

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Ovarian cancer is the most lethal form of gynecologic cancer. In 2019, the American Cancer Society estimated 22,530 new ovarian cancer cases and 13,980 ovarian cancer deaths [1]. The management of ovarian cancer has been evolving with the introduction of new drugs and surgical innovation.
Patients with advanced-stage ovarian cancer traditionally underwent surgery upfront with maximal cytoreductive surgery via laparotomy (open surgery) followed by adjuvant platinum-based chemotherapy. A recently emerging approach involves neo-adjuvant chemotherapy followed by interval tumor debulking. Phase III clinical trials showed similar progression-free and overall survival rates for this emerging modality, but surgery following neo-adjuvant chemotherapy features lower morbidity and mortality rates than the traditional method [2345]. Current guidelines endorse neo-adjuvant chemotherapy as an option for some patients [6]. The ultimate goal is to achieve complete cytoreductive surgery, which has been shown to improve survival [789].
The morbidity and surgical complexity associated with interval cytoreductive surgery appears lower than that with surgery upfront [2410]. As a result, patients and gynecologic oncologists may be inclined to use the minimally invasive approach to achieve similar oncologic outcomes as laparotomy. Furthermore, patients with significant comorbidities and elderly patients may decline to undergo laparotomy. The benefits of minimally invasive surgery over laparotomy are reduced blood loss, reduced post-operative pain, a smaller incision with a reduced risk of wound infection, a shorter hospital stay, a faster recovery, and a shorter time to resuming chemotherapy after interval cytoreductive surgery.
Phase III trials that compare standard laparotomy with minimally invasive surgery for ovarian cancer after neo-adjuvant chemotherapy are lacking. Oncologic outcomes have been reported from the National Cancer Database [11]. A phase II clinical trial by Gueli Alletti et al. [12] of 30 patients demonstrated that minimally invasive surgery is safe and feasible in ovarian cancer patients with complete clinical response to neo-adjuvant chemotherapy. Furthermore, the latest version of the National Comprehensive Cancer Network's guidelines for ovarian cancer considers that there may be a role for minimally invasive surgery in ovarian cancer. Patients who are unable to be optimally debulked using minimally invasive techniques should be converted to an open procedure performed by an experienced surgeon [13].
Surgical innovation is important, as are outcomes, but complex [1415]. Robotic-assisted surgery has technological differences with laparoscopy, such as 3-dimensional optics, improved depth perception, camera stability, increased dexterity, and tremor filtration. Furthermore, the latest robotic platform Xi (Intuitive Surgical, Inc., Sunnyvale, CA, USA) allows pelvic and upper abdominal surgery with simple maneuvers. Very limited data are available with this new platform in ovarian cancer. This study aimed to assess complete cytoreductive surgery and perioperative outcomes with the robotic platform Xi in advanced-stage ovarian cancer patients after neo-adjuvant chemotherapy.
Materials and methods
1. Objective
The primary objective of the study was to assess the feasibility of robotic-assisted interval cytoreductive surgery for patients with advanced ovarian cancer after neo-adjuvant chemotherapy. The secondary objective was to examine perioperative outcomes.
2. Eligibility criteria
Patients with biopsy-proven stage IIIC or IV ovarian, fallopian tube, and primary peritoneal carcinoma with a clinical response to neo-adjuvant chemotherapy who would also undergo interval cytoreductive surgery with robotic assistance were included in this study. The minimum follow-up duration after surgery was 60 days. Patients with clinical early-stage cancer (I to IIIB), primary debulking surgery, and secondary cytoreductive surgery were excluded. Patients with resolution of ascites, pleural effusion, significant decrease of cancer antigen 125 (CA-125), decrease of tumor burden on computed tomography (CT) or a positron emission tomography/CT scan, and partial or complete response to chemotherapy by response evaluation criteria in solid tumors (RECIST) criteria after neo-adjuvant chemotherapy underwent diagnostic laparoscopy. Patients underwent robotic-assisted surgery if the diagnostic laparoscopy showed potential complete cytoreductive surgery. Study criteria were based on those of the randomized controlled trial by Rutten et al. [16]. All eligible patients identified during the study period were included.
3. Data extraction
Data were abstracted from the patients' electronic medical records in Epic (Epic Systems Corporation, Verona, WI, USA). The variables were: age, comorbid conditions (hypertension, diabetes, chronic obstructive pulmonary disease, asthma, and coronary artery disease), prior abdominopelvic surgery, body mass index (BMI), American Society of Anesthesiologists (ASA) score, RECIST tumor response, CA-125 at the time of diagnosis and pre-operatively, chemotherapy, breast cancer gene status, tumor histology and grade, operative time, blood loss, transfusion, length of hospital stay, complication, readmission, surgical procedure, complexity score, and pathology. Chemotherapy response score was assessed by a pathologist (AE) during the review of a single omental tissue block with the least response to chemotherapy as per the recent recommended guidelines [17].
The surgical approach for robotic-assisted surgery followed the standard approach described in the National Comprehensive Cancer Network's 2019 guidelines [13]. Pre- and post-operative care were performed according to enhanced recovery after surgery protocols [1819]. To define case complexity, we used the surgical complexity scoring system described by Aletti et al. [20]. The da Vinci Xi robotic platform was used. Port placement was described by Lucidi et al. [21].
Complete cytoreductive surgery was defined as no gross residual disease at the end of surgery, optimal cytoreductive surgery was defined as no residual disease measuring greater than 1 cm, and sub-optimal cytoreductive surgery was defined as residual disease measuring greater than 1 cm.
4. Data analysis
Categorical variables are presented as number of cases and percentages. Continuous variables are presented as median, mean, standard deviation, range, and 95% confidence interval (CI). For categorical variables, the χ2 test and Fisher's exact test were used. The data analysis was performed using SPSS Statistics version 25 (SPSS Inc., Chicago, IL, USA).
Results
During the study period, 12 patients met the inclusion criteria and were included in the study. The median follow-up was 9.5 months (95% CI, 6.19–13.31). Three patients in the robotic group underwent diagnostic laparoscopy upon receiving the initial diagnosis. The criteria for neo-adjuvant chemotherapy included a low likelihood of optimal cytoreduction on diagnostic laparoscopy (3/12), stage IV disease (3/12), tumor in porta hepatis on a CT scan (1/12), unresectable tumor upon exploratory laparotomy (1/12), acute venous thromboembolism upon diagnosis (2/12), and patient declining surgery up front (1/12) (Supplementary Table 1).
Patient demographics are presented in Table 1. Median age was 72.5 years, median BMI was 23.35 kg/m2 (17.53–41.28), and all patients had an ASA score of 3. Perioperative outcomes are presented in Table 2. The estimated mean blood loss was 100 mL (50–800 mL). Pre- and post-operative changes in hemoglobin were 1.5±0.5 (95% CI, 1–1.7). Patients spent a median 2 days in the hospital. The 30-day post-operative complication and readmission rate was 8.3% (1 patient). Complexity scores of surgical procedures performed is in Supplementary Table 2.
Table 1
Patient demographics
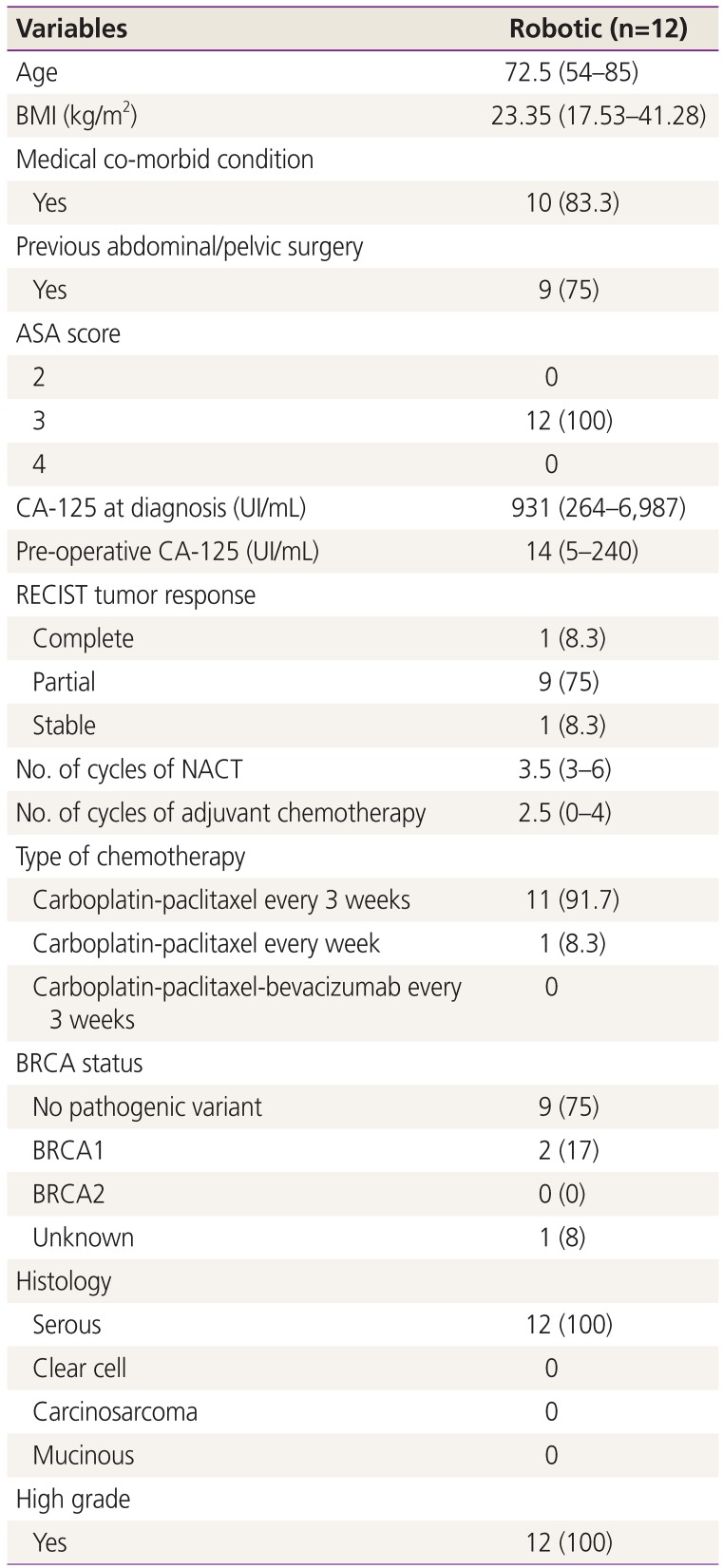
Table 2
Perioperative outcomes
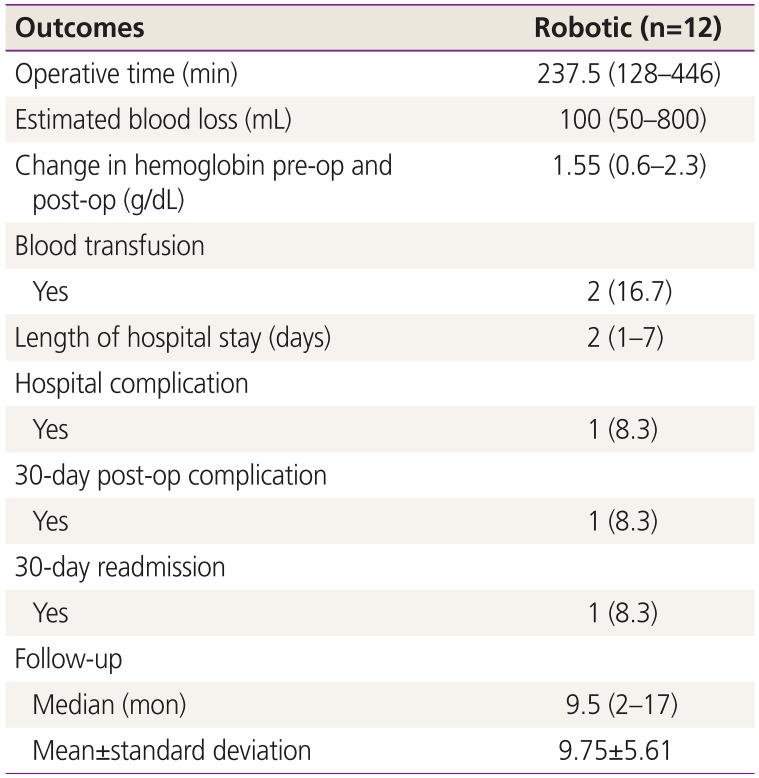
One patient required a post-operative blood transfusion. One patient was readmitted with bacteremia. Another patient required surgery due to port site hernia on post-operative day 31. The patient was admitted and underwent laparoscopic surgery at an outside hospital. The port site hernia was induced by the 12-mm assistant port. As a result of that event, institutional practice changed to close the assistant port with 0-vicryl suture. It is possible that the port size was extended due to the abdominopelvic surgery.
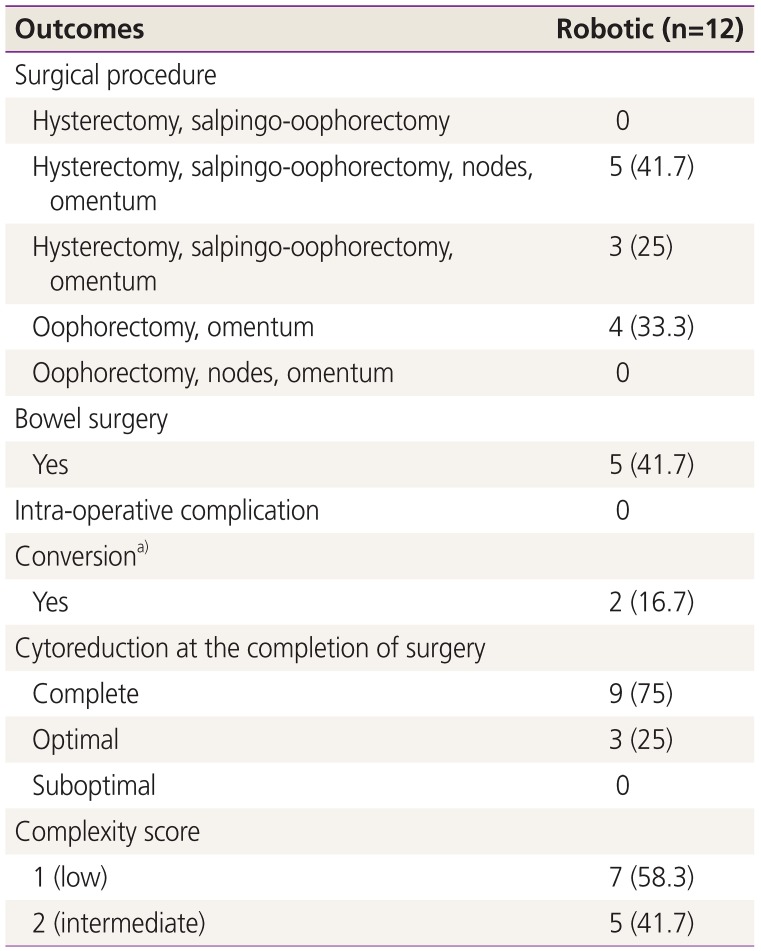
Optimal cytoreductive surgery was achieved in 100% of patients; including optimal but not complete cytoreduction in 3 (25%) (Table 3). Complete cytoreduction was achieved in 9 cases (75%), with no gross residual disease. Two robotic cases required supra-umbilical laparotomy to achieve optimal cytoreduction. In both cases, the pelvic surgery was performed using the Xi robotic platform. One case required a transverse colon resection and partial gastrectomy, while the other required small bowel resection. The other 3 cases did not require laparotomy; rather, one each required partial transverse colon resection, partial cecal resection with appendectomy, and appendectomy (Supplementary Table 3).
Table 3
Surgical outcomes
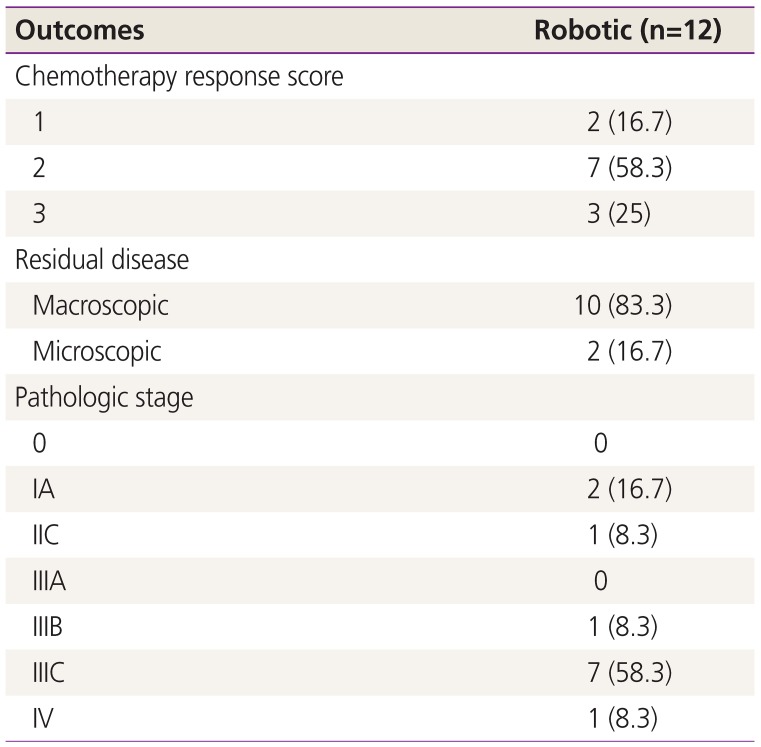
The abstracted data did not provide a standardized and objective confirmation of complete resection. However, all patients underwent a CT scan at 2–20 weeks post-operative (median, 8 weeks; 95% CI, 5.61–12.06). All cases show no measurable disease. One case showed ascites. All patients underwent CA-125 testing at 4 weeks post-operative. Eleven of 12 patients had normal levels. One patient had a pre-operative CA-125 level of 240 U/mL and a 4 weeks post-operative level of 84 U/mL (Supplementary Table 3). Patients received a median of 2.5 cycles of adjuvant platinum-based chemotherapy (95% CI, 0.89–2.95; range, 0–4). One patient declined adjuvant chemotherapy. Two patients received 6 cycles of neo-adjuvant chemotherapy and 0 after surgery (Supplementary Table 2).
The pathologic findings showed that 83% of patients had a positive response, with chemotherapy response scores of 2 and 3 (Table 4). With a median follow-up of 9.5 months, 92% of the patients remained alive (Table 5). Three patients underwent lymph node dissection due to abnormal findings during surgery or CT scan findings (Supplementary Table 3). One case had a 2-mm metastatic focus of carcinoma in a left pelvic lymph node. In another case, 2 pelvic nodes failed to reveal any carcinoma. In another case, 5 lymph nodes were removed; 1 of them included a 0.35-mm metastatic serous carcinoma. The most common location of disease recurrence was the peritoneum (4/12), followed by lymph nodes in the abdomen and pelvis (1/12) and chest (1/12) (Supplementary Table 3).
Discussion
The surgical approach for interval cytoreduction in ovarian cancer patients is evolving. Our preliminary data showed that complete cytoreductive surgery is feasible (75%) and may be an alternative approach for some patients.
Robotic-assisted surgery for ovarian cancer was previously described but without a focus on interval cytoreductive surgery [222324]. Our data are among the first to address the role of robotic surgery using the da Vinci Xi platform and overcomes the limitations of previous publications based on an older platform. We believe this is relevant since the neo-adjuvant chemotherapy rate has increased.
The robotic approach may be an additional tool for achieving complete cytoreduction. Our preliminary data are consistent with published data that included mainly laparoscopic cytoreductive surgery (74.50%; 95% CI, 40.41–97.65) [11122526272829]. Although phase III trials demonstrated that interval cytoreductive surgery is less invasive and required fewer surgeries than debulking upfront, adequate exposure, identification of tumors in the upper abdomen, and removal of residual disease are critical [24].
The feasibility of performing complex and widespread surgery, such as bowel and stomach resection, diaphragm stripping, splenectomy, and pelvic and para-aortic node dissection, may be limited for minimally invasive surgery. Our 2 robotic cases that required supra-umbilical laparotomy were due to the presence of a tumor in the upper abdomen that required bowel resection, while 1 case required transverse colon and partial stomach resection. Brown et al. [30] reported a 17% conversion rate to achieve optimal cytoreduction among 53 patients who underwent laparoscopic surgery. Ackroyd et al. [25] reported a 3% conversion rate (3 of 29 cases) and the need for a mini-laparotomy in 17% (5 of 29 cases) of patients who underwent robotic interval cytoreduction.
Our 30-day perioperative outcomes are similar to published data. Our readmission rate (8.3%) is within the range of published data (5–14%) [1125].
Overall, the reported hospital stay was 2–4 days for minimally invasive surgery [11122526272830]. Our overall hospital stay was 2 days (median, 2; mean, 2.5; 95% CI, 1.27–3.73). These findings may be due to the implementation of enhanced recovery after surgery guidelines and represent a relatively shorter stay than other experiences of 5–6 days [1011242730]. In the largest study, which included 2,621 patients in the laparotomy group versus 450 cases in the laparoscopy group, the reported length of hospital stay was 5 days (range, 4–7 days) and 4 days (range, 2–6 days) for laparotomy and laparoscopy, respectively (P<0.001) [11].
Elderly patients with significant comorbidities, patients older than 80 years, and frail patients may decline open surgery, so minimally invasive surgery may be an option. In our study, patients in the robotic group tended to be older and have higher ASA scores than those in previous publications (Table 1) [12].
A recent international study from 5 centers collected data regarding 123 patients over 8 years of age with a minimum of 6 months of follow-up (3 cases per center per year). Investigators assessed the feasibility and outcomes of minimally invasive surgery after neo-adjuvant chemotherapy. A total of 122 patients (96.1%) had no residual tumors after surgery. With a median follow-up of 37 months (7–86 months), the median progression-free survival was 23 months and 5-year survival was 52% [31].
The limitations of our preliminary experience are inherent to its retrospective design and small case cohort. However, limited data exist for assessing the robotic platform in this setting [2223]. Furthermore, given the introduction of the da Vinci Xi system and widespread adoption of robotic surgery, more data are expected. We continue to collect data to assess disease recurrence and survival.
The strengths of this study include its enrollment of consecutive cases performed by the same surgical team using a standardized approach, which produced consistent, precise, and reliable data. Likewise, our focus on using the da Vinci Xi platform, which minimizes maneuvers for upper abdominal surgery, is another asset of this study.
Our preliminary data suggest that robotic-assisted surgery is an option to achieve complete interval cytoreductive surgery with similar perioperative outcomes to those of laparotomy, the gold standard approach. Prospective trials with adequate follow-up durations are needed to confirm our results as well as assess tumor recurrence and survival.
 XML Download
XML Download