death immediately after birth at delivery room despite active resuscitation was high in infants with GA of 22 weeks. However, it was rare in infants with GA ≥25 weeks. Deaths within 24 hours after birth and within 1 week after birth were high in infants with GA ≤24 weeks. Early death, especially death within 24 hours, reflects extreme immaturity. Stoll et al.15 have commented that death within 24 hours might be related to not giving active treatment to these extreme preterm infants.
Sepsis was the leading cause of death in the present study, consistent with results of other studies.1920 Preterm infants have up to ten times higher incidence of infection than term infants,21 and 22% of VLBWIs was affected by sepsis by KNN data. Streptococcus agalactiae is common in term infants, whereas Escherichia coli is common in preterm infants.21 Maternal genital tract or urinary tract infection with Escherichia coli is related to fetal loss, preterm delivery, and early neonatal death due to sepsis.22 In the present study, the most common pathogen of early onset sepsis was also Escherichia coli associated with maternal genital tract infection. In contrast, Staphylococcus was common in late onset sepsis in the present study. Coagulase-negative Staphylococcus is the most common pathogen of late onset sepsis in preterm infants, accounting for 31–54%.23 Risk factors of late onset sepsis apart from prematurity and low birth weight include prolonged use of intravenous catheter, parenteral nutrition, mechanical ventilation, and prolonged hospital stay.24
Mortality rate of sepsis is known to be high in infants with low GA: 54% in GA of 22–24 weeks, 36% in GA of 25–58 weeks, and 12% in GA of 29–33 weeks.21 Candida parapsilosis was isolated in an infant boy with GA of 23 weeks and 2 days and birth weight of 520 g. He died on the 20th postnatal day in this study. Thus, we need to be aware that fungal infection is also fatal. Fungal infection is still the third most common cause of late onset neonatal sepsis after Gram-positive sepsis and Gram-negative sepsis.25
High grade IVH (grade 3 or 4) was the second common cause of death in the present study, especially in preterm infants with GA ≤24 weeks. High grade IVH up to 7.9% of VLBWIs by KNN data can cause death or post-hemorrhagic ventricular dilatation in more than 50% of affected infants. Survivors are known to have permanent neurologic sequelae such as developmental delay and cerebral palsy.26 There is no effective treatment until now to ameliorate brain injury after IVH except mesenchymal stem cell transplantation27 which is now on phase two clinical trial. New treatment for permanent neurologic sequelae of IVH is urgently needed.
RDS and associated tension pneumothorax were main causes of early death, especially in infant with GA of 22–24 weeks, although surfactant was instilled immediately after birth.28 Pulmonary hemorrhage and PDA were also causes of early death. BPD and NEC were main causes of death after 28 days of life. Two infants died because of sudden onset of circulatory collapse. One baby born with GA of 28 weeks and 1 day (birth weight of 1,250 g) died at 10 days after birth. Another baby born with GA of 28 weeks and 3 days (birth weight of 700 g) died at 12 days after birth. There was no IVH, pulmonary hemorrhage, PDA, anemia, or sepsis to cause hypotension. Sudden onset hypotension occurred. It was refractory to volume expander and inotropes. It seems to be late-onset circulatory collapse (LCC) related to relative adrenal insufficiency which is not well-known or widely accepted yet.29 This new entity of LCC causes periventricular leukomalacia, an independent risk factor for cerebral palsy.30
In Korea, the survival rate of preterm infants has increased significantly. The survival rate of VLBWIs in Korea was significantly low in the past. It was 33.8% in the 1960s, 49.2% in the 1980s, 65.8% in the early 1990s, 77.5% in 2002, 85.7% in 2009, and 86.4% in 2015.79 Recently, it seems to have no more significant improvement. The survival rate of VLBWIs in NICHD NRN was 85% between 1997 and 2002, having no more significant improvement except for the NRNJ data (89.2% in 2003 and 91.3% in 2008).2 The International Network for Evaluating Outcomes of Neonates (iNeo) collaborated with 10 national and regional neonatal networks reported that the survival rate of infants with GA of 24–29 weeks was 87.4% between 2007 and 2013.31 It was higher than that (79.2%) in the present study. However, this study included infants having GA of 22–23 weeks who had the highest rate of mortality. The survival rate of infants with GA of 24–29 weeks was the highest in Japan: 93.3% by NRNJ, 89.0% by ANZNN, 87.0% by SwissNeoNet, 79.9% by INN, 78.1% by Spanish Neonatal Network (SEN1500), and so on. There were wide inter-network variations.
Delivery with appropriate supports of neonatal resuscitation team and sufficient maternal obstetric care, especially maternal infection control, are potentially modifiable factors that can decrease asphyxia and early onset neonatal sepsis, thus decreasing mortality rate. In addition, pregnancy should continue with sufficient maternal care. We can reduce late onset sepsis by reducing risk factors such as prolonged use of central venous catheter, parenteral nutrition, and mechanical ventilation. Mortality due to LCC can be controlled by exogenous glucocorticoid if we can recognize it early. New treatment for IVH such as mesenchymal stem cell transplantation is being studied. Mortality due to high grade IVH could be somewhat controlled in the near future.
In conclusion, mortality rate did not decrease over ten years (January 2009 to December 2018) in this study. We can't help the birth of extreme prematurity. However, there are modifiable factors to reduce mortality, especially immediate postnatal death of extreme preterm infants. Increasing survival without major morbidities, besides decreasing mortality is another important task.



 XML Download
XML Download