

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypertriglyceridemia is defined as a high triglyceride (TG) level in the blood and is considered one of the main components of metabolic syndrome (MetS), along with abdominal obesity, insulin resistance, high blood pressure, and a low high-density lipoprotein-cholesterol (HDL-C) level. All these components contribute to the risk of cardiovascular disease (CVD) [12]. CVD, which is increasing in prevalence, is considered one of the leading causes of death globally and the mortality rate of stroke patients in the Asian populations is higher than those in the Western populations [3]. In Korea, the prevalence of hypertriglyceridemia has greatly increased, from 10.2% in 1998 to 16.4% in 2017, and the prevalence is greater in men (25.2%) than in women (8.0%) [4].
Low-density lipoprotein-cholesterol (LDL-C) regulation is a major consideration in CVD treatment, and hypertriglyceridemia is also considered a major target of CVD treatment [5678]. An independent association of a high TG level with increased CVD risk has been reported in large-scale epidemiological studies [910]. Of particular note, hypertriglyceridemia may be a more important risk factor for CVD in Asian populations than in other populations, as race specificity of the disease has been reporeted [111213].
East Asians consume fewer dairy products than Westerners. Central Latin Americans are reported to drink 1.3 servings of milk per day [14] and the average daily milk intake in Swedish cohort was 290 g for men and 240 g for women [15]. According to the 2017 Korea National Food and Nutrition Statistics Report, the daily intake of milk and yogurt for adults aged 19 to 64 years was 58.8 g and 15.3 g, respectively [16].
Although recent meta-analyses of prospective cohort studies reported that dairy product intake may prevent MetS [17] and CVD [18], the beneficial effects of dairy products on MetS and CVD remain controversial because milk contains saturated fats [19]. Inconsistent results have been reported worldwide about the effects of dairy products consumption on chronic diseases such as diabetes, CVD, and MetS, and it has been shown that the effects vary by race, dietary pattern [20212223], dairy product consumption rate [242526], gender, and obesity [272829]. Hypertriglyceridemia is a component of MetS and may lead to CVD, but the association between hypertriglyceridemia and dairy product consumption has not been fully described in Asian populations with a relatively low intake of dairy products. Therefore, we evaluated the associations between the intake of dairy products (milk and yogurt) and hypertriglyceridemia according to gender and obesity status using data from the Korea National Health and Nutrition Examination Survey (KNHANES).
Go to : 
SUBJECTS AND METHODS
Subjects
This study used data from the KNHANES IV and V survey (2007–2012) that were conducted by the Ministry of Health and Welfare and the Korea Centers for Disease Control and Prevention (KCDC). The survey consisted of three components: a health examination, a health interview, and a nutrition survey conducted by highly trained experts. The integrated KNHANES IV and V data include information on 50,405 individuals. Participants under 18 or over 65 years old (n = 20,722) and pregnant women (n = 214) were excluded from our analyses to avoid bias. Participants who did not have dietary intake records (n = 3,945) or food frequency questionnaire (FFQ) data pertaining to dairy product intake (n = 548) or who had extreme caloric intakes (< 500 or > 5,000 kcal/day) (n = 384) were also excluded [30]. Additionally, participants who had previously been diagnosed with dyslipidemia by a physician or who were taking medication for dyslipidemia (n = 1,756) were excluded, as such patients may have biased the intake data. Finally, data for 22,836 participants were included in this study.
This study was conducted in accordance with the Ethical Principles for Medical Research Involving Human Subjects by the Helsinki Declaration. No requirement for institutional review board (IRB) review was needed for this study since the KNHANES data are publicly available online. The original KNHANES was approved by the IRB of KCDC (IRB approvals: 2007-02CON-04-P, 2008-04EXP-01-C, 2009-01CON-03-2C, 2010-02CON-21-C, 2011-02CON-06-C, and 2012-01EXP-01-2C).
Dairy product and nutrient intakes
Data from the validated FFQ were used to determine the frequency of dairy product intake. Dairy products were categorized as either milk or yogurt. The yogurt category included liquid and semi-solid yogurts. As cheese intake is very low in Korea, it was not included in the FFQ [23]. For analysis, the dairy product intake frequency data were categorized as < 1 time/month, ≥ 1 time/month - ≤ 1 time/week, > 1 time/week - <1 time/day, or ≥ 1 time/day [23]. The 24-hour recall data were used to assess food and nutrient intakes.
Definition of hypertriglyceridemia and Covariates
Among participants who were not diagnosed or recognized with hypertriglyceridemia, participants with a fasting TG level > 200 mg/dL in the health examination were considered to have hypertriglyceridemia [5]. We considered sex, age, income (household monthly income), education, smoking status, alcohol consumption, regular physical activity, menopause (women only), total energy intake, carbohydrate intake, and fiber intake as potential confounding factors. Participants were grouped into four age categories: 18–21, 22–29, 30–49, or 50–64 years. Levels of household income (lowest, low, high, and highest) and education (0–6, 7–9, 10–12, and ≥ 13 years) were obtained from a well-designed questionnaire. Smoking status was dichotomized as current smoker and non-smoker (including previous smokers and individuals who have never smoked). Alcohol consumption was categorized as yes (≥ 1 serving/month) or no (< 1 serving/month, including no alcohol consumption). Regular physical activity was classified as yes (including regular walking, moderate activity, and vigorous activity) or no exercise. Menopause status was also dichotomized as yes (menopause including natural and surgical menopause) or not (non-menopausal including premenstrual, menstrual, and breast-feeding).
Statistical analysis
The general characteristics of the participants are described as percentages or means ± standard error (SE). Chi-squared tests were performed for analyzing categorical variables and generalized linear models (GLM) were used for continuous variables. Logistic regression was used to assess the association between dairy product intake and the prevalence of hypertriglyceridemia as follows: 1) age and gender adjusted analyses, and 2) multivariable adjusted analyses including adjustments for gender, age, household income, education, smoking, alcohol drinking, regular physical activity, menopause status (for women only), body mass index (BMI), total energy intake, total carbohydrate intake, and total fiber intake. Furthermore, gender and BMI (obesity: BMI ≥ 25 kg/m2, normal: BMI < 25 kg/m2) stratified analyses were performed. A P-value < 0.05 represented statistical significance in all tests. All statistical analyses were carried out using IBM SPSS Statistics software (ver. 20.0; IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
General characteristics of subjects
The general characteristics of the participants according to the frequency of dairy products consumption are shown in Table 1. Participants who frequently consumed dairy products (≥ 1 time/day) were significantly more likely to be women aged 30–49 years, non-smokers, alcohol drinkers, have the highest income, and a high level of education. BMI, total energy, protein, fat, and calcium intake all showed significant differences across the four categories of dairy product consumption frequency, but there were no differences in total carbohydrate or total fiber intakes by dairy product consumption frequency.
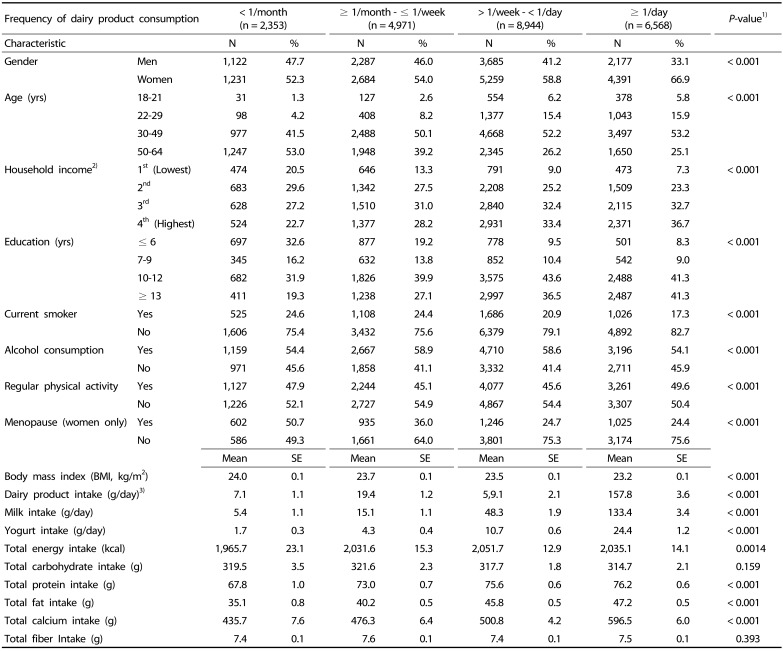
Table 1
General characteristics of subjects according to the frequency of dairy product consumption
1)P-values were derived from generalized linear models (GLM) for continuous variables and Chi-squared tests for categorical variables.
2)Household income levels were calculated by equivalizing gross household income per month in each year.
3)Dairy product intake was calculated as a combination of milk intake and yogurt intake (both liquid and semisolid yogurt).
![]()
Association between hypertriglyceridemia and dairy product intakes among all subjects
Regarding the association between dairy product consumption and hypertriglyceridemia, a significantly decreased odds ratio (OR) was obtained for the highest dairy product intake frequency group (≥ 1 time/day) compared to that for the lowest dairy product intake frequency group when assessed by using a multivariable-adjusted model (OR = 0.79; 95% CI: 0.64–0.97, P for trend = 0.022) (Table 2). In the group with the highest milk consumption frequency (≥ 1 time/day), similar pattern was observed; a significant decrease in the risk of hypertriglyceridemia when using the multivariable-adjusted model (OR = 0.79; 95% CI: 0.66–0.95, P for trend = 0.088). However, the multivariable-adjusted model did not detect a significant risk associated with yogurt intake.
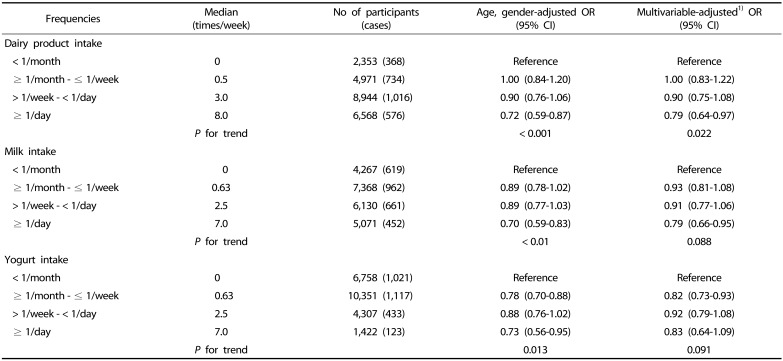
Table 2
Odds ratios (ORs) and 95% confidence intervals (Cls) for hypertriglyceridemia by milk, yogurt, and dairy product consumption frequencies among all participants
![]()
Association between hypertriglyceridemia and dairy product consumption by gender
Compared to the lowest dairy product intake group, the OR for hypertriglyceridemia was lowest in the highest dairy product intake group for both men and women when applying the age-adjusted model (men, OR = 0.74; 95% CI: 0.59–0.92, P for trend = 0.002; women, OR = 0.68; 95% CI: 0.49–0.94, P for trend = 0.045) (Table 3). These associations remained significant in the results of the multivariable-adjusted model for men (OR = 0.76; 95% CI: 0.60–0.97, P for trend = 0.024) but the significance disappeared for women. A significant inverse association with elevated TG was detected in the highest milk intake group (≥ 1 time/day) for men (OR = 0.71; 95% CI: 0.56–0.89, P for trend = 0.025), but there was no significance for the association in women. Furthermore, there were no significant associations between yogurt intake and hypertriglyceridemia in men or women.
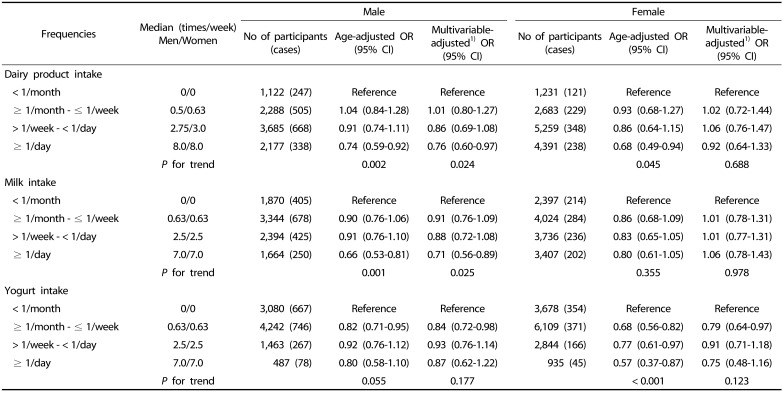
Table 3
Odds ratios (ORs) and 95% confidence intervals (Cls) for hypertriglyceridemia by milk, yogurt, and dairy product consumption frequencies for male and female subjects
![]()
Association between hypertriglyceridemia and dairy product consumption in obese men and women
When assessing the effects of both gender and obesity status, the risk of hypertriglyceridemia was lowest in the highest milk intake group (≥ 1 time/day) of obese men (OR = 0.64; 95% CI: 0.46–0.91, P for trend = 0.036) (Table 4). Among the obese women, the risk of hypertriglyceridemia was significantly low in the group with the highest frequency of yogurt consumption (OR = 0.53; 95% CI: 0.29–0.94, P for trend = 0.019). However, the risk of hypertriglyceridemia in the highest milk consumption group of normal-weight men was not significantly different from that in the lowest milk consumption group (OR = 0.73; 95% CI: 0.40–1.32, P for trend = 0.414). In addition, there was no association between yogurt intake and the risk of hypertriglyceridemia among the normal-weight women (OR = 0.94; 95% CI: 0.51–1.72, P for trend = 0.902).
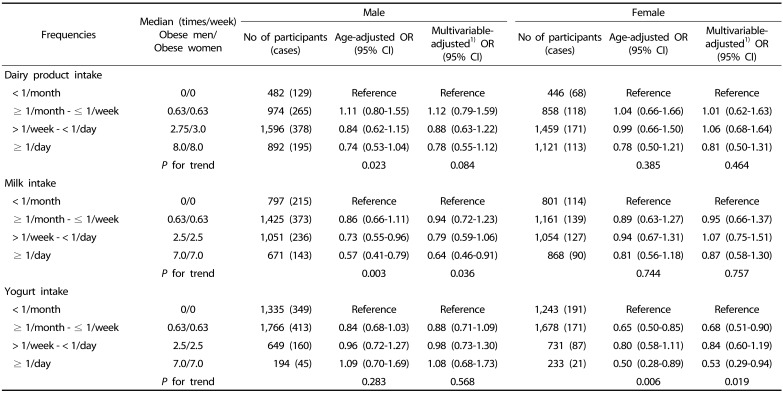
Table 4
Odds ratios (ORs) and 95% confidence intervals (Cls) for hypertriglyceridemia by milk, yogurt, and dairy product consumption frequencies in obese (BMI ≥ 25kg/m2) male and female subjects
![]()
Go to :
DISCUSSION
In this study, we observed the association between dairy product intake level and the presence of hypertriglyceridemia in Korean adults. The analysis showed that the total dairy product intake (milk and yogurt) was negatively associated with the prevalence of hypertriglyceridemia in Korean adults. High intakes of dairy product and milk specifically, significantly reduced the risk of hypertriglyceridemia, but only in men. In addition, a negative association between milk consumption and hypertriglyceridemia was observed in obese men and a negative association between yogurt consumption and hypertriglyceridemia was observed in obese women.
Recent studies have reported inverse associations between dairy product consumption and CVD [2731], CHD [32], and MetS [283334], but some studies have reported that the intake of milk may increase the risk of CVD, CHD, and stroke due to milk's fat content [2635]. These inconsistent results appear to be due to dairy products being not only rich in saturated fat, but also rich in minerals and vitamins that have beneficial effects on health [36]. Among the various components of milk and dairy products, conjugated linoleic acid, whey protein, and calcium are known to have beneficial effects on obesity [2337] and CVD [3038]. According to Zemel et al. [39], a high calcium diet can suppress the 1,25-dihydroxyvitamin D3 level, reduce intracellular Ca2+ in adipocyte cells, suppress lipogenesis, and promote lipolysis. In addition, the effects of calcium from dairy sources on weight and fat loss are greater than those of supplemental calcium carbonate [4041]. Moreover, a high calcium intake can reduce fatty acid synthase (FAS) mRNA expression and serum triglycerides [42].
The effects of dairy product intake on CVD, CHD, and MetS has also been shown to depend on gender and obesity status. A lower intake of dairy products was reported to increase the risk of death from CVD in Japanese women but not in Japanese men [27]. A high milk and dairy product consumption have reduced the prevalence of MetS in UK men [28]. Also, the relationship between dairy products and changes in weight and waist circumstance (WC) differed by gender and body weight status [29]. In addition, a large cohort study conducted in Korea reported that calcium intake was inversely correlated with WC and hyperglycemia in women and with hypertriglyceridemia in men [43].
The dietary factors related to hypertriglyceridemia vary by gender. In men, excessive intake of beef and alcohol is significantly associated with hypertriglyceridemia, whereas, high intakes of fast food and rice are associated with hypertriglyceridemia in women [44]. In the United States, a carbohydraterich diet (> 59.1% of total energy from carbohydrates) has been associated with high serum TG levels in women [45]. Also, women in Korea who obtain more than 70% of their total energy from carbohydrates are at high risk for diabetes and hypertriglyceridemia [46].
A previous study used KNHANES III data to calculate the risk associated with MetS components according to milk intake levels and revealed protective effects of high milk consumption on TG and HDL-cholesterol levels in subjects with a BMI ≥ 23 kg/m2; nonetheless, there was no significant association detected in normal-weight subjects. However, this study did not evaluate the effect of gender on the associations between milk and MetS components [34]. Similarly, in the Coronary Artery Risk Development in Young Adults (CARDIA) study, more frequent consumption of dairy products was associated with a reduced risk of dyslipidemia in obese adults in the US (P for trend < 0.01); however, the same association was not detected in normal-weight adults [22]. These results suggest a stronger beneficial effect of dairy product consumption on elevated TG level in overweight or obese individuals than in normal individuals. It is unclear why high dairy product consumption is associated with lowering the risk of hypertriglyceridemia in obese people only.
Our study showed an inverse association between yogurt consumption and hypertriglyceridemia in obese women. A previous study using US National Health and Nutrition Examination Survey (NHANES) data showed that yogurt consumption was associated with better metabolic outcomes, including an increased HDL-C level, in women (32.8% of the women were obese, BMI ≥ 30) [37]. This type of gender difference in the association between dairy product consumption and hypertriglyceridemia has not been fully explained. A possible explanation for the inverse association between yogurt consumption and hypertriglyceridemia in obese women may be related to the composition of the intestinal microbiota. Yogurt generally contains commensal microbiota such as Bifidobacterium and Lactobacillus [47]. In one study, after yogurt consumption, female subjects had as higher total bacterial, especially Bifidobacterium content than male subjects [48]. Intestinal microbiomes have been shown to produce short-chain fatty acids (SCFAs) and conjugated linoleic acid (CLA) from dietary fiber and polyunsaturated fatty acid (PUFA). Such acids interact with peroxisome proliferator-activated receptors (PPARs) and have been associated with a higher TG level very low density lipid (VLDL) clearance, and higher lipolysis [49].
From the standpoint of public health in Asia, this study is of great value because it directly investigated the dairy product intake and hypertriglyceridemia relationship based on gender and obesity status. Dairy products provide multiple types of nutrients in a comparatively easy-to-consume form compared with other foods, and they can have a beneficial role in attenuating the development of hypertriglyceridemia, although the underlying mechanisms remain unclear. This study was based on well-validated, nationally representative data on the Koreans populations, and it controlled for possible changes in eating habits by excluding participants who were diagnosed with dyslipidemia, or who had taken medication for disease treatment, thereby reducing possible sources of bias.
However, as the present study was observational and crosssectional in nature, residual confounding factors could not be ruled out; therefore, a causal relationship between dairy product intake and hypertriglyceridemia cannot be inferred. In addition, the differential effects of high- and low-fat dairy product consumption on hypertriglyceridemia could not be examined; disparities in the dietary intake of high- and low-fat dairy products across several ethnicities should be studied.
In conclusion, the association between dairy product intake and hypertriglyceridemia may differ according to gender, obesity status and type of dairy products. Frequent consumption of dairy products was shown to be associated with a reduced prevalence of hypertriglyceridemia. In particular, milk consumption was inversely associated with hypertriglyceridemia in obese men and frequent yogurt intake had similar effects in obese women. Further prospective studies and clinical trials are needed to validate these findings and elucidate the underlying mechanisms.
Go to :
 XML Download
XML Download