

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Uterine rupture in pregnancy is defined as complete separation of the wall and serosa of the pregnant uterus. It is one of the most life-threatening complications leading to massive hemorrhage, shock, and even fetal and maternal mortality. Although it may occur spontaneously without scarred uterus, the most common cause of uterine rupture is the presence of scar tissue including previous myomectomy and cesarean delivery.
The risk of uterine rupture in pregnancy after myomectomy is around 0.75–1% according to approach methods.12 Although the incidence is very low, it is associated with fatal complications to both mother and fetus, suggesting that myomectomy in reproductive patients should be carefully assessed and performed. Almost all cases of uterine rupture after myomectomy occurred in the third trimester or labor.3 Because uterine rupture in the first trimester is very rare condition, massive bleeding and serious complications could occur by failing to diagnose uterine rupture in early pregnancy with abdominal pain. So, it is important to keep in mind that uterine rupture could happen in women with surgical history of myomectomy. We present a rare case of recurrent uterine rupture in the first trimester after laparoscopic myomectomy, and discuss operative strategies to prevent uterine rupture following pregnancy after laparoscopic myomectomy.
Case
A 36-year-old primigravida pregnant woman at 10 weeks and 3 days of gestation, was transferred to the emergency department of Dongguk University Ilsan Hospital due to severe abdominal pain and diarrhea with vaginal bleeding. The patient had a history of laparoscopic myomectomy for 5 cm sized intramural myoma involving the fundus before 3 years. Approximately 7 months after the operation (laparoscopic myomectomy), she was pregnant. However, at 7 weeks of gestation, spontaneous uterine rupture occurred around left side of fundus, and was repaired by laparoscopic approach at another institution. After 2 years, she was pregnant and received regular antenatal care before she was transferred to Dongguk University Ilsan Hospital.
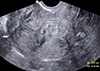
Physical examination revealed that blood pressure was 99/49 mmHg and the heart rate was 105 beats per min. Whole abdomen tenderness and rebound tenderness was observed. Transvaginal ultrasonography was performed and no gestational sac with hyperechoic lesion was observed within the uterine cavity (Fig. 1).
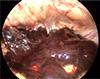
Based on clinical manifestation with surgical history, uterine rupture was suspected. An emergency diagnostic laparoscopy was performed immediately with informed consent. Intraoperative findings revealed about 1,000 mL blood in the abdominal cavity with active bleeding from the perforated myometrium near the fundus (Fig. 2). Owing to the difficulty of laparoscopic approach to uterine rupture site and adherent mesentery, the operation was converted to laparotomy. During exploration, the anterior wall of uterus near to fundal area was perforated about 3 cm in diameter and there were protruding conceptive tissues in rupture site (Fig. 3). The protruding conceptive tissues were gently removed, and the myometrium was repaired by double-layer closure and serosa was repaired finally, resulting in a total repair of three layers. Five units of packed red blood cells were transfused, and the postoperative course was uneventful. Histopathological examination was confirmed by the production of conception tissues with endometrium.
Discussion
As the number of women undergoing myomectomy has increased in recent years following treatment for infertility and increased the average maternal age at childbirth, the number of pregnant women with a history of myomectomy is growing in the obstetric care unit. As pregnancy after myomectomy may increase the risk of uterine rupture,4 the physician should evaluate the risks and complications in the reproductive patient with myoma.5
In our patient, spontaneous uterine rupture occurred twice in the first trimester at 7 weeks and 10 weeks of gestational age. It was a very rare condition because uterine rupture typically occurs during active labor or in third trimester.3 The potential causes of uterine rupture in early pregnancy in the present case include laparoscopic uterine surgery twice for myomectomy and uterine wall repair surgery for first uterine rupture, and the interval between myomectomy and pregnancy was not enough for complete wound healing.
Uterine rupture after laparoscopic surgery generally occurs due to failure to meticulously close the myometrial bed, poor hemostasis with subsequent hematoma formation or excessive use of monopolar or bipolar electrosurgery, devascularization of the myometrium by thermal damage.6 In addition, the opening of the uterine cavity, the extent of local tissue destruction, development of infection, and single-layer sutures are risk factors for uterine rupture.7
Several studies suggest operative strategies to reduce uterine rupture in subsequent pregnancies. First, women with myomectomy carry a higher risk of uterine rupture in subsequent pregnancy, even after removal of superficial sub-serosal myomas.2 The physician should consider the benefits and complications of myomectomy in a reproductive patient depending on the site and size of myomas. Second, multilayer uterine closure of myometrial bed and avoidance of entry into the endometrial cavity are also recommended.268 Because a multilayer repair can improve the strength of the wound and decrease the risk of postoperative hematoma formation, which can also interfere with optimal tissue healing.9 Based on systemic review, there is no significant difference between the incidences of uterine rupture during pregnancy following laparoscopic versus an open myomectomy (1.2% vs. 0.4%, P=0.119).10 Therefore, regardless of surgical approach, multilayered closure of the myometrium is recommended. Third, during laparoscopic myomectomy, excessive monopolar or bipolar coagulation for hemostasis should be avoided because it reduces vascularization and interferes with wound remodeling. Laparoscopic electrolysis is one of minimal invasive surgery that blood supply of uterine myoma was blocked by electrocauterization and the procedure results in shrunken myoma instead of complete excision.11 However, in spite of the benefits, devascularization itself is one of the predisposing factors for healing because of poor vascularity of uterine muscles and destroying blood supply is a risk factor for wound healing even unscarred uterus.12 The new technology for myoma, targeted volumetric thermal ablation such as radiofrequency fibroid ablation, magnetic resonance-guided focused ultrasonography surgery or high intensity focused ultrasonography are related with coagulative necrosis on the uterus. These changes may affect implantation, placentation, and uterine contractility during labor, thus increasing the risk of uterine rupture.13 As we mentioned, the incidence of uterine rupture is variable ranges at literatures and 0.03–0.08% of uterine rupture was revealed in women with unscarred uterus.1014 It commonly occurs for women with past history of uterine surgery without a scar.15 Therefore, minimal coagulation and avoiding poor vascularity may contribute to preserve the integrity of uterine myometrium.
Although the incidence of unscarred uterine rupture is not frequent, uterine rupture in any pregnancy after laparoscopic procedures is increasing. In addition, adequate interval between myomectomy and pregnancy reduces uterine rupture. Although there is no guideline about safe interval, a few studies recommend 12 to 24 months to decrease the complications of pregnancy after myomectomy.161718 It is important to balance between uterine wound healing and reproductive outcomes. A study of uterine wound healing using magnetic resonance imaging reported that the uterine healing process was complete at 12 weeks after abdominal myomectomy in the absence of hematoma or edema formation in the myometrium.17 Another study with 471 patients, the average interval in the live birth group was much shorter than in the non-live birth group (15.0±8.4 months vs. 18.9±9.3 months, P=0.005).19 This indicates that a longer interval may not get better reproductive outcomes, but adequate interval should be considered.
In conclusion, as the wide use of laparoscopic procedures like myomectomy and electromyolysis with remarkable benefits, careful selection of patients and accurate surgical procedure by a surgeon proficient in laparoscopy is essential. Also, it should be accompanied with informed consent about complications because the uterine rupture is a fatal condition and the consequence is irreversible. Therefore, when considering laparoscopic procedures for myoma in reproductive-age women, strict selection criteria for surgical indications and intraoperative strategies to reduce uterine rupture in subsequent pregnancies are highly recommended.

 XML Download
XML Download